Self medication is an important element of self care and defined as “the selection and use of medicine by individuals to treat self-recognized illness and symptoms” [1]. Self medication with non-prescription or over the counter (OTC) drugs are common in developing countries like India.
Young population especially students usually make unsupervised health related decisions including self medication of various drugs like analgesics, antibiotics, nutritional supplements and others [2]. Youths are highly influenced by media and internet which promotes self medication. An Indian study conducted at All India Institute of Medical Sciences, New Delhi found that self medication was considerably high among undergraduate medical students [3].
Analgesic self medication is also commonly prevalent among undergraduate medical students as pain is one of the most important suffering that compels an individual for self medication [4,5]. Analgesics, commonly known as painkillers, are substances which work in various ways to relieve different types of pain experienced in the body [6].
Acute and chronic painful conditions are often associated with sleep disturbances and vice versa is also true. Sleep disturbance can cause or modulate pain by producing hyperalgesic changes and can interfere with the analgesic treatments [7–9].
As there is paucity of literature on the analgesic self medication and its association with sleep quality among Indian medical undergraduates, the present study was hence conducted.
Materials and Methods
An observational cross-sectional study was conducted in a rural medical college situated in Rohtas district of Bihar, India among all medical undergraduate students of MBBS 1, MBBS 2, MBBS 3-I and MBBS 3-II phase. The study period was from December 2015 to February 2016.
A pre-designed semi-structured, validated, anonymous and confidential questionnaire was used to collect the relevant information pertaining to study variables. The questionnaire was prepared by collaborative efforts of Department of Pharmacology, Physiology and Community Medicine. Ethical clearance was obtained from institutional ethical committee. Cronbach’s alpha test was applied to test the reliability of the questionnaire and it was found to be 0.75. The study was conducted in different sessions by distributing questionnaires to one batch of MBBS students in one session. The students were briefed about the purpose and process of the study. They were informed that the participation would be totally voluntary. The questionnaire was distributed among the students after taking informed consents. The researchers were present during completion to clarify any doubts. Questionnaire consisted of close ended questions in english language. The questions inquired about personal and socio-demographic data, practice and pattern of self medication with analgesics such as symptoms that led to analgesic use, type of most used analgesics, most important source of information and frequency of analgesic use in last one month.
The sleep quality of students was assessed by Pittsburgh Sleep Quality Index (PSQI). The PSQI is a self-rated questionnaire which measures subjective sleep quality and disturbances over past one month and differentiate between normal and poor sleepers. In this, 19 questions are grouped into 7 components, each having score range from 0 (no difficulty in sleep) to 3 (severe difficulty). The global PSQI score was calculated and score >5 was considered as disturbed or poor sleep [10].
On completion, the questionnaires were checked for their completeness and only the completed questionnaires were accepted.
Statistical Analysis
The data was reviewed, organised, tabulated and analyzed by SPSS Version 17.0. The qualitative variables were expressed as percentages. Where appropriate, Odds Ratio (OR) with 95% confidence interval (CI) was also calculated. Chi-square test was used and values of p< 0.05 were considered as statistically significant. Some questions containing multiple responses by study subjects and hence the sum of percentages is not always 100%.
Results
Out of 320 MBBS students present on the days of interview, a total of 308 responded to the questionnaire with complete answers, giving a response rate of 96.25%. The age range of students was 17 to 30 years, with a mean age of 21.4±1.85 years. The prevalence of analgesic self medication was 49.7% (n=153) of the respondents. A proportionately larger number of males were self medicating (54.2%; 83/153) than females (45.8%; 70/153) although the difference was non-significant.
The students were divided into two age groups by an age cut-off of 19 years, as the adolescents (10-19years) are more vulnerable to do high risk practices like self medication. Self medication was significantly higher in age group ≥ 20 years as compared to age group ≤19 years (adolescents). Students of urban residence (51.9% vs 34.8% in rural) and those whose mothers were in service (57.1% vs 46.2% in housewives) were more involved in self medication with analgesics [Table/Fig-1].
Socio-economic factors and utilization of analgesic self medication (N=308).
| Characteristics | Self Medication with analgesic | χ2 (p) | OR (95% CI) |
|---|
| Yes(n=153) | No(n=155) | TotalC |
|---|
| No. | % | No. | % |
|---|
| Age |
| ≤ 19 years | 11 | 30.6 | 25 | 69.4 | 36 | 5.96 (0.0146)* | 1 |
| ≥ 20 years | 142 | 52.2 | 130 | 47.8 | 272 | 2.48 (1.17-5.24) |
| Sex |
| Males | 83 | 54.2 | 93 | 52.8 | 176 | 1.04 (0.3078) | 1 |
| Females | 70 | 45.8 | 62 | 47.0 | 132 | 1.26 (0.80-1.98) |
| Study Year |
| MBBS 1 | 29 | 43.3 | 38 | 56.7 | 67 | 1.45(0.693) | 1 |
| MBBS 2 | 41 | 50.6 | 40 | 49.4 | 81 | 1.34 (0.70-2.57) |
| MBBS 3-I | 43 | 52.4 | 39 | 47.6 | 82 | 1.44 (0.75-2.76) |
| MBBS 3-II | 40 | 51.3 | 38 | 48.7 | 78 | 1.37 (0.71-2.65) |
| Residence |
| Urban | 136 | 51.9 | 126 | 48.1 | 262 | 4.59(0.032)* | 2.02 (1.05-3.88) |
| Rural | 16 | 34.8 | 30 | 65.2 | 46 | 1 |
| Father’s Occupation |
| Service | 145 | 49.7 | 147 | 50.3 | 292 | 0.71(0.972) | 0.98 (0.36-2.69) |
| Others | 8 | 50.0 | 8 | 50.0 | 16 | 1 |
| Mother’s Occupation |
| Service | 56 | 57.1 | 42 | 42.9 | 98 | 3.21(0.073) | 1.55 (0.95-2.51) |
| Housewife | 97 | 46.2 | 113 | 53.8 | 210 | 1 |
*Significant; χ2: Chi Square; OR: Odds Ratio; 95% CI: 95% Confidence Interval
The most frequently reported symptom for self medication was headache (48.4%), followed by cough, cold and fever (44.4%) and bone and joint pain (39.9%). Among females, 84.3% were taking analgesic self medication for dysmenorrhoea. Nearly 21% of students were taking analgesics for general well being in absence of any pain [Table/Fig-2].
Reported symptoms as a cause of analgesic self medication (N=153).
| Types of symptoms/ illness | Frequency | Percentage | 95% CI |
|---|
| Headache | 74 | 48.4 | 40.6- 56.2 |
| Cough/ Common Cold/ Fever | 68 | 44.4 | 36.8- 52.3 |
| Bone and Joint Pain | 61 | 39.9 | 32.4- 47.8 |
| Dysmenorrhoea (N=70)* | 59 | 84.3 | 74.0- 91.0 |
| General well being | 32 | 20.9 | 15.2- 28.0 |
| Non-specific pain | 24 | 15.7 | 10.8- 22.3 |
*Only females
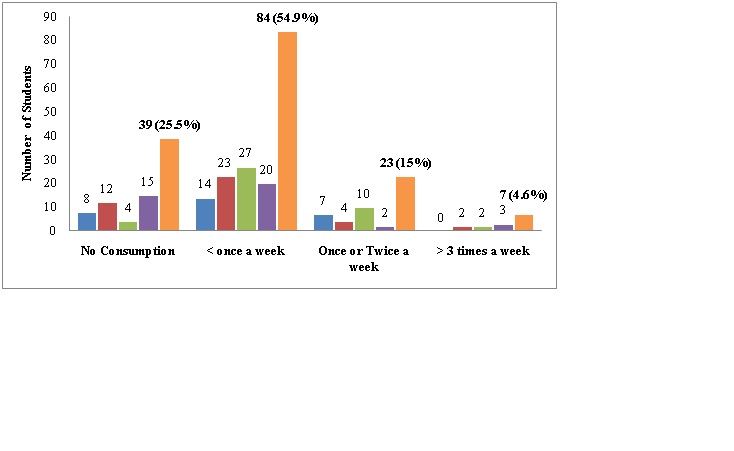
The frequency of analgesic use was ‘less than once a week’ in 84 (54.9%), ‘once or twice a week’ in 23 (15%), ‘more than three times a week’ in 7 (4.6%) and no intake in 39 (25.5%) students in past one month [Table/Fig-3].
Recent pattern of analgesic self medication in last one month (N=153).
Paracetamol (79.7%) was the most common self medicated analgesic used by students followed by fixed dose combinations of paracetamol and NSAIDs like Ibuprofen and diclofenac (70.6%) [Table/Fig-4].
Types of analgesics used as self medication (N=153).
| Types | Frequency | Percentage | 95% CI |
|---|
| Paracetamol only | 122 | 79.7 | 72.7- 85.3 |
| NSAIDs only | 67 | 43.8 | 36.2- 51.7 |
| Fixed dose combinations | 108 | 70.6 | 62.9- 77.2 |
| Opioids / Opioid like | 6 | 3.9 | 1.8- 8.3 |
The most common source of information about analgesics by students was through self obtained academic knowledge from textbooks and internet (47.1%), followed by advice from seniors/ friends/ family (19.6%) and chemist recommendation from drug stores (13.7) [Table/Fig-5].
Sources of Information about analgesics self medication (N=153).
| Source | Frequency | Percentage | 95% CI |
|---|
| Self knowledge (Textbooks and Internet) | 72 | 47.1 | 39.3- 54.9 |
| Previous prescriptions by doctors | 14 | 9.1 | 5.5- 14.7 |
| Chemist recommendation | 21 | 13.7 | 9.2- 20.1 |
| Advertisement | 12 | 7.8 | 4.5- 13.2 |
| Advice from Seniors/ Friends/ Family | 30 | 19.6 | 14.1- 26.6 |
| Other sources | 4 | 2.7 | 1.0- 6.5 |
When inquired about most important reason for self medication, 49.1% of the students responded that their illnesses were too trivial for consultation, followed by other reasons like lack of time (20.3%), previous experience (15%), self diagnosis (7.8%), privacy (5.9%) and others (1.9%) [Table/Fig-6].
Reason for analgesics self medication (N=153).
| Reason | Frequency | Percentage | 95% CI |
|---|
| Illness too trivial for consultation | 75 | 49.1 | 41.2- 57.0 |
| Lack of time for consultation/ urgency | 31 | 20.3 | 13.9- 26.7 |
| Previous experience | 23 | 15.0 | 9.3- 20.1 |
| Confidence in self diagnosis | 12 | 7.8 | 3.5- 12.0 |
| Privacy | 9 | 5.9 | 2.2- 9.6 |
| Other reasons | 3 | 1.9 | -0.3- 4.0 |
In this study we analysed the sleep quality of students using PSQI and its association with analgesic self medication. Out of 308 students, 122 (39.6%) were classified as “poor sleepers” having global PSQI score >5 and 186 (60.4%) were classified as “normal sleepers” having a global PSQI score ≤5. The use of analgesics self medication was proportionately more (57.4%) among “poor sleepers” compared to “normal sleepers” (45.2%) and this difference was statistically significant [Table/Fig-7].
Association between sleep quality and analgesic self medication (N=308).
| Sleep Quality | Analgesic use | Total | χ2(p) | OR(95% CI) |
|---|
| Yes | No |
|---|
| N (%) | N (%) |
|---|
| Poor sleepers (PSQI Score > 5) | 70 (57.4) | 52 (42.6) | 122 | 4.40(0.036)* | 1.63(1.03-2.59 |
| Normal sleepers (PSQI Score ≤ 5) | 84 (45.2) | 102 (54.8) | 186 | 1 |
*Significant; σ2: Chi Square; OR: Odds Ratio; 95% CI: 95% Confidence Interval
Discussion
As per WHO, self medication is a selection and use of medicines by individuals to treat self recognized illnesses or symptoms [11]. Many studies done before have shown prevalence rate of self medication ranging from 45-90% [12,13]. In India most of the common illnesses are treated by self medication due to easy availability of non prescription drugs and it is also becoming a routine practice among undergraduate medical students which creates a hurdle in the path of safe and effective use of medicines [14,15].
In this study, the prevalence of analgesic self medication was 49.7%. Similar studies done on medical students in India showed prevalence of analgesic use ranging from 23%-90% [4,13,16]. However, studies done in other countries on medical students showed prevalence of analgesic self medication as 73.2% in Nepal and 55.4% in Saudi Arabia [2,17]. Although, some higher rates (81.3%) were reported by Bahrain University students and 76.6% in Iranian University students [15,18]. These variations are difficult to compare due to differences in socio-demographic characteristics of the study population, study design and measurement time frame of study.
This study showed a higher proportion (54.2%) of analgesic self medication in male students as compared to female students (45.8%) although it was non-significant. Similar observations were seen in other studies [19–21]. Although some studies showed higher prevalence in females [12,16,22,23].
According to theories given by Hargreave et al., the gender differences in analgesic consumption depends upon ‘sex-roles’, ‘social support, ‘stress level’ and ‘biological differences’ related to women’s reproductive life [24].
The prevalence of use of analgesic self medication was higher among students aged ≥ 20 years compared to age group ≤19 years. Similar study in Serbian students showed older students self medicated more than younger and for each year of age; there was about 1.13 times more chance to self medicate [23].
Senior batches are more exposed to subjects like medicine and pharmacology which might have increased their knowledge and confidence to self medicate with analgesics as shown by Ibrahim NK et al., [2]. Although the prevalence was more in higher age group, the prevalence among adolescents was still 30.6%. It is an important finding considering the vulnerability of this age group towards high risk behaviours. A systemic review by Shahnaz SI et al., showed self medication prevalence range of 2% to 92% among adolescents in different countries [25].
The prevalence of analgesic self medication was lower (43.3%) among 1st year MBBS students as compared to 3rd year students (52.4%), as shown by other studies which may be due to their increased clinical exposure [15,16,26]. A study done in Gujarat on medical students showed that 2nd year medical students tend to have greater knowledge of appropriate self medication, have a more confident and concerned attitude towards self medication, and tend to practice it more often [27].
Students of urban residence were more involved in analgesic self medication probably due to their exposure to over the counter drugs at a younger age and easy accessibility of drug stores in urban areas. Parental use of analgesics to combat work related illnesses might have an influence on self medication practices of their children. Also, children of working parents are more vulnerable to unsupervised use of medicines. Ibrahim NK et al., also showed in their study that prevalence of analgesic self medication was more in students whose mothers were involved in professional occupation [2].
Headache followed by cough, cold and fevers were the most commonly reported symptoms behind the use of analgesics which is similar to other studies [13–16,19,22]. Kaur et al., found an association of insomnia along with headache as an important cause for self medication [28].
However, among females dysmenorrhoea was also an important cause of analgesic self medication apart from headache [18]. It was noted that 21% of the students were using analgesics for general well being in absence of any pain, a similar proportion (25%) seen in a study done by Sai D et al., pain free intervals due to analgesic use during actual illnesses might have driven students to use analgesics for general well being [29].
Paracetamol was the most common analgesic used by students followed by fixed dose combinations of paracetamol and NSAIDs like ibuprofen and diclofenac. Other studies have also shown paracetamol as the most common self medicated analgesic [18,30]. This is because most of the commercial brands of analgesics contain paracetamol. Also, it has favourable side effect profile and used as a first line analgesics for day-to-day pain.
Recent pattern for use of analgesic self medication shows that in most of the students, the frequency of analgesic use was ‘less than once a week’ over past one month. However, use of analgesics ‘more than three times a week’ was seen more in seniors. A different frequency pattern was observed by Sarahroodi S et al., in an Iranian study, probably because of variability in study population [18].
The study group mentioned the most common source of information for analgesic self medication as academic knowledge gained through textbooks and internet, followed by advice by seniors and chemist recommendation. This is comparable to previous conducted studies [13,14]. On the contrary, other studies revealed source of information as previous prescriptions by doctors [16,31], seniors, family and friends [18,19].
Most common reason for analgesic self medication in this study was minor nature of illnesses followed by urgency of the condition or lack of time to consult, previous experience with self medication, self diagnosis and privacy (especially for females). Studies done by different authors have shown similar results [12,15,16,19,30].
Lukovic JA et al., suggested many risk factors to increase the self medication such as less physical activity, depression, consumption of alcohol, tobacco and drug addiction. Patient Health Questionnaire-9 (PHQ-9) was used to assess depressive symptoms and showed that self medication was higher among students having significant higher depressive symptoms [23]. Sleep disruptions may contribute to increases in depressive symptoms via their impact on cognitive control. Improving sleep quality may prevent the development of depressive symptoms and reduce the likelihood of suicidal ideation [32,33].
In this study, assessment of sleep quality was done using PSQI score. A 39.6% of students scored >5 on PSQI, indicating poor sleep quality. A lithuanian survey showed a relatively higher prevalence of 59.4% poor sleepers among total university students though medical students had the highest prevalence of poor sleep compared to other non-medical students [34].
A study in India showed relatively higher percentage (72.9%) of medical students having poor sleep quality in comparison to non-medical (51.9%) [35]. Studies in other countries have shown a range of 51-59% prevalence of poor sleep among college students [36–38]. However, in a Chinese study, only 19% of the medical students was found to have poor sleep quality [39].
We found a significant association between poor sleepers and analgesic self medication in this study. Hectic class schedules and altered study habits of medical students predispose them to sleep disturbances. General fatigability and myriad of pain symptoms produced due to sleep disturbances can affect the pattern of analgesic self medication among medical students.
Disturbances or deprivation of sleep affects pain modulation. Pain can alter sleep continuity and sleep architecture by inducing arousal and triggering neurobiological sequels of stress. Hence, a vicious cycle might arise starting either with disturbed sleep or with pain in which the two components maintain or even augment each other. Accordingly, sufficient management of disturbed sleep might alleviate pain. On the other hand better pain relief may promote more restorative sleep, which then further assists in long-term pain relief [7–9,40].
Conclusion
A significant number of students practiced self medication with analgesics, most commonly paracetamol and combinations with NSAIDs. A significant association was observed between students having poor sleep quality and analgesic self medication. Physical and mental burden due to hectic academic load results in fatigability, altered pain perception and poor sleep that might affect the self medication behaviour of medical students.
Although responsible analgesic self medication practices as a part of self care is an easy and effective way to treat mild to moderate pain, students should be made aware of the potentially dangerous side effects, drug interactions and toxicity. Educational awareness programmes about concepts and principles of self medication and healthy sleep habits should run parallel to academic curricula. There is also an urgent need to form a stricter drug policy by concerned health authorities to curb the peaking trend of analgesic self medication among youth.
*Significant; χ2: Chi Square; OR: Odds Ratio; 95% CI: 95% Confidence Interval
*Only females
*Significant; σ2: Chi Square; OR: Odds Ratio; 95% CI: 95% Confidence Interval