Open Reduction and Volar Plate Fixation of Dorsally Displaced Distal Radius Fractures: A Prospective Study of Functional and Radiological Outcomes
Arjun Ballal1, Anand Kumar Sadasivan2, Anoop Hegde3, Ashwin Shetty4
1 Registrar, Department of Orthopaedics, ARS Hospital, Tirupur, Tamil Nadu, India.
2 Consultant and Chief Orthopaedic Surgeon, Department of Orthopaedics, ARS Hospital, Tirupur, Tamil Nadu, India.
3 Registrar, Department of Orthopaedics, ARS Hospital, Tirupur, Tamil Nadu, India.
4 Associate Professor, Department of Orthopaedics, K.S. Hegde Medical Academy, Mangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Arjun Ballal, 6/53, 6th Street Thennampalyam Extension, Palldam Road, Tirupur-641604, Tamil Nadu, India.
E-mail: 5arjunballal@gmail.com
Introduction
The fractures of the distal radius have always posed a unique challenge to the orthopaedic fraternity. The complex ligamentous and bony anatomy offers a wide variety of fractures to be dealt with around this zone. Over the years these injuries have become common especially in the elderly age group as well as the implants and surgical techniques have improved.
Aim
To assess the radiological and functional outcome after fixation of intra-articular dorsally displaced distal radius fractures with open reduction and volar Locking Compression Plate fixation (LCP). To study the complications occurring with this technique.
Materials and Methods
A prospective study was conducted in the Department of Orthopaedics at ARS Hospital, Tirupur, Tamil Nadu, from June 2015 to June 2016. A total of 20 skeletally mature patients with Lidstrom class 2D and 2E fresh closed distal radius fractures were enrolled in the study. All the patients underwent open reduction with locking compression plating with titanium LCPs using the volar approach. The patients were reviewed regularly at three, six, 12 and 24 weeks. Final assessment of radiographic fracture union was done and scored as per the ‘Radiographic Scoring System to Evaluate Union of Distal Radius Fractures {Radius Union Scoring System (RUSS)}’ and the functional assessment of the wrist was done using the Mayo wrist score. The final results were tabulated and calculated statistically using ‘frequency and proportions’ and ‘Chi-square tests’ were used to assess the test of association.
Results
Of the 20 patients reviewed, one patient had excellent Mayo wrist score, five had good scores, 12 had satisfactory and two patients had poor results. Seven patients had a RUSS score less than five points and four patients had RUSS score of five points, four patients had six points, two patients had seven points and three patients had eight points. One patient was noted to have dorsal collapse of the fracture during the final review. But, no evident of cosmetic deformity or any diminution in functional outcome of wrist was noted.
Conclusion
Open reduction and internal fixation with volar plating of dorsally displaced intra-articular distal radius fractures is an excellent technique with acceptable radiological fracture union and satisfactory functional outcome of the wrist.
Locking compression plate, Lidstrom classification, Volar approach
Introduction
Intra-articular fractures of the distal radius represent a spectrum of therapeutic challenges to the trauma surgeons over the years [1]. Dorsal angulation of the fracture is a common complication of these injuries; secondary displacement is also seen after conservative management [2]. These injuries have been noted to develop mal-union in many occasions which provide a less satisfactory functional and cosmetic outcome [3]. The distal radius forms a cornerstone for kinematics of the radiocarpal and the radioulnar joints, near normal restoration of the radial length, volar angulation and radial inclination are important pre-requisites for obtaining good wrist function [2]. Dorsal plating of dorsally displaced fractures was an option in case of patients with these injuries but, the complication rate also remained high [4,5]. Double-plating was tried in many cases of unstable distal radius fractures and several complications of loss of reduction and osteoporosis were noted [4,6]. The volar approach was then developed in management of these fractures and it had several advantages of minimizing the complications of the dorsal approach such as deprivation of metaphyseal blood supply to the fragments, avoidance of dorsal dissection and complications of extensor tendons also a more spacious volar aspect of distal radius [4,7,8]. The locking compression plates utilize a threaded screw head which locks to the plate. When tightened, the angular and axial stability is provided which reduces screw pull-out and loosening, hence, secondary displacement is avoided for unstable fractures [7,8].
Aim
To assess the radiological and functional outcome after fixation of intra-articular dorsally displaced distal radius fractures with open reduction and volar Locking Compression Plate fixation (LCP). To study the complications occurring with this technique.
Materials and Methods
A prospective study was conducted in the Department of Orthopaedic Surgery, ARS Hospital, Tirupur, Tamil Nadu from June 2015 to June 2016. A total of 20 skeletally mature patients, between the age group of 20-65 years with fresh (maximum of 2 days after injury) Lidstrom class 2D and 2E distal radius fractures [9] were enrolled into the study after obtaining consent from the patients [Table/Fig-1]. Extra-articular fractures, volar displaced fractures, diaphyseal extension of the fractures, fractures with associated neurovascular injury, associated ulna fractures or other wrist and hand injuries (both bony and soft tissue), open fractures, pathological fractures, old fractures, severe comminution with ≥= 5 articular fragments were excluded from the study. The patients were taken up for the study after complete medical fitness.
Plane x-rays antero-posterior and lateral views of the left wrist showing Lindstron class 2E type of distal radius fracture.

Surgical technique
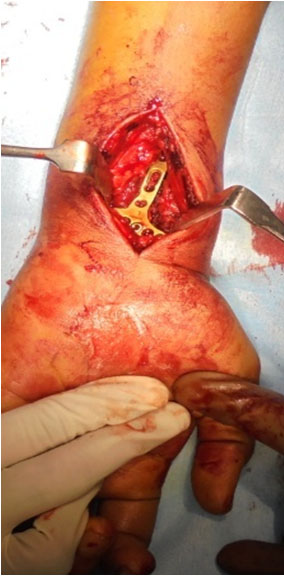
All surgeries were performed under regional or general anaesthesia under fluoroscopic guidance. With the patient positioned on the operating table, the skin incision was made after palpating the Flexor Carpi Radialis tendon (FCR) [Table/Fig-2]. The sheath of FCR was split and the FCR was retracted ulnar-ward. The interval was developed between the FCR tendon and the radial artery. The Pronator Quadratus (PQ) was exposed and incision was made over the radial border of the PQ. The fracture site was exposed and the periosteum was elevated using a periosteal elevator. The fracture was the reduced using a volar and ulnar directed force with traction being applied. In some cases a temporary Kirschner wire (K-wire) was inserted through the fracture site from the radial styloid. An appropriate sized titanium distal radius LCP was selected depending on the fracture pattern [Table/Fig-3]. The plate was fixed under the guidance of the image intensifier and the articular reduction was maintained with titanium subchondral screws [Table/Fig-4,5]. The skin was closed in layers after a thorough wash. A dorsal slab was applied in all cases and was maintained for a period of three weeks Post-operative. Post-operative radiographs were taken [Table/Fig-6a,b]. The patients were then reviewed at post-operative weeks 3, 6, 12 and 24. Antero-posterior and lateral radiographs were taken during all the reviews, the slab was removed at week 3 and wrist mobilization in terms of range of motion exercises and soft ball exercises to improve grip strength were started at week 3. During the final review at Post-operative week 24 the final scoring of wrist function was done using the Mayo wrist score and the radiological union of the fracture was scored using the ‘Radiographic Scoring System to Evaluate Union of Distal Radius Fractures (RUSS)’ [10] [Table/Fig-7]. The results were tabulated and analysed statistically using frequency and proportions and Chi-square tests were used to assess the test of association.
Intraoperative image after skin incision and exposure of the FCR tendon (marked by the yellow arrow) and release of the sheath of FCR.

Titanium locking compression plate used for fixation of all our cases.

Intraoperative image after placement of LCP after open reduction of the fracture.
Intraoperative fluoroscopic image after fixation with LCP.

Antero-posterior and lateral radiographs showing left wrist after open reduction and volar LCP fixation. A dorsal plaster of paris slab was applied and was removed at two weeks.

Anteroposterior and lateral radiograph showing left wrist during the final review at six months showing uniting fracture. RUSS score three.

Results
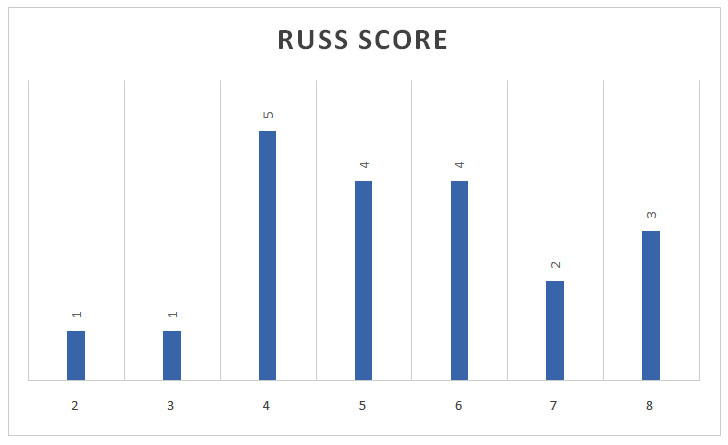
The age group distribution of patients under the study showed four(20%) patients, between 20-30 years, three patients (15%) between 30-40 years, six patients between 40-50 years and four patients (15%) between 50-60 years and three patients (15%) from 60-65 years. Gender distribution noted 15 patients (75%) of the 20 to be males and five patients (25%) to be females. Twelve (60%) of the 20 distal radius fractures taken under the study belonged to the Lidstrom class 2D and eight (40%) patients belonged to Lidstrom class 2E. Seven patients had a RUSS score less than five points and four patients had RUSS score of five points, four patients had six points, two patients had seven points and three patients had eight points during the final review at 24 weeks [Table/Fig-8].
Bar graph showing the distribution of patients as per the RUSS score. X-axis indicating the points of the RUSS score and Y-axis indicating the distribution of patients. Note that there were seven patients below the score of five points and four patients scored five points, four scored six, two scored seven and three patients scored eight points.
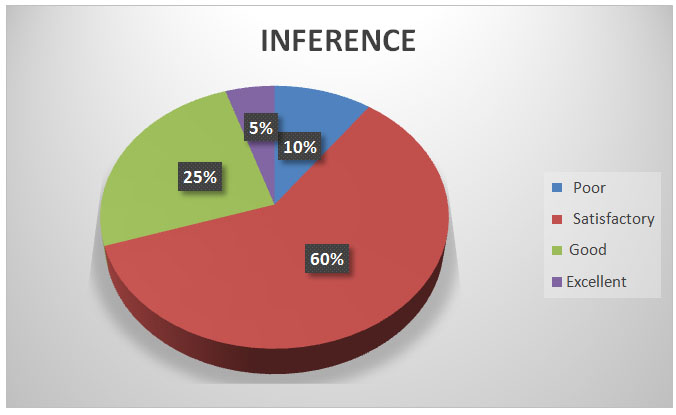
The inference from the Mayo wrist score showed ‘Excellent’ results for one patient (5%), five had ‘good’ (25%), 12 patients (60%) had ‘satisfactory’ and two patients (10%) had ‘poor’ results [Table/Fig-9]. One patient presented with ‘dorsal collapse’ of the fracture as a complication during the final review at 24 weeks, but he had satisfactory functional outcome with no evident cosmetic deformity, hence no secondary procedures were performed. No other complications of infection, mal-union, non-union etc., were noted.
Pie diagram indicating the distribution of patients as per the inference of the Mayo wrist score. The inference from the Mayo wrist score showed ‘Excellent’ results for one patient(5%), five had ‘good’(25%), 12 patients(60%) had ‘satisfactory’ and two patients(10%) had ‘poor’ results.
Discussion
The older teachings for surgical management of distal radius fractures relied on the fact that the surgical approach should depend on the direction of the fracture displacement [2]. The biomechanical stability offered by the dorsal plate was considered effective as compared to the volar plating [2]. Leung et al., in a cadaveric study concluded that no statistical difference was present in axial load transmission in case of a volar plate fixation of an unstable fracture and of that of an intact radius [8]. He also presented advantages of the volar approach over the dorsal approach [8]. The dorsal approach requires dissection of the extensor retinaculum with resection of the Lister’s tubercle. The exposure of the extensor pollicis longus tendon is therefore done due to mechanical attrition by the implant [2]. The volar approach provides advantages of providing a spacious zone for placement of the implant also the PQ acts as a barrier protecting the flexor tendons from irritation [2]. The comminution of the volar cortex is not as much as the dorsal cortex, hence, there is more room for adequate and accurate reduction, which also reduces the incidence of radial shortening [8]. The anatomical flat contour of the volar cortex is an added advantage for implant placement [2]. The locking plate provides an advantage of providing an inherent angular stability as the implant construct provides a single unit to hold and support the fragments [2]. Hence, a perfect alignment of the implant to the distal radius is not necessary and hence the periosteal blood supply is maintained which aids fracture union [2].
Radiographic scoring system to evaluate union of distal radius fractures or RUSS is a scoring system developed for assessment of the Post-operative radiographic union of distal radius fractures [10].
The age distribution of majority of our patients was between 40-60 years with a mean age of 45 years; this is comparable to the results of Wong and colleagues who reported a mean of 58.6 years [2]. Majority of our patients had RUSS scores over 5 points; this indicated an excellent to good union of the fracture after volar plating. These results are comparable to those of Wong and colleagues who presented an excellent to good results in terms of radiological union of the fracture in their series [2]. Mayo wrist score showed majority of the patients with excellent to good results. These results were comparable to those of Wong and colleagues [2] who reported excellent to good results in their series.
Wong and colleagues in their series of 30 patients with displaced distal radius fractures concluded that application of volar plate in dorsally displaced fractures of the distal radius brought about good radiological union of the fracture and functional outcome of the wrist with minimal complications [2].
Orbay and Fernandez in their series of 31 dorsally displaced fractures concluded that volar fixation of dorsally displaced fractures led to preservation of soft tissue, blood supply, reduced tendon related problems, reduced need for bone grafting hence minimizing complication rates [11].
Fok and colleagues concluded in their series that irrespective of the direction and amount of initial displacement of the distal radius fracture single approach volar plating could be employed with satisfactory results [1]. Othman reported good to excellent results in 88% of the 17 patients with distal radius fractures who underwent volar locking plate fixation [12].
Limitation
The sample size of the study was 20 as only 20 patients agreed to get enrolled into the study. The follow-up of the study was only for 6 months.
Conclusion
Open reduction and internal fixation with volar plating of dorsally displaced intra-articular distal radius fracture is a good technique with acceptable fracture union and satisfactory functional outcome of the wrist and minimal complication rates.
[1]. Fok MWM, Klausmeyer AM, Fernandez LD, Orbay LJ, Bergada LA, Volar plate fixation of intra-articular distal radius fractures: a retrospective studyJ Wrist Surg 2013 2:247-54. [Google Scholar]
[2]. Wong KK, Chan KW, Kwok TK, Mak KH, Volar fixation of dorsally displaced distal radial fracture using locking compression plateJournal of Orthopaedic Surgery 2005 13(2):153-57. [Google Scholar]
[3]. Arora R, Lutz M, Deml C, Krappinger D, Haug L, Gabl M, A prospective randomized trial comparing nonoperative treatment with volar locking plate fixation for displaced and unstable distal radial fractures in patients sixty-five years of age and olderJ Bone Joint Surg Am 2011 93(23):2146-53. [Google Scholar]
[4]. Swan K Jr, Capo JT, Tan V, Distal radius plating optionsCurr Opin Orthop 2003 14:238-44. [Google Scholar]
[5]. Campbell DA, Open reduction and internal fixation of intra-articular and unstable fractures of the distal radius using the AO distal radius plateJ Hand Surg Br 2000 25:528-34. [Google Scholar]
[6]. Jakob M, Rikli DA, Regazzoni P, Fractures of the distal radius treated by internal fixation and early function. A prospective study of 73 consecutive patientsJ Bone Joint Surg Br 2000 82:340-44. [Google Scholar]
[7]. Chan KW, Kwok TK, Mak KH, Early experience with locking compression plate in the treatment of distal radius fractureHong Kong J Orthop Surg 2003 7:88-93. [Google Scholar]
[8]. Leung F, Zhu L, Ho H, Lu WW, Chow SP, Palmar plate fixation of AO type C2 fracture of distal radius using a locking compression plate: a biomechanical study in a cadaveric modelJ Hand Surg Br 2003 28:263-66. [Google Scholar]
[9]. Lidstrom A, Fractures of the distal end of the radius. A clinical and statistical study of end resultsActa Orthop Scand Suppl 1959 41:1-118. [Google Scholar]
[10]. Patel SP, Anthony SG, Zurakowski D, Didolkar MM, Kim PS, Wu JS, Radiographic scoring system to evaluate union of distal radius fracturesJ Hand Surg Am 2014 39(8):1471-79. [Google Scholar]
[11]. Orbay LJ, Fernandez LD, Volar fixation for dorsally displaced fractures of the distal radius: a preliminary reportThe Journal of Hand Surgery 2002 27A(2):205-15. [Google Scholar]
[12]. Othman AY, Fixation of dorsally displaced distal radius fractures with volar plateJ Trauma 2009 66(5):1416-20. [Google Scholar]