Introduction
Pediatric fractures hold special attention owing to the fact that bones in this age group have an enormous growth as well as remodeling ability. Long term functional outcome and radiological appearance of a fracture treated in pediatric age group may be quite different from the immediate post-management status. Neurovascular complications associated with this fracture make it an orthopaedic emergency thus, understanding of this fracture is extremely important.
Supracondylar fracture of the humerus is one of the most talked about and often encountered injury (only after clavicle and both bone forearm fracture) in pediatric age group with a male predominance accounting for 16% of all pediatric fractures and 60% of all pediatric elbow fractures, classically occurring as a result of fall on an outstretched hand [1-3]. Immediate complications associated with it are limb threatening (by virtue of involving neurovascular structures) whereas late complications are a serious concern to functional status of the patient. Due to the above reasons they require a strict vigilance and a proper management protocol. In pediatric age group the more common age of presentation is 5-7 years (90% cases). Extension type injury is more common than flexion type [4]. It is frequently found in the non-dominant extremity. The flexion type is common in elderly children [5]. Certain studies have reported up to 30% incidence of open fractures in this subset of patient [6].
Pertinent Anatomy
Bone – In children, the supracondylar region consists of a weak, thin bone located in the distal humerus. This area is bordered posteriorly by olecranon fossa, anteriorly by coronoid fossa and on both sides by respective supracondylar ridges. The medial and lateral supracondylar ridges end into respective condyles and epicondyles. The trochlea is normally tilted 4° valgus in males and 8° valgus in females (carrying angle). The trochlea is also 3-8° externally rotated, resulting in external rotation of the arm when is flexed to 90° [2,7].
Soft tissue structures – Both supracondylar ridges, condyles and epicondyles give rise to attachment of various muscles which are responsible for the displacement and rotation of distal fragment. Neurovascular structures lie in proximity to supracondylar region. Brachial artery which commonly gets involved in supracondylar fracture of humerus lies along the antero-medial aspect of distal humerus just superficial to the brachialis muscle. Major neurological structures of the upper limb (median, radial and ulnar nerves) are also in close relation with supracondylar region [2].
Pathoanatomy
The ossification process of distal humerus occurs at different ages. The first to appear is capitulum at 1 year of age. The radial head and medial epicondyle begins to ossify at 4-5 years of age, followed by trochlea and olecranon epiphysis at 8-9 years of age. The lateral condyle is generally the last to appear at approximately 10 years of age. The supracondylar area undergoes remodeling between 6 to 7 years of age and is typically thinner with a more slender cortex, predisposing this area to fracture. As elbow forced into extension, the olecranon serves as a fulcrum and focuses the stress on the distal humerus causing fracture [8].
Approach To a Case
History – In a case where there is a classical history of fall on an out stretched hand followed by pain and swelling over the elbow with loss of function of upper limb, onset of pain holds special consideration. It is of utmost importance to ascertain whether the pain is due to fracture or because of muscle ischemia which has a late onset (hours after the injury).
Clinical examination – Initial gross assessment should be aimed to rule out any associated systemic trauma and neurovascular involvement. The clinical presentation is that of a painful swollen elbow that the patient is hesitant to move, when a patient history includes a high energy trauma or a significant fall. Urgent orthopaedic review in Emergency Department is indicated in the following circumstances: when there is absence of radial pulse, ischaemia of hand (pale and cool extremities); severe swelling in forearm and or elbow, skin puckering or anterior bruising, open injury and neurological injury [9].
Both radial and ulnar pulses must be palpated at the wrist of injured extremity. In case of pulselessness, other signs of perfusion must be checked viz., color (the hand should be pink), temperature, capillary refill and oxygen saturation on pulse oximeter. Ultrasound with Doppler flow should be performed in children with evidence of vascular injury (e.g., decreased or absent radial pulse) [8].
If a neurological involvement is noted, it warrants a careful evaluation and documentation such as when it first became apparent, the degree of involvement and possible progression/ regression of symptoms.
The median nerve along with the brachial artery crosses the elbow joint. Anterior Interosseous Nerve Branch (AION) of the median nerve is most prone to get involved in postero-lateral displacement of the distal fracture fragment [10].
AION syndrome in children and adolescents most of the time present with proximal forearm pain followed by weakness in the hand without any sensory deficit. A weak "OK sign" (e.g., more of a pincer grasp than an OK sign) can be elicited on physical examination. The radial nerve runs between the brachialis and brachioradialis muscles before crossing the elbow and penetrating the supinator muscle. Radial nerve impingement most commonly occurs when the distal fracture fragment is displaced postero-medially. This occurs because the proximal fracture fragment is displaced laterally. The ulnar nerve is prone to injury following flexion type of supracondylar fractures as the nerve crosses the elbow posterior to the medial epicondyle. If a neurological/vascular involvement appears following manipulation or splint placement, one must consider immediate re-manipulation. Neuropraxias are not uncommon and generally resolve with restoration of normal alignment and lengths.
A puckered, dimple and/or ecchymosis of the skin just anterior to the distal humerus may be suggestive of a difficult reduction probably due to the fact that the proximal, anteriorly directed fragment has penetrated the brachialis muscle and possibly the subcutaneous layer as well [8].
Radiographic Assessment- The standard radiographic study of the injured limb should include an Antero-Posterior (AP) and a lateral view of the elbow and any other sites of deformity, pain, or tenderness. Because of the association of supracondylar fractures with forearm fractures, the clinician should also obtain AP and lateral radiographic views of the forearm [11]. Radiographs should be obtained only after appropriate analgesia and splintage of the extremity so as to avoid any neurovascular injury or its exacerbation by the fractured fragments. Idea of splintage is to provisionally stabilize the limb and it should be done in a position of comfort (approximately 20°–30° of flexion) [12]. Splinting in displaced or unstable fractures with elbow in full extension or hyper-flexion is contraindicated because it stretches the neurovascular bundle over the fracture site or they may get impinged between fractured fragments [13].
The carrying angle (the varus or valgus attitude of the distal humerus and elbow) is evaluated on AP view by looking at Baumann’s angle. Radiographs of the contralateral elbow should be used for comparison, if needed, as the Baumann’s angle varies among all individuals [14].
On the lateral view, the following radiological parameters are looked for: (a) Anterior humeral line; (b) Coronoid line; (c) Fish tail sign; (d) Fat pad sign; (Anterior and Posterior) [5,15].
A positive fat pad sign (sail sign) is suggestive of occult fracture when no radiological fracture line is obvious.
Classification of Fracture Supracondylar Humerus [
16]
Fractures of supracondylar humerus may be classified in a number of ways as per following:
a) Displaced or undisplaced fractures of supracondylar humerus
b) Open or close fractures of supracondylar humerus.
c) Uncomplicated or complicated fractures of supracondylar humerus (with/without neurological and/or vascular involvement).
d) Extension type (95%) or flexion type (5%).
e) Modified Gartland’s staging system [17] is based on the lateral radiograph and widely used for extension type supracondylar fractures to classify further as it can help to guide treatment.
Type I fracture: Undisplaced.
Type II fracture: Displaced with angulation, but maintain with an intact posterior cortex.
II A fracture: Angulation.
II B fracture: Angulation with rotation.
Type III fracture: Completely displaced and lack meaningful cortical contact, but have a periosteal hinge (either medial/ lateral) intact.
III A fracture: Medial periosteal hinge intact. Distal fragment goes posteromedially.
III B fracture: Lateral periosteal hinge intact. Distal fragment goes posterolaterally.
Type IV fracture: Have no periosteal hinge and are unstable both in flexion and extension i.e., they have multidirectional instability.
Treatment of Fractures of Supracondylar Humerus
Undisplaced (Gartland Type I) or minimally displaced fractures in children can potentially be treated with an above-elbow splint in 90° of flexion for 3 weeks [9]. Circumferential casting and extremes of flexion should be initially avoided to prevent compartment syndrome and vascular compromise [15,18-20]. While it is often easiest to visualize displacement or angulation on the lateral radiograph, but varus mal-alignment/ impaction is best depicted by Baumann’s angle on the AP radiograph. In case of varus at the fracture site of more than 10° (compared to the contralateral upper limb), closed reduction and percutaneous pinning should be strongly considered. In principle, larger diameter pins provide better stability and are more effective at maintaining fracture reduction and alignment. In a randomized trial by Ponce et al., in a study population of 50 children managed by per cutaneous pinning [20], they concluded that those immobilized initially in a posterior splint and sling returned to normal activity sooner than those immobilized in a collar and cuff sling (median two versus seven days, p≤0.01), but there is no difference between the two groups in daily pain scores or in resumption of normal activity or mobility at two weeks.
Gartland Type II fractures require close reduction [21]. Further, these may become stable after closed reduction and casting at 90° of flexion [Table/Fig-1a,b] but if more than 90° of flexion is needed to maintain reduction, then in order to minimize risks of complications associated with the increased elbow flexion, stabilization of the fracture with percutaneous pinning should be performed [Table/Fig-2a,b]. In the largest reported series by Skaggs et al., in management of Type II fractures [22], they reported an extremely low rates of complication after closed reduction and percutaneous pinning; secondary operations were also uncommon (0.5%). This series demonstrated a high probability of satisfactory outcome after operative treatment of Type II fractures compared to previous studies of children treated by closed reduction without pinning [22].
Pre-operative images showing gartland Type-II fracture.
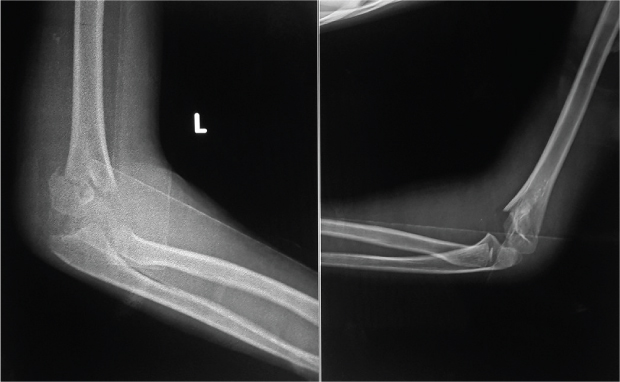
Post-Reduction images in lateral and shoot through view.
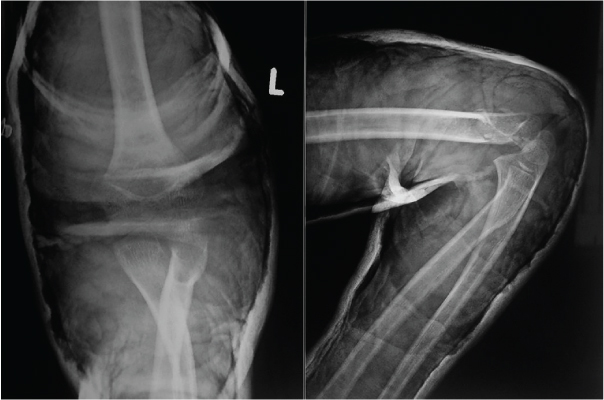
Pre-operative images showing gartland Type-II fracture.
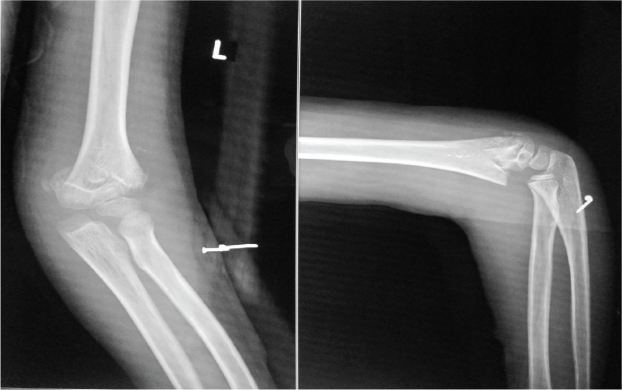
Post-operative images in lateral and AP view showing fixtion by percutaneous K –wires after close reduction.

Reduction manoeuvres for supracondylar humerus fractures: With the patient preferably under General Anaesthesia (GA) and with fluoroscopy assistance-before pounding on to anatomic reduction freeing the proximal fragment from soft-tissue entrapment is essential. First step is to apply traction in line with the humerus, with the elbow in slight flexion. Traction in full extension has to be avoided as this may cause tethering of neurovascular structures over the proximal fragment. If there is suspicion that the proximal fragment has pierced through the brachialis muscle (clinically elicited by S sign), then a persistent, gradual traction is given in slightly flexed elbow for a full minute which often gives a palpable feeling of freeing of the proximal fragment. Alternatively, the same may be achieved by proximal to distal “milking” manoeuvre over the brachialis [23].
For the reduction maneuver, it should begin with hyper-flexing the elbow while simultaneously pushing in an anterior direction on the olecranon. While keeping the elbow in hyper-flexed state fluoroscopic assessment is done with an AP image, though difficult to interpret due to overlapping of proximal ulna and radius over the fracture site. However, Jone’s view allows assessment of the continuity of the medial and lateral columns and Baumann’s angle.
Rotation of distal fragment if present can be addressed by repeating the reduction with two additional maneuvers. If the distal fragment is internally rotated (most common), to press selectively harder on the medial side during the reduction, and pronate the forearm during the reduction as well, the opposite applies for an externally rotated distal fragment. If normal range Baumann’s angle is not achieved, to repeat the reduction while stressing the arm in valgus.
Reduction maneuvers should not be attempted if the vascular status doesn’t improve after gross reduction and stabilisation in a splint. Taking decision as per appropriate use criteria [24-26] is wise in such circumstances. Cases of an open fracture, significant swelling over the elbow, vascular deficit, unstable reduction (Gartland III and IV) pose certain limitations in reduction maneuvers for supracondylar humerus fractures. In these cases one must go for open reduction as attempting close reduction may further worsen the situation.
Gartland Type III fractures are particularly prone to neurovascular compromise. The closed reduction and percutaneous pinning is the preferred treatment for displaced fractures. Fractures with displacement treated by closed reduction and casting have a higher incidence of residual deformity as compared to those managed with close/open reduction and pinning, complication rates [27-30] or the quality of the reduction [31]. However, considering it as an orthopaedic urgency, optimal management of a displaced fracture should be done by close/open reduction and percutaneous pinning preferably within 24 hours. Sadiq et al., in a review of 20 cases of grade III supracondylar fractures who were managed conservatively with straight-arm lateral traction with arm in 90° abduction and full supination showed no complication in any patient with uneventful recovery [32]. They concluded straight-arm lateral traction as a safe and effective maneuver for treating these fractures.
In a study by de Gheldere A and Bellan D, on 74 patients with Gartland Type II and III fracture managed by closed reduction and immobilization with a collar sling fixed to a cast around the wrist in order to keep forearm in pronation, they found no statistically significant difference in the final outcomes as measured by Baumann’s angle (except in posterolateral displacements) but humerocapitellar angles show statistically significant difference in Type III group [33]. The purpose of the study is to give a more precise limitation of this technique. This study suggests that Gartland Type II and pure posterior or posteromedial displaced Gartland type III fractures can be treated by closed reduction and immobilization with success, whereas Type III fractures with posterolateral displacements should preferably be fixed.
Effect of supination versus pronation in the non-operative treatment of pediatric supracondylar humerus fractures was studied prospectively by Seyed Ali MN et al., in which they concluded that considering late complication of malunion, no obvious difference was observed between the two positions of forearm after closed reduction and casting [34]. However, as cubitus varus and valgus were reported in both the groups with unstable Type III fractures, so it is advisable to prevent this complication by operative fixation.
Indications of Surgical Intervention to be Considered in the Following Conditions [
35]
If close manipulation fails to achieve the reduction.
If after close reduction fracture is unstable i.e., failure to maintain the reduction.
If neurological involvement occurs during or after the manipulation of fracture.
If vascular exploration is required.
In open fractures.
All Type II and III fractures requiring elbow flexion of more than 90° to maintain the reduction.
All Type IV fractures supracondylar humerus.
Polytrauma with multiple ipsilateral fractures requiring surgical intervention.
Ozturkmen et al., in a study on 34 children with displaced fractures of supracondylar humerus treated by close reduction and percutaneous lateral pinning observed no significant differences between the mean Baumann, humerocapitellar, and carrying angles of the normal and affected sides (p>0.05) [36]. They concluded that closed reduction and percutaneous lateral pinning proved an efficient, safe and reliable method in the treatment of displaced supracondylar fractures of the humerus in children.
In a systematic review by Brauer et al., of medial and lateral entry pinning versus lateral entry pinning for supracondylar fractures of the humerus, they observed that for operative fixation with medial/lateral entry pins, probability of ulnar nerve injury is 5.04 times higher than the lateral entry pins alone [37]. When all documented operative nerve injuries are included, the probability of iatrogenic nerve injury is 1.84 times higher with the medial/lateral entry pins, than with isolated lateral pins. The medial/lateral pin entry provides a more stable configuration, and probability of deformity or loss of reduction is 0.58 times lower than the isolated lateral pin entry. Considering intraoperative nerve injury as a surgical technique error, it is indicated medial/lateral entry pinning of pediatric supracondylar fractures, remains the most stable configuration and that care needs to be taken regardless of technique to avoid iatrogenic nerve injury and loss of reduction.
In another systematic review of four randomized controlled trials by Yousri et al., comparing efficacy of crossed versus lateral Kirschner -wire fixation in extension type Gartland Type III supracondylar fractures of the humerus in children [38], they found no study concluding any significant statistical difference in terms of loss of reduction between the two groups, suggesting similar stability of both constructs.
In terms of approach used for open fixation of fracture supracondylar humerus, Ersan O et al., in their prospective case series of 46 children evaluated the effectiveness and safety of using an anterior approach to address these fractures and concluded that it is a safe and reliable method with very good results [39]. In another study of 84 patients who underwent open reduction and Kirschner wire (K-wire) fixation through anterior or lateral approach were compared with regard to complications and end results with the conclusion that anterior incision offers the advantage of a smaller scar and easy access to structures that might be injured between the fractured fragments. Medial approach and cross-pinning for delayed surgical treatment (>24 hours) of Type III supracondylar humerus fractures is shown to be an effective and reliable treatment method by Eren A et al., in their prospective study on 30 patients [40].
Gartland Type IV fracture being a highly unstable fracture needs fixation, either close or open.
While going in for internal fixation one should be aware of the fact that in older children medial condyle sometimes remain with the proximal fragment making medial pin fixation worthless.
After management, next question which arises is that, when the patient should be called for follow up for clinical and/ or radiological assessment and when the wires should be removed for mobilization?
Study by Ponce et al., gives an answer to the above question. In their study they concluded that clinical and radiographic evaluation of routine displaced supracondylar humerus fractures requiring closed reduction and percutaneous pinning may be safely delayed until pin removal [20]. Pins were removed when the distal humerus is no longer tender, usually in 3 to 4 weeks [41] and there after active mobilization is begun.
After pin and cast removal, active range of motion exercises is recommended as tolerated. Studies on children with supracondylar fractures and no neurovascular deficit suggest that formal physical therapy does not appear to improve mobility in long term [42]. However, physical therapy is recommended for children with persistent contractures after three to four months or neurological deficits.
Complications of Supracondylar Fracture of The Humerus
Vascular Insufficiency
Absence of the radial pulse is reported in 6 to 20 percent of all supracondylar fractures [43,44]. Vascular injury evident by involvement of brachial artery is most commonly associated with Type II and III supracondylar fractures, frequently encountered in postero-laterally displaced fractures [3,45]. Patients without significant improvement in pulse after orthopaedic care, warrant emergent vascular exploration, especially if there is intractable pain, persistence of pain or increasing pain despite of fracture site stabilization which is suggestive of ischemia [3,45-49].
Griffin et al., in a systematic review of 161 children with supracondylar fractures and a pulseless hand found that closed reduction and percutaneous pinning resulted in return of the radial pulse in 51% (82 of 161) of cases [45]. A total of 63 of remaining 79 children with persistent pulseless hand after operative care underwent vascular exploration. Brachial artery injury or thrombus was found in 61 patients (97%). Mangat et al., in an observational study of 19 children who had a perfused but pulseless hand after Gartland Type III fracture concluded that in cases where there is vascular deficit along with neurological deficit (due to median/ anterior interosseous nerve involvement) [48], early exploration is recommended, as these appear to be strongly predictive of nerve and vessel entrapment at the fracture site. Those with isolated vascular deficit can be managed by closed reduction and could be observed for return of vascularity and if needed secondary exploration. Blakey et al., in an observational study of 26 children who had a pink pulseless hand, wherein 3 underwent immediate surgical exploration of vessel with good functional results and remaining 23 who presented late (four days to one year after injury) and did not have early release of brachial artery obstruction developed ischemic contractions of hand and/or forearm muscles, and thus recommended urgent exploration of the vessels and nerves in such cases not relieved by reduction of a supracondylar fracture of the distal humerus and presenting with persistent and increasing pain suggestive of a deepening nerve lesion and critical ischemia [49]. In a study of 66 children by Korompilias et al., with displaced supracondylar fractures of the humerus, they encountered 4 patients with a pink yet pulseless hand after fracture reduction. On exploration brachial artery thrombus was found in 3 [50]. Subsequent thrombectomy was performed, which led to the restoration of a palpable radial pulse. In 1 patient with open fracture, brachial artery contusion and spasm were found, and treated by removal of adventitia. They concluded that pulselessness even in the presence of viable pink hand after an attempt at closed reduction is an indication for surgical exploration of the brachial artery, to check for its patency.
Neurologic Deficit
The frequency of neurologic deficit reported after supracondylar fractures in children is 10 to 20 percent and increases in some series of children with Type III supracondylar fractures to as high as 49 percent [8,44,50-54]. Median nerve and its anterior interosseous nerve branch is at risk and gets most commonly involved in postero-lateral displacement of the distal fracture fragment, whereas radial nerve is most commonly involved with postero-medial displacement of the distal fracture fragment. Ulnar nerve injuries are commonly associated with flexion type supracondylar fractures [51,53,54].
Most often associated nerve injuries are neuropraxias that usually resolve within two to three months [8,10,54,55]. One should consider surgical exploration for nerve deficits that persist beyond three months [10,41,42,55]. Barret KK et al., in one of the largest retrospective, multicentric study conducted on 4409 patients with supracondylar fracture of the humerus presenting with anterior interosseous nerve injury (no sensory involvement) concluded that an isolated anterior interosseous nerve injury associated with this fracture in itself is not an indication for surgery [55]. In this huge series they showed complete neurological recovery in a mean time of 49 days with 90 percent of the patients recovering by 149 days.
Forearm Compartment Syndrome Resulting in Volkmann’s Ischemic Contracture
Vascular injury and primary swelling from the injury can lead to the development of compartment syndrome within 12 to 24 hours [51]. If a compartment syndrome is not treated timely, the associated ischemia may progress to infarction and subsequent development of Volkmann’s ischemic contracture: fixed flexion of the elbow, pronation of the forearm, flexion at the wrist, and joint extension of the metacarpal-phalangeal joint [51].
Malunion
One of the frequent long term complications of supracondylar fracture are angular deformities, of which cubitus varus or “gunstock” deformity is very common. The distal humerus physis, in contrast to the proximal humeral physis, contributes only 15 to 20 percent to the overall longitudinal growth of the humerus [56]. This suggests very limited remodeling in correction of fracture angulation in children with supracondylar fractures. Modern surgical techniques (e.g., closed reduction with percutaneous pinning) have reduced this frequency of cubitus varus from 58 percent to approximately 3 percent in children treated for supracondylar fractures [57]. Posttraumatic cubitus varus deformity has important problems, which are associated with tardy ulnar nerve palsy [58], tardy Postero-Lateral Rotatory Instability (PLRI) [59], and secondary distal humeral fractures [60]. Therefore, humeral osteotomy is used to correct this deformity and to avoid such later complications [61].
Eren A et al., conducted a study to evaluate the relationship between the fracture displacement and cubitus varus deformity in displaced supracondylar humerus fractures [62]. They observed that the carrying angle loss was more significant in Type III-A fractures compared with Type III-B and concluded that although anatomic reduction has been achieved by surgical treatment without loss of reduction, further there is still a risk for cubitus varus deformity for Type III-A fractures due to the initial compression of the medial column or, in other words, physical injury. Stiffness elbow-secondary to manipulation with or without development of myositis. Supracondylar fractures of the humerus are a common pediatric elbow injury that can be associated with neurovascular complications and skeletal deformity. The understanding of the anatomy, radiographic findings, complications, as well as the management options that associated with this fracture, allow physicians to limit the morbidity associated with this injury.
Conclusion
Supracondylar fracture of the humerus is a very common problem of pediatric age group and one frequently has to deal with such a fracture, with or without complication. A thorough history with a detailed clinical examination is a must. During radiographic evaluation one must not forget to verify three important points pertaining to a normal elbow: (a) On lateral view, the anterior humeral line should intersect the capitellum; (b) The head of radius should point to the capitellum in every view; and (c) Baumann’s angle must be in valgus. In treatment, we should remember that a pulseless, poorly perfused hand needs an urgent reduction, not an arteriogram. It is always safer to use K-wires to maintain the reduction in case if more than 90° of flexion is required to keep the fracture reduced as there is risk of developing compartment syndrome in holding reductions beyond 90° of flexion. Even if it is a Type II fracture, when in doubt whether to fix it or not, it is better to fix as it is safe and outcomes are good. Usage of appropriate use criteria is wise in managing these fractures as it has been quite exhaustively designed. Prognosis in case of complications or possible complications should be explained.
[1]. Cheng JC, Shen WY, Limb fracture pattern in different pediatric age groups: a study of 3,350 childrenJ Orthop Trauma 1993 7(1):15-22. [Google Scholar]
[2]. Wilkins KE, Fractures and dislocations of the elbow region. In: Rockwood CA Jr, Wilkins KE, King RE, editorsFractures in children 1991 3rd edPhiladelphiaJB Lippincott:526-617. [Google Scholar]
[3]. Skaggs D, Pershad J, Pediatric elbow traumaPaediatr Emerg Care 1997 13(6):425-34. [Google Scholar]
[4]. Mahan ST, May CD, Kocher MS, Operative management of displaced flexion supracondylar humerus fractures in childrenJournal of Pediatric Orthopaedics 2007 27(5):551-56. [Google Scholar]
[5]. Skaggs DL, Elbow fractures in children: diagnosis and managementJ Am Acad Orthop Surg 1997 5(6):303-12. [Google Scholar]
[6]. Bachman D, Santora S, Orthopedic traumaIn: Textbook of Pediatric Emergency Medicine, Fleisher GR, Ludwig S, et al. (Eds) 2006 PhiladelphiaLippincott Williams and Wilkins:1538 [Google Scholar]
[7]. Ryan LM, Bachur RG, Wiley JF, Evaluation and management of supracondylar fractures in childrenUpToDate 2009 Waltham (MA)UpToDate [Google Scholar]
[8]. Kasser JR, Beaty JH, Supracondylar fractures of the distal humerusIn: Rockwood and Wilkins’ Fractures in Children 2001 5thPhiladelphiaLippincott Williams & Wilkins:577Beaty JH, Kasser JR. (Eds) [Google Scholar]
[9]. Villarin LA, Belk KE, Freid R, Emergency department evaluation and treatment of elbow and forearm injuriesEmergency Medicine Clinics of North America 1999 17(4):843-58. [Google Scholar]
[10]. Campbell CC, Waters PM, Emans JB, Kasser JR, Millis MB, Neurovascular injury and displacement in type III supracondylar humerus fracturesJournal of Pediatric Orthopaedics 1995 15(1):47-52. [Google Scholar]
[11]. Sallay PI, Pedowitz RA, Mallon WJ, Vandemark RM, Dalton JD, Speer KP, Reliability and reproducibility of radiographic interpretation of proximal humeral fracture pathoanatomyJournal of Shoulder and Elbow Surgery 1997 6(1):60-69. [Google Scholar]
[12]. Leitch KK, Kay RM, Femino JD, Tolo VT, Storer SK, Skaggs DL, Treatment of multidirectionally unstable supracondylar humeral fractures in children. A modified Gartland type-IV fractureJ Bone Joint Surg Am 2006 88(5):980-85. [Google Scholar]
[13]. Otsuka NY, Kasser JR, Supracondylar fractures of the humerus in childrenJ Am Acad Orthop Surg 1997 5(1):19-26. [Google Scholar]
[14]. American Academy of Orthopaedic Surgeons. Guideline on the treatment of pediatric supracondylar humerus fractures 2011. http://www.aaos.org/Research/guidelines/Supracondylar Fracture/SupracondylarFracture_Guideline.asp. Retrieved 19 December 2011 [Google Scholar]
[15]. Azbug JM, Herman MJ, Management of supracondylar humerus fractures in children: Current conceptsJ Am Acad Ortho Surg 2012 20(2):69-77. [Google Scholar]
[16]. Camp J, Ishizue K, Gomez M, Gelberman R, Akeson W, Alteration of Baumann’s angle by humeral position: implications for treatment of supracondylar humerus fracturesJ Pediatr Orthop 1993 13(4):521-25. [Google Scholar]
[17]. Barton KL, Kaminsky CK, Green DW, Shean CJ, Kautz SM, Skaggs DL, Reliability of a modified Gartland classification of supracondylar humerus fracturesJournal of Pediatric Orthopaedics 2001 21(1):27-30. [Google Scholar]
[18]. Herring JA, Upper extremity injuriesIn Tachdjian’s Pediatric Orthopaedics 2008 4th EdPhiladelphiaSaunders:2451-536. [Google Scholar]
[19]. Gartland JJ, Management of supracondylar fractures of the humerus in childrenSurg Gynecol Obstet 1959 109(2):145-54. [Google Scholar]
[20]. Ponce BA, Hedequist DJ, Zurakowski D, Atkinson CC, Waters PM, Complications and timing of follow-up after closed reduction and percutaneous pinning of supracondylar humerus fractures: follow up after percutaneous pinning of supracondylar humerus fracturesJ Pediatr Orthop 2004 24(6):610-14. [Google Scholar]
[21]. Clifford R. Wheeless. Wheeless’ Textbook of Orthopaedics. (http://www.wheelessonline.com/ortho/reduction_supracondylar_fractures) Last assessed on 11 Sep 2015 [Google Scholar]
[22]. Skaggs DL, Sankar WN, Albrektson J, Vaishnav S, Choi PD, Kay RM, How safe is the operative treatment of Gartland Type 2 supracondylar humerus fractures in children?J Pediatr Orthop 2008 28(2):139-41. [Google Scholar]
[23]. Archibeck MJ, Scott SM, Peters CL, Brachialis muscle entrapment in displaced supracondylar humerus fractures: a technique of closed reduction and report of initial resultsJ Pediatr Orthop 1997 17(3):298-302. [Google Scholar]
[24]. http://www.aaos.org/research/Appropriate_Use/PSHF_Vascular_Injury_AUC.pdf [Google Scholar]
[25]. http://www.orthoguidelines.org/go/auc/auc.cfm?auc_id=224922 [Google Scholar]
[26]. http://www.orthoguidelines.org/go/auc/auc.cfm?auc_id=224951 [Google Scholar]
[27]. Pirone AM, Graham HK, Krajbich JI, Management of displaced extension-type supracondylar fractures of the humerus in childrenJ Bone Joint Surg Am 1988 70(5):641-50. [Google Scholar]
[28]. Iyengar SR, Hoffinger SA, Townsend DR, Early versus delayed reduction and pinning of type III displaced supracondylar fractures of the humerus in children: a comparative studyJ Orthop Trauma 1999 13(1):51-55. [Google Scholar]
[29]. Leet AI, Frisancho J, Ebramzadeh E, Delayed treatment of type 3 supracondylar humerus fractures in childrenJ Paediatr Orthop 2002 22(2):203-07. [Google Scholar]
[30]. Mehlman CT, Strub WM, Roy DR, Wall EJ, Crawford AH, The effect of surgical timing on the perioperative complications of treatment of supracondylar humeral fractures in childrenJ Bone Joint Surg Am 2001 83-A(3):323-27. [Google Scholar]
[31]. Carmichael KD, Joyner K, Quality of reduction versus timing of surgical intervention for pediatric supracondylar humerus fracturesOrthopaedics 2006 29(7):628-32. [Google Scholar]
[32]. Sadiq MZ, Syed T, Travlos J, Management of grade III supracondylar fractures of humerus by straight arm lateral tractionInt Orthopaedics 2007 31(2):155-58. [Google Scholar]
[33]. de Gheldere A, Bellan D, Outcome of Gartland type II and type III supracondylar fractures treated by Blount’s techniqueIndian J Orthop 2010 44(1):89-94. [Google Scholar]
[34]. Seyed Ali MN, Seyed Abdolhossein MN, Mohammad B, Effect of supination versus pronation in the non-operative treatment of pediatric supracondylar humerus fracturesArch Trauma Res 2013 2(1):26-29. [Google Scholar]
[35]. Shaw BA, Kasser JR, Emans JB, Rand FF, Management of vascular injuries in displaced supracondylar humerus fractures without arteriographyJournal of orthopaedic trauma 1990 4(1):25-29. [Google Scholar]
[36]. Ozturkmen Y, Karamehmetoglu M, Azboy I, Closed reduction and percutaneous lateral pin fixation in the treatment of displaced supracondylar fractures of the humerusActa Orthop Traumatol Turc 2005 39(5):396-403. [Google Scholar]
[37]. Brauer CA, Lee BM, Bae DS, Waters PM, Kocher MS, A systematic review of medial and lateral entry pinning versus lateral entry pinning for supracondylar fractures of the humerusJ Pediatr Orthop 2007 27(2):181-86. [Google Scholar]
[38]. Yousri T, Tarassoli P, Whitehouse M, Monsell F, Khan WS, Systematic review of randomized controlled trials comparing efficacy of crossed versus lateral K-wire fixation in extension type Gartland Type III supracondylar fractures of the humerus in childrenOrtop Traumatol Rehabil 2012 14(5):397-405. [Google Scholar]
[39]. Ersan O, Gonen E, Arik A, Dasar U, Ates Y, Treatment of supracondylar fractures of the humerus in children through an anterior approach is a safe and effective methodInt Orthop 2009 33(5):1371-75. [Google Scholar]
[40]. Eren A, Güven M, Erol B, Cakar M, Delayed surgical treatment of supracondylar humerus fractures in children using a medial approachJ Child Orthop 2008 2(1):21-27. [Google Scholar]
[41]. Baratz M, Micucci C, Sangimino M, Pediatric supracondylar humerus fracturesHand Clin 2006 22:69 [Google Scholar]
[42]. Keppler P, Salem K, Schwarting B, Kinzl L, The effectiveness of physiotherapy after operative treatment of supracondylar humeral fractures in childrenJ Pediatr Orthop 2005 25:314 [Google Scholar]
[43]. Omid R, Choi PD, Skaggs DL, Supracondylar humeral fractures in childrenJ Bone Joint Surg Am 2008 90:11-21. [Google Scholar]
[44]. Garg S, Weller A, Larson AN, Fletcher ND, Kwon M, Schiller J, Clinical characteristics of severe supracondylar humerus fractures in childrenJournal of Pediatric Orthopaedics 2014 34(1):34-39. [Google Scholar]
[45]. Griffin KJ, Walsh SR, Markar S, Tang TY, Boyle JR, Hayes PD, The pink pulseless hand: a review of the literature regarding management of vascular complications of supracondylar humeral fractures in childrenEuropean Journal of Vascular and Endovascular Surgery 2008 36(6):697-702. [Google Scholar]
[46]. Lins RE, Simovitch RW, Waters PM, Pediatric elbow traumaOrthop Clin North Am 1999 30:119 [Google Scholar]
[47]. Valentini MB, Farsetti P, Martinelli O, Laurito A, Ippolito E, The value of ultrasonic diagnosis in the management of vascular complications of supracondylar fractures of the humerus in childrenBone Joint J 2013 95(5):694-98. [Google Scholar]
[48]. Mangat KS, Martin AG, Bache CE, The ‘pulseless pink’ hand after supracondylar fracture of the humerus in children: the predictive value of nerve palsyJ Bone Joint Surg Br 2009 91:1521-25. [Google Scholar]
[49]. Blakey CM, Biant LC, Birch R, Ischaemia and the pink, pulseless hand complicating supracondylar fractures of the humerus in childhood: long-term follow upJ Bone Joint Surg Br 2009 91:1487 [Google Scholar]
[50]. Korompilias AV, Lykissas MG, Mitsionis GI, Kontogeorgakos VA, Manoudis G, Beris AE, Treatment of pink pulseless hand following supracondylar fractures of the humerus in childrenInt Orthop 2009 33(1):237-41. [Google Scholar]
[51]. Wu J, Perron AD, Miller MD, Powell SM, Brady WJ, Orthopaedic pitfalls in the ED: pediatric supracondylar humerus fracturesThe American Journal of Emergency Medicine 2002 20(6):544-50. [Google Scholar]
[52]. Fletcher ND, Schiller JR, Garg S, Weller A, Larson AN, Kwon M, Increased severity of type III supracondylar humerus fractures in the preteen populationJournal of Pediatric Orthopaedics 2012 32(6):567-72. [Google Scholar]
[53]. Brown IC, Zinar DM, Traumatic and iatrogenic neurological complications after supracondylar humerus fractures in childrenJournal of Pediatric Orthopaedics 1995 15(4):440-43. [Google Scholar]
[54]. Lyons ST, Quinn M, Stanitski CL, Neurovascular injuries in type III humeral supracondylar fractures in childrenClinical Orthopaedics and Related Research 2000 376:62-67. [Google Scholar]
[55]. Barrett KK, Skaggs DL, Sawyer JR, Andras L, Moisan A, Goodbody C, Supracondylar humeral fractures with isolated anterior interosseous nerve injuries: is urgent treatment necessary?J Bone Joint Surg Am 2014 96(21):1793-97. [Google Scholar]
[56]. Price C, Phillips J, Devito D, Management of fracturesIn: Lovell & Winter’s Pediatric Orthopaedics 2001 5thPhiladelphiaLippincott Williams & Wilkins:1319Morrissey, Weinstein SL. (Eds) [Google Scholar]
[57]. Farnsworth CL, Silva PD, Mubarak SJ, Etiology of supracondylar humerus fracturesJ Pediatr Orthop 1998 18:38 [Google Scholar]
[58]. Abe M, Ishizu T, Shirai H, Okamoto M, Onomura T, Tardy ulnar nerve palsy caused by cubitus varus deformityJ Hand Surg Am 1995 20:5-9. [Google Scholar]
[59]. O’Driscoll SW, Spinner RJ, McKee MD, Kibler WB, Hastings H, Morrey BF, Tardy posterolateral rotatory instability of the elbow due to cubitusvarusJ Bone Joint Surg Am 2001 83:1358-69. [Google Scholar]
[60]. Takahara M, Sasaki I, Kimura T, Kato H, Minami A, Ogino T, Second fracture of the distal humerus after varusmalunion of a supracondylar fracture in childrenJ Bone Joint Surg Br. 1998 80:791-97. [Google Scholar]
[61]. Takagi T, Takayama S, Nakamura T, Horiuchi Y, Toyama Y, Ikegami H, Supracondylar osteotomy of the humerus to correct cubitusvarus: Do both internal rotation and extension deformities need to be corrected?J Bone Joint Surg Am 2010 92:1619-26. [Google Scholar]
[62]. Eren A, Guven M, Erol B, Akman B, Ozkan K, Correlation between posteromedial or posterolateral displacement and cubitusvarus deformity in supracondylar humerus fractures in childrenJ Child Orthop 2008 2(2):85-89. [Google Scholar]