Obesity is a condition of excessive fat accumulation and is a major risk factor for a number of chronic diseases. It is a health disorder and is growing in high income countries, as well as in low and middle income countries [1–3]. This health problem is increasing in cities like Mumbai in India and the causes are urbanization and life style changes, among other factors [4–6]. The previous studies showed that among the Asian Indians, the prevalence of obesity is high in male populations [7,8].
BMI (Body Mass Index) is considered as a measure of obesity. It was observed that for Asian Indians, BMI cut-off points are to be considered much lesser than the WHO standards for categorizing the obesity [9–12]. In our study, subjects with BMI of 25kg/m2 or above were considered as obese.
In general, obesity is caused by an unbalance in the energy intake and energy expenditure [13]. The causes of obesity are not fully understood but it is a multi factorial disorder. The present options for controlling obesity are inadequate and have adverse effects [14–17]. Yoga is an ancient therapeutic practice based on Patanjali yoga sutras [18–20]. The Integrated Approach of Yoga Therapy (IAYT) consists of yogic practices based on ancient yoga texts and addresses the mind and body in a holistic way. The earlier studies showed that Yoga practice is useful for stress reduction, awareness on satiety, awareness on over eating and weight reduction [21]. The long term effect of yoga after imparting the training is required to be assessed. The aim of this study was to assess the final outcome after 3 months, of obesity parameters, after giving 14 weeks of IAYT training, for adult male, in an urban setting.
Materials and Methods
Participants
The study was a parallel group study with Yoga and Control groups. After training 14 weeks the Yoga group continued practice of yoga, for the next 3 months. The Control group was not given any specific physical activity.
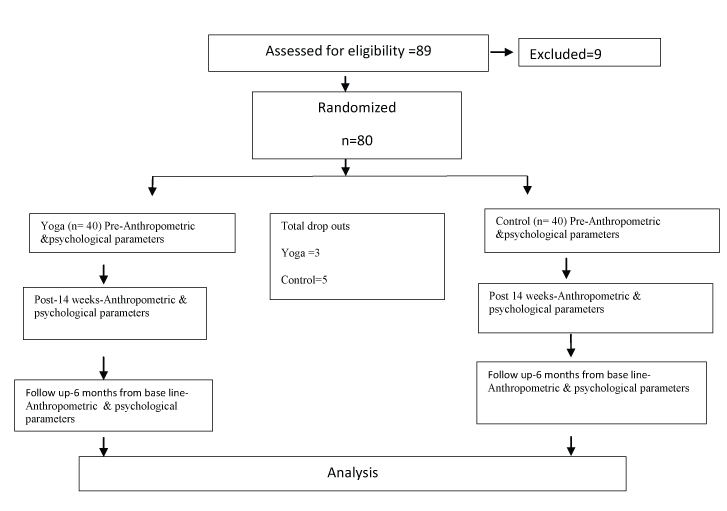
The participants were from north east part of Mumbai. Advertisement was done and total 80 subjects were enrolled based on inclusion criteria. After randomization with minimization of co-factors, 40 subjects were assigned in each group. The IAYT training was given to Yoga group for 14 weeks and assessments outcome were reported in an earlier paper [22]. Further the study was continued and the final results were taken and the outcome is presented in this paper.
The trial profile is shown in [Table/Fig-1]. Open source software, titled MinmPy, was used for randomization with minimization of co factors [23]. In the inclusion criteria, BMI was from 23 to 35 kg/m2, and age was from 18 to 60 years. All the participants were male. The subjects who had any surgery during previous six months were excluded. Each participant was given an alpha numeric code to remove all personal identities.
Sample Size
The minimum sample size was determined based on a previous study [24]. In the previous study, out of the 4 primary outcome variables, HC (Hip Circumference) had the lowest effect size and it was considered for calculating the minimum sample size [24]. An open source software, G*Power 3.1 was used and the minimum sample size was determined as 29 [25].
Intervention
The IAYT yoga training consisted of Lecture, Loosening Exercises, Suryanamaskara, Asana, Pranayama and Meditation. All practices were introduced in a slow and progressive manner. Yoga training was for 90 minutes, for five days in a week. After the 14 weeks training Yoga group continued their practice at their home. Regular e-mail, once in a week, was sent to them as a reminder to do yoga practice and requested them to maintain the food log as done during the yoga training. During the final assessment of anthropometric and psychological parameters, after 3 months, all subjects self reported that they were performing yoga practice. The control group was not given any specific physical exercise but they were asked to continue their regular physical activities. The details of the yoga intervention are shown in [Table/Fig-2]. The intervention was during March to September 2015.
Five part yoga training details.
| Sr. No. | Yoga practice | Duration in Minutes |
|---|
| 1 | Lecture & Counselling | 10 |
| 2a | Loosening Exercises | 10 |
| 2b | Suryanamaskara | 10 |
| 3 | Asana | 30 |
| 4 | Pranayama | 15 |
| 5 | Meditation | 15 |
| Total duration | 90 |
Components Across both the Groups
All participants were given their respective measurement records (Pre and Interim at 14 weeks) and the sample meal plan applicable for sedentary male adults, based on guidelines of National Institute of Nutrition Hyderabad [26].
Assessments
The Wt (Body Weight), BMI, WC (Waist Circumference), HC (Hip Circumference), WHR (Waist hip Ratio), A Body Shape Index (ABSI), Skinfold thickness (SKF) at 4 body points applicable for men and Mid Upper Arm Circumference (MAC) of left and right arms were taken. ABSI was calculated based on WC height and BMI [27–29].
The scores of Perceived Stress Scale (PSS) and Acceptance and Action Questionnaire for Weight Related Difficulty (AAQW) were taken [30–32]. PSS is a validated scale for perceived stress. The AAQW is a validated scale which assesses the experience based avoidance and psychological inflexibility associated with food habits and obesity [32].
For assessing the SKF, skinfold thickness caliper was used [33,34]. The assessments were done at four locations applicable for male [35,36]. The table applicable for men was used for calculating Percentage Body Fat (PFC), based on the cumulative value of skin fold thicknesses [35]. The four measures of SKF were at biceps, triceps, subscapular and suprailiac sites. Each SKF was calculated from the average of three readings. The cumulative SKF was found from sum of the four SKFs. The Wt was measured in electronic weighing scale and circumferences were measured using non elastic tape.
Ethical Clearance
The Institutional Ethical Committee (IEC) clearance was taken.
Informed consent
The informed consent from participants was obtained before recruitment.
Trial Registration
Registered at Clinical Trials Registry of India CTRI/2015/01/005433.
Statistical Analysis
Analysis was performed using SPSS software, version 21.0 The normality test was done by Shapiro wilk test. The Paired sample t-test was done for all the parameters, for the first and final values, of both groups, which were found normally distributed. For not normally distributed parameters, the Wilcoxon signed ranks test was done. The Between group analysis was done by independent sample t-test. To find the relative improvement, from Pre to Final values, among the variables, the differences of Pre to Final values were correlated, among each other. A two sided, value of p<0.05 was considered statistically significant.
Results
The base line demographic data of age, height and BMI of the groups are given in [Table/Fig-3]. The outcome of within group analysis of anthropometric parameters, for the Yoga and Control groups are given in [Table/Fig-4,5] respectively. The between group analysis at 6 months, is given in [Table/Fig-6]. The relative improvements (from Pre to Final) among the variables are given in [Table/Fig-7]. The comparative data of Pre, Interim and Final are given in [Table/Fig-8].
Shapiro wilk test was applied for normality.
| Variable | Yoga Group | Control Group |
|---|
| Pre | 95% C | Pre | 95% C |
|---|
| Age | 40.03±8.74 | (37.12-42.94) | 42.20±12.06 | (38.76-46.89) |
| Height | 169.45±7.35 | (167.00-171.90) | 169.29±6.37 | (167.17-171.65) |
| Min | Max | Min | Max |
| BMI | 25.33 | 34.84 | 25.01 | 33.64 |
BMI- Body Mass Index
Pre: Before intervention
Within group analysis of normally distributed variables.
| Variable | Pre Mean ± Std Dev. | Final Mean ± Std Dev. | t value | Sig | Means 95% C | Lower | Upper |
|---|
| Yoga group |
| WT | 82.63±10.05 | 80.47±9.59 | 2.86 | 0.007 | 2.16 | 0.63 | 3.68 |
| MACL | 29.98±2.02 | 28.21±1.59 | 8.34 | 0.001 | 1.77 | 1.34 | 2.20 |
| MACR | 30.18±2.04 | 28.24±2.07 | 5.14 | 0.001 | 1.94 | 1.17 | 2.71 |
| HC | 103.50±5.71 | 99.46±4.76 | 6.15 | 0.001 | 4.04 | 2.71 | 5.37 |
| RAB | 19.05±7.01 | 15.26.±2.90 | 3.54 | 0.001 | 3.80 | 1.62 | 5.97 |
| STOF | 32.45±7.82 | 26.47±6.69 | 3.52 | 0.001 | 5.98 | 2.53 | 9.42 |
| SHOB | 27.87±6.97 | 23.10±5.61 | 3.27 | 0.002 | 4.77 | 1.81 | 7.73 |
| BMI | 28.7±2.35 | 27.97±2.21 | 2.77 | 0.009 | 0.73 | 0.20 | 1.26 |
| SKFT | 93.93±22.56 | 76.45±11.74 | 4.37 | 0.001 | 17.48 | 9.36 | 25.60 |
| PSS | 16.51±6.12 | 12.16±6.90 | 3.93 | 0.001 | 4.35 | 2.11 | 6.60 |
| AAQW | 81.24±17.35 | 74.76±16.16 | 2.46 | 0.019 | 6.49 | 1.15 | 11.82 |
| Control group |
| WT | 79.45±8.85 | 78.82±9.16 | 1.52 | 0.139 | 0.63 | -0.22 | 1.48 |
| MACL | 32.53±16.53 | 28.30±1.86 | 1.52 | 0.137 | 4.23 | -1.42 | 9.89 |
| MACR | 32.47±16.73 | 28.39±2.04 | 1.46 | 0.154 | 4.09 | -1.60 | 9.77 |
| HC | 104.28±6.60 | 100.50±5.79 | 5.78 | 0.001 | 3.78 | 2.45 | 5.10 |
| RAB | 13.70±6.57 | 14.77±3.66 | -0.94 | 0.354 | -1.07 | -3.37 | 1.24 |
| STOF | 27.46±9.37 | 24.81±6.10 | 1.80 | 0.081 | 2.65 | -0.35 | 5.65 |
| SHOB | 21.76±7.11 | 22.2±6.42 | -0.30 | 0.765 | -0.43 | -3.36 | 2.49 |
| BMI | 27.70±2.05 | 27.28±2.55 | 1.66 | 0.106 | 0.42 | -0.09 | 0.93 |
| SKFT | 73.65±20.61 | 72.12±13.88 | 0.46 | 0.651 | 1.53 | -5.27 | 8.33 |
| PSS | 14.29±6.51 | 13.06±6.31 | 1.42 | 0.165 | 1.23 | -0.53 | 2.99 |
| AAQW | 73.11±14.80 | 66.63±14.20 | 2.83 | 0.008 | 5.49 | 1.55 | 9.42 |
Paired sample t test was done for all the above Table/Fig 4
WT: weight
MACL: Mid upper arm circumference of left hand
MACR: Mid arm circumference of right hand
HC: Hip circumference
RAB: Triceps skin fold thickness
STOF: Suprailiac skin fold thickness
SHOB: Sub scapular skin fold thickness
BMI: Body mass index
SKFT: Cumulative skin fold thickness
PSS: Perceived stress scale score
AAQW: Action and weight relayed difficulty score
Within group analysis of not normally distributed variables.
| Variable | Yoga group | Z score | Sig asymp.sig (2- tailed) |
|---|
| Pre Mean ± Std Dev. | Final Mean ± Std Dev. | t value | Sig |
|---|
| WC | 99.58±7.37 | 97.12-102.04 | 95.09±6.76 | 92.84-97.34 | -4.79b | 0.001 |
| RAF | 14.55±7.19 | 12.16-16.95 | 11.62±3.14 | 10.58-12.67 | -2.29b | 0.020 |
| WHR | 0.96±0.04 | 0.95-0.98 | 0.96±0.04 | 0.94-0.97 | -1.41b | 0.158 |
| PFC | 30.78±4.37 | 29.32-32.24 | 28.16±3.45 | 27.01-29.31 | -3.75b | 0.001 |
| Variable | Control group | Z score | Sig asymp.sig (2- tailed) |
| Pre Mean ± Std Dev. | Final Mean ± Std Dev. | t value | Sig |
| WC | 99.28±6.82 | 96.94-101.63 | 96.29±7.20 | 93.81-98.76 | -3.12b | 0.002 |
| RAF | 10.72±5.00 | 9.01-12.43 | 10.34±3.06 | 9.29-11.39 | -0.57b | 0.572 |
| WHR | 0.95±0.06 | 0.93-0.97 | 0.96±0.05 | 0.94-0.97 | -0.02b | 0.987 |
| PFC | 27.55±5.17 | 25.77-29.33 | 27.64±4.65 | 26.05-29.24 | -0.19c | 0.852 |
Wilcoxon signed ranks test was done for Not Normally distributed variables
b- based on positive ranks
c- based on negative ranks
WC: Waist circumference
RAF: Biceps skin fold thickness
WHR: Waist hip ratio
PFC Percentage fat(based on skin fold thickness)
| Variable | Yoga - Final- Mean Std dev n=37 | Control -Final- Mean Std dev n=35 | t | Sig (2- tailed) | Diff. in Mean 95% CI lower/Upper |
|---|
| WT | 80.47± 9.59 | 78.82± 9.16 | 0.75 | 0.46 | 1.65 (-2.76 - 6.07) |
| MACL | 28.21±1.59 | 28.30±1.86 | -0.22 | 0.83 | -0.09 (-0.90 – 0.72) |
| MACR | 28.24±2.07 | 28.39±2.04 | -0.31 | 0.76 | -0.15 (-1.11 – 0.82) |
| HC | 99.46±4.76 | 100.50±5.79 | -0.83 | 0.41 | -1.04 (-3.53 – 1.45) |
| RAB | 15.26±2.90 | 14.77±3.66 | —0.63 | 0.53 | 0.49 (-1.06 – 2.04) |
| STOF | 26.47±6.69 | 24.81±6.10 | 1.10 | 0.28 | 1.66 (-1.35 – 4.67) |
| SHOB | 23.10±5.61 | 22.20±6.42 | 0.64 | 0.53 | 0.90 (-1.93 – 3.73) |
| BMI | 27.97±2.21 | 27.28±2.55 | 1.22 | 0.23 | 0.68 (-0.43 – 1.80) |
| SKFT | 76.45±11.74 | 72.12±13.88 | 1.43 | 0.16 | 4.33 (-1.70 – 10.36) |
| PSS | 12.16±6.90 | 13.06±6.31 | -0.57 | 0.57 | -0.89 (-4.01 – 2.22) |
| AAQW | 74.76±16.16 | 67.63±14.20 | 1.98 | 0.06 | 7.13 (-0.04 – 14.30) |
An independent sample t test was applied between yoga & control groups
WT: weight
MACL: Mid upper arm circumference of left hand
MACR: Mid upper arm circumference of right hand
HC: Hip circumference
RAB: Triceps skin fold thickness
SHOB: Subscapular skin fold thickness
STOF: Suprailiac skin fold thickness
BMI: body mass index
SKFT Cumulative skin fold thickness
PSS: Perceived stress scale score
AAQW: Action and weight relayed difficulty score
Correlation analysis on improvement from pre to final readings, among variables.
| Difference of final –pre values | WT | MACL | MACR | WC | HC | RAF | RAB | STOF | SHOB | BMI | WHR | SKFT | PFC | PSS | AAQW |
|---|
| WT | 1.00 | | | | | | | | | | | | | | |
| MACL | -0.01 | 1.00 | | | | | | | | | | | | | |
| MACR | 0.01 | 0.991** | 1.00 | | | | | | | | | | | | |
| WC | 0.700** | 0.07 | 0.07 | 1.00 | | | | | | | | | | | |
| HC | 0.594** | 0.00 | 0.03 | 0.656** | 1.00 | | | | | | | | | | |
| RAF | 0.202* | -0.09 | -0.07 | 0.229* | 0.13 | 1.00 | | | | | | | | | |
| RAB | 0.361** | -0.08 | -0.05 | 0.271* | 0.11 | 0.624** | 1.00 | | | | | | | | |
| STOF | 0.458** | 0.01 | 0.00 | 0.503** | 0.234* | 0.350** | 0.326** | 1.00 | | | | | | | |
| SHOB | 0.297** | -0.09 | -0.06 | 0.282** | 0.241* | 0.328** | 0.335** | 0.420** | 1.00 | | | | | | |
| BMI | 0.854** | -0.02 | 0.01 | 0.509** | 0.470** | 0.205* | 0.358** | 0.435** | 0.272* | 1.00 | | | | | |
| WHR | 0.318** | 0.10 | 0.06 | 0.670** | -0.12 | 0.16 | 0.234* | 0.427** | 0.14 | 0.19 | 1.00 | | | | |
| SKFT | 0.462** | -0.08 | -0.05 | 0.455** | 0.257* | 0.716** | 0.723** | 0.761** | 0.742** | 0.443** | 0.339** | 1.00 | | | |
| PFC | 0.449** | -0.06 | -0.04 | 0.457** | 0.249* | 0.659** | 0.693** | 0.728** | 0.745** | 0.445** | 0.354** | 0.963** | 1.00 | | |
| PSS | 0.14 | -0.291** | -0.300** | 0.07 | -0.04 | -0.02 | -0.03 | 0.07 | 0.04 | 0.10 | 0.14 | 0.03 | 0.02 | 1.00 | |
| AAQW | 0.290** | 0.01 | -0.01 | 0.295** | 0.02 | -0.02 | 0.07 | 0.19 | 0.01 | 0.348** | 0.358** | 0.10 | 0.12 | 0.260* | 1.00 |
**. Correlation is significant at the 0.01 level (1-tailed).
*. Correlation is significant at the 0.05 level (1-tailed).
Bivariate -Pearson correlation test applied
WT: weight
MACL: Mid arm circumference left
MACR: Mid arm circumference right
HC: Hip circumference
WC: Waist circumference
RAF:Biceps skin fold thickness
RAB: Triceps skin fold thickness
SHOB: Sub scapular skin fold thickness
STOF: Suprailiac skin fold thickness
BMI: body mass index
WHR: Waist hip ratio
PFC: Percentage fat
SKFT: Cumulative skin fold thickness
PSS: Perceived stress scale score
AAQW: Action and weight relayed difficulty score
Pre- Interim- Final Results
| Sr. No | Group | Parameter | Pre | Interim | Final | Sig Pre Interim | Sig Pre Final |
|---|
| 1 | Yoga | WT | 82.63±10.05 | 81.51±10.00 | 80.47±9.59 | 0.004 | 0.007 |
| Control | 79.45±8.85 | 79.22±8.93 | 78.82±9.16 | 0.353 | 0.139 |
| 2 | Yoga | MACL | 29.98±2.02 | 29.42±1.92 | 28.21±1.59 | 0.016 | <0.001 |
| Control | 32.53±16.53 | 28.10±1.70 | 28.30±1.86 | 0.118 | 0.137 |
| 3 | Yoga | Macr | 30.18±2.04 | 29.64±2.04 | 28.24±2.07 | 0.018 | <0.001 |
| Control | 32.47±16.73 | 28.10±1.85 | 28.39±2.04 | 0.125 | 0.154 |
| 4 | Yoga | HC | 103.50±5.71 | 101.29±4.95 | 99.46±4.76 | <0.001 | <0.001 |
| Control | 104.28±6.60 | 101.38±6.13 | 100.50±5.79 | <0.001 | <0.001 |
| 5 | Yoga | WC | 99.58±7.37 | 98.25±7.12 | 95.09±6.76 | 0.039 (z score -2.06b) | <0.001 (z score -4.79b) |
| Control | 99.28±6.82 | 95.79±8.33 | 96.29±7.20 | <0.001 (z score -3.71b) | 0.002 (z score -3.12b) |
| 6 | Yoga | WHR | 0.96±0.04 | 0.97±0.05 | 0.96±0.04 | 0.069 (z score -1.82c) | 0.158 (z score -1.41b) |
| Control | 0.95±0.06 | 0.94±0.06 | 0.96±0.05 | 0.413 (z score -0.82b) | 0.987 (z score -0.02b) |
| 7 | Yoga | PFC | 30.78±4.37 | 29.66±3.30 | 28.16±3.45 | 0.051 (z score -1.96b) | <0.001 (z score -3.75b) |
| Control | 27.55±5.17 | 27.58±5.29 | 27.64±4.65 | 0.98 (z score -0.03c) | 0.852 (z score -0.19c) |
| 8 | Yoga | BMI | 28.7±2.35 | 28.33±2.42 | 27.97±2.21 | 0.008 | 0.009 |
| Control | 27.70±2.05 | 27.61±2.01 | 27.28±2.55 | 0.306 | 0.106 |
| 9 | Yoga | SKFT | 93.93±22.56 | 85.52±13.38 | 76.45±11.74 | 0.032 | <0.001 |
| Control | 73.65±20.61 | 72.17±14.55 | 72.12±13.88 | 0.693 | 0.651 |
| 10 | Yoga | Biceps-skfraf | 14.55±7.19 | 12.70±5.02 | 11.62±3.14 | 0.156 (z score -1.42b) | 0.02 (z score -2.29b) |
| Control | 10.72±5.00 | 11.10±3.69 | 10.34±3.06 | 0.502 (z score -0.672c) | 0.572 (z score -0.57b) |
| 11 | Yoga | Triceps-skfrab | 19.05±7.01 | 17.87±5.05 | 15.26.±2.90 | 0.379 | 0.001 |
| Control | 13.70±6.57 | 13.22±4.24 | 14.77±3.66 | 0.652 | 0.354 |
| 12 | Yoga | suprailiac-skfstof | 32.45±7.82 | 28.04±5.45 | 26.47±6.69 | 0.002 | 0.001 |
| Control | 27.46±9.37 | 25.57±7.06 | 24.81±6.10 | 0.259 | 0.081 |
| 13 | Yoga | Subscapular-skfshob | 27.87±6.97 | 26.91±5.23 | 23.10±5.61 | 0.396 | 0.002 |
| Control | 21.76±7.11 | 22.28±4.98 | 22.20±6.42 | 0.707 | 0.765 |
| 14 | Yoga | PSS | 16.51±6.12 | 12.59±6.65 | 12.16±6.90 | <0.001 | <0.001 |
| Control | 14.29±6.51 | 13.51±5.95 | 13.06±6.31 | 0.493 | 0.165 |
| 15 | Yoga | AAQW | 81.24±17.35 | 71.54±14.62 | 74.76±16.16 | <0.001 | 0.019 |
| Control | 73.11±14.80 | 69.71±16.28 | 66.63±14.20 | 0.224 | 0.008 |
Paired sample t test was applied for all Normally distributed variables and Wilcoxon signed ranks test was applied for Not Normally distributed variables
b- based on positive ranks, c- based on negative ranks
WT: weight
MACL: Mid arm circumference left
MACR: Mid arm circumference right
HC: Hip circumference
WC: Waist circumference
WHR: Waist hip ratio
PFC: Percentage body fat
BMI: body mass index
SKFT: Cumulative skin fold thickness
SKFRAF: Biceps skin fold thickness
SKFRAB: Triceps skin fold thickness
SKFSHOB: Sub scapular skin fold thickness
SKFSTOF: Suprailiac skin fold thickness
PSS: Perceived stress scale score
AAQW: Action and weight relayed difficulty score
In each group, 50% of the total subjects was having educational qualification between 10th standard to graduates and 50% was post graduates or above. Also in each group 50% was in age group of 18 to 40 and 50% was in age group of 41 to 60 years. In each of the groups, all the subjects were working and all were having BMI above 25 Kg/m2. The minimum age in Yoga group was 26 and maximum was 60 whereas in Control group, minimum was 21 and maximum 58. Thus minimization of co factors was done [23,37,38]. None of the subjects reported any adverse events due to the intervention.
The combined Pre, Interim and Final results given in [Table/Fig-8], shows that some of the gain in the interim values was lost during the final results.
Anthropometric Parameters
All parameters except WC, WHR, PFC and SKF of biceps were normally distributed.
There was consistent improvement from Pre to Interim to Final result, in the parameters of Wt, HC, BMI, Cumulative skin fold thickness (SKFT), SKF of biceps (SKFraf) and SKF of suprailiac (SKFstof) for both the groups. The Skfstof was improved from Pre to Interim (p<0.002) & Interim to Final (p<0.001) in the Yoga group. In the Yoga group the improvement in SKFT, in Pre to Final was more significant (p<0.001) than in Pre to Interim (p<0.05). In Yoga group alone, MACL and MACR were improved consistently from Pre Interim to Final (p<0.001 for both MACL and MACR for pre-final). Control group did not improve in these parameters in the final result. The WC (p<0.001), WHR, and PFC (p<0.001) were improved from Pre to Interim and to Final in Yoga group but in Control group the gain was lost in the final result. The PFC of Control group was increased in the Final (increase was not significant).
The SKF of triceps (SKFrab), in Control group reduced in Interim but increased in Final. In the Control group, the SKF of sub scapular (SKFshob) increased in Interim and remained almost same in the Final.
The Final results, with respect to the Pre values were as below:
The Wt in the Yoga and Control groups were decreased during the 6 months. The Wt reduction in Yoga group alone was significant (p<0.007). The upper mid arm circumference of right arm (MACR) and upper mid arm circumference of left arm (MACL) were reduced in both the groups but change in Yoga group alone was significant (p<0.001). The WC was reduced in both the groups (yoga p< 0.001 and control p<0.002). WHR remained same in yoga, increased in control but not significant. In Yoga, the PFC, based on chart, was decreased and was significant (p<0.001) [35]. In the Control group it was increased but was not significant. HC was reduced and was significant in both the groups (p<0.001). The cumulative skin fold thickness was reduced in both the groups but was significant (p<0.001) in Yoga group alone. The SKFrab (p<0.001) SKFshob (p<0.002) and SKFstof (p<0.001) and SKFraf (p <0.02) were reduced in Yoga group. In control group SKFstof and SKFraf reduced but were not significant. SKFrab and SKFshob were increased but changes were not significant. The BMI was reduced in both the groups with significance (p< 0.009) in Yoga group alone. The cumulative Skin Fold Thickness (SKFT) reduction was significant (p<0.001) in the Yoga group alone.
Psychological Parameters
The PSS was improved consistently from Pre Interim to Final in the Yoga group alone (p< 0.001). The AAQW was improved in Control group in the Pre-Interim (but not significant) and improved during Pre to Final (p<0.05).
In Yoga group, AAQW was improved during the Pre-Interim but was increased (worsened) in Final (p<0.001 for Pre-Interim, p< 0.05 for Pre-Final).
Compared to Pre values, the improvement in PSS was significant in the Yoga group (p<0.001) alone. In both the groups (compared to Pre values) the AAQW improvement was significant (Yoga p<0.02 and Control p<0.01).
Correlations
The correlations results with respect to, Pre to Final were as below:
BMI was positively correlated to WC (r=0.509, p<0.01), SKFT (r=0.443, p<0.01), HC (r=0.47, p<0.01) and AAQW (r=0.348, p<0.01). The PSS was not much correlated to BMI. The PSS was negatively correlated to MACL (r=-0.291, p<0.01) and MACR (r=-0.300, p<0.01).
Discussion
There was improvement in anthropometric parameters and this was supportive of the earlier studies [39]. In the Yoga group, PFC decrease (improvement) was significant (p<0.001) considering the Pre Final values, though decrease of PFC was not significant during Pre to Interim. This shows that the 14 weeks IAYT training had effect in the Final values. The weight reduction was more significant in Pre to Final than in Pre to Interim, and the weight reduction was consistent. This indicates that the reduction of weight was due to fat reduction. The earlier study of 8 week yoga on boys, showed a significant decrease in percentage body fat [39].
Earlier short term study on 2 weeks yoga and walking with diet control (residential study), showed significant improvements in anthropometric parameters, with no change in WHR [40]. Another study showed similar results on WHR [41]. In our non residential study, and without diet control (though sample food plan information were given to both the groups), the WHR was increased in Interim (compared to pre) and decreased in Final (with respect to interim value-but compared to Pre value the Final value remained same) in the Yoga group. The WHR was decreased in Interim and increased in Final, in the Control group. But WC and HC were consistently reduced in Yoga group, in Pre to Interim and Pre to Final. WC was increased from Interim to Final in the Control group. This shows that in the Yoga group, the fat stored centrally and at peripherally was reduced in a similar way. Similar trend was noted in a short duration trial on obese adults [40]. In the Control group the WHR improvement (decrease) may be due to less fat reduction in peripheral area than in abdominal area in the Interim value. The decrease of WHR of Yoga group, in the Final may be due to more decrease of WC than HC. This could be due to yoga practices of the abdomen area.
The MAC was measured as part of anthropometric measurement in the earlier studies also [41]. But we assessed both the right and left MAC. In our study MAC reduction was significant for Yoga group alone (p<0.001) both during Pre Interim and Pre Final, which shows some reduction of fat or skin muscle in the upper limb similar to the earlier short duration studies [40].
The SKFT was significant in the Yoga alone (p<0.05 in Pre Interim and p<0.001 in Pre Final). This supports that there is reduction in MAC skin fold muscle or fat in the upper arms due to yoga practice which included the Suryanamaskara and Asana requiring active movement of upper arms, for one third of the yoga duration. The consistent reduction of fat/muscle in upper arms in Final value also shows the effectiveness of IAYT for obesity control.
This also shows that in long term yoga practice can give more balanced reduction at different parts of the body like upper arm and waist, compared to the Control group. In the Control group, reduction in waist area was lesser and also there was lesser reduction in upper arms. This may be due to their varied regular physical activities. In our study, Yoga group SKFT and PFC reduced consistently from Pre Interim to Final unlike in the Control group and the anthropometry and skin fold thickness give the best predictors for obesity assessment [42].
In Yoga group SKFraf, SKFrab, SKFshob and SKFstof were also consistently reduced from Pre Interim to Final value. In the Control group SKFraf, SKFshob and SKFstof reduced but SKFrab got increased from Interim to the Final. This may be due to lesser physical activities using hand and shoulder. The reduction in weight in the Yoga group was in all parts. The Control group, doing their regular physical activities like walking etc. did not get weight reduction in all parts.
In AAQW and PSS scores, there was difference in Pre values in the groups [30,32]. Earlier studies showed Psycho Immunological effects of yoga and reduction of various stress levels [43–45].
Previous study showed that the decrease in weight related experiential avoidance is linked to more weight loss in a male female combined batch [46]. But in the Yoga group the AAQW score increased from Interim to final and in the Control group it was decreased in the Final. The significance of reduction in AAWQ was lost in Yoga group. This may be due to lesser yoga practices of meditation such as MSRT (Mind sound resonance technique) which are having a group effect and was part of the yoga training of 14 weeks. During Interim to Final, the subjects were doing yoga alone at their home in unsupervised situations. In control group AAQW score reduction was almost same as Pre to Interim and Interim to Final. There was no group activity for the Control group and each was continuing their own regular physical activities similar to pre interim period.
The PSS was validated using college students or workers [30]. Our all subjects were working. The PSS is used for measuring the perceived stress [47]. In our study PSS reduced with significance (p<0.001) consistently in Pre Interim and Pre Final in yoga group alone. The yoga practice reduced anxiety and depression scores in mixed male female obese group of grade 2 obesity, BMI 31.37 ± 6.64 with psychological problems [48]. Improvement in depression and anxiety was mostly correlated with improvements in WC and HC [48]. Our study showed that yoga practice during Interim and Final also reduced the perceived stress in obese male of BMI 28.7±2.3. In IAYT module there are many components such as Suryanamaskara Pranayama Body awareness etc which reduces the stress levels [24]. This shows that in the Final, the stress level was reduced and that also might have improved their food habits and promoted weight reduction.
The Pre Final correlation results show that BMI was positively correlated to WC, SKFT, HC and AAQW. These correlations were supportive to earlier short terms studies [48]. The PSS was negatively correlated to MACL (r=-0.291, p<0.01) and MACR (r=-0.300, p<0.01). Higher MAC indicate chronic energy deficiency [49]. Thus, anthropometric and psychological parameters are found to be correlated in obese and the long term yoga practice improves these parameters.
Previous studies showed that short and long term yoga interventions reduce anxiety and mood changes [44,50]. The psychological stress increases cortisol secretion and abdominal fat in an RCT on female [51]. The mindfulness practices modify eating disorders. Our study support that the reduction of abdominal fat in male is consistent with reduction in perceived stress reduction.
Strengths Limitations and Future Scope
Our study is one of the earliest RCTs on male obesity and long term yoga (six months) in urban setting along with assessments of PSS and AAQW. It was reported that people with some belief in yoga join to such programme [21]. Though, all our subjects were new to yoga this point is relevant. Future studies can be taken in different cross sections and in different cities where the eating habits and consumption of junk food could be different. The accurate food log plays a vital role in control of the eating and the smart phone or web based methods will be easier than hand written food log [52,53]. The age group in our study was large to get more sample size and for longer period study. However, the age distribution was similar in both groups by minimization of co factors. Also, the urban human habits of junk food eating, sedentary life etc., are common for all age groups. Further studies can be done with smaller range of age groups and at various cities (probably having varying food habits).
Conclusion
The anthropometric parameters and percentage body fat showed improvement in the Final result. Some of the improvements including AAQW score obtained during the 14 weeks training was lost in the Final value. The PSS score was improved consistently. The fat reduction was effective at central and peripheral parts in the Interim to Final result. Reduction of abdominal fat on male is correlated to reduction in perceived stress. The yoga practice is effective for obesity control for adult male in urban setting.
BMI- Body Mass Index
Pre: Before intervention
Paired sample t test was done for all the above Table/Fig 4
WT: weight
MACL: Mid upper arm circumference of left hand
MACR: Mid arm circumference of right hand
HC: Hip circumference
RAB: Triceps skin fold thickness
STOF: Suprailiac skin fold thickness
SHOB: Sub scapular skin fold thickness
BMI: Body mass index
SKFT: Cumulative skin fold thickness
PSS: Perceived stress scale score
AAQW: Action and weight relayed difficulty score
Wilcoxon signed ranks test was done for Not Normally distributed variables
b- based on positive ranks
c- based on negative ranks
WC: Waist circumference
RAF: Biceps skin fold thickness
WHR: Waist hip ratio
PFC Percentage fat(based on skin fold thickness)
An independent sample t test was applied between yoga & control groups
WT: weight
MACL: Mid upper arm circumference of left hand
MACR: Mid upper arm circumference of right hand
HC: Hip circumference
RAB: Triceps skin fold thickness
SHOB: Subscapular skin fold thickness
STOF: Suprailiac skin fold thickness
BMI: body mass index
SKFT Cumulative skin fold thickness
PSS: Perceived stress scale score
AAQW: Action and weight relayed difficulty score
**. Correlation is significant at the 0.01 level (1-tailed).
*. Correlation is significant at the 0.05 level (1-tailed).
Bivariate -Pearson correlation test applied
WT: weight
MACL: Mid arm circumference left
MACR: Mid arm circumference right
HC: Hip circumference
WC: Waist circumference
RAF:Biceps skin fold thickness
RAB: Triceps skin fold thickness
SHOB: Sub scapular skin fold thickness
STOF: Suprailiac skin fold thickness
BMI: body mass index
WHR: Waist hip ratio
PFC: Percentage fat
SKFT: Cumulative skin fold thickness
PSS: Perceived stress scale score
AAQW: Action and weight relayed difficulty score
Paired sample t test was applied for all Normally distributed variables and Wilcoxon signed ranks test was applied for Not Normally distributed variables
b- based on positive ranks, c- based on negative ranks
WT: weight
MACL: Mid arm circumference left
MACR: Mid arm circumference right
HC: Hip circumference
WC: Waist circumference
WHR: Waist hip ratio
PFC: Percentage body fat
BMI: body mass index
SKFT: Cumulative skin fold thickness
SKFRAF: Biceps skin fold thickness
SKFRAB: Triceps skin fold thickness
SKFSHOB: Sub scapular skin fold thickness
SKFSTOF: Suprailiac skin fold thickness
PSS: Perceived stress scale score
AAQW: Action and weight relayed difficulty score