Alobar Holoprosencephaly Associated with Meningomyelocoele and Omphalocoele: An Unusual Coexistence
Tejaswini Priyadarshan Waghmare1, Pragati Aditya Sathe2, Naina Atul Goel3, Bhuvaneshwari Mahendra Kandalkar4
1 Assistant Professor, Department of Pathology, Seth G.S. Medical College and KEM Hospital, Mumbai, Maharashtra, India.
2 Associate Professor, Department of Pathology, Seth G.S. Medical College and KEM Hospital, Mumbai, Maharashtra, India.
3 Associate Professor, Department of Pathology, Seth G.S. Medical College and KEM Hospital, Mumbai, Maharashtra, India.
4 Professor and Head of Department, Department of Pathology, Seth G.S. Medical College and KEM Hospital, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Tejaswini Priyadarshan Waghmare, Department of Pathology, Seth G.S. Medical College and KEM Hospital, Parel, Mumbai-400012, Maharashtra, India.
E-mail: tejaswinipanad@gmail.com
Holoprosencephaly is a rare congenital disorder which results from failure of cleavage or incomplete differentiation of the forebrain structures at various levels or to various degrees. Depending on the degree of involvement, it is classified into 4 types: Alobar, Semilobar, Lobar and Middle interhemispheric fusion variant. A male child was born to 28-year-old female at 34 weeks of gestation. The mother on antenatal follow-up was detected to have a fetus with multiple congenital anomalies on Ultrasonography (USG) done at 34weeks of gestation. The baby died after 12 hours of birth. A complete autopsy was performed. On external examination, multiple congenital anomalies were seen including cleft lip and palate, absent nasal bridge, proptosis of right eye, micropenis, left undescended testis, bilateral rocker bottom feet, omphalocele and sacral meningomyelocele. Internal examination of the brain revealed hydrocephalus and features of alobar holoprosencephaly. This case is presented for its rarity. In addition, it is unusual for a fetus with alobar holoprosencephaly to survive till term as this is the most severe type. Though facial malformations are usually present in a case of holoprosencephaly, its association with sacral meningomyelocele and omphalocele has rarely been described in literature.
Congenital anomalies, Cranio Facial malformations, Holoprosencephaly
Case Report
A 12 hours and 30 minutes-old-male infant, weighing 1.735 kilograms, was born vaginally to a 28-year-old third gravid mother at 34 weeks of gestation with no significant maternal and family history. The obstretic history of the mother included first female child which was delivered normally at term, presently nine-year-old, second gestation was medically terminated as the baby was malformed and third was the present pregnancy. The mother was not a registered patient and ultrasound done just a day before delivery revealed a large ventricular cavity surrounded by a thin rim of brain in the skull along with a lumbosacral meningomyelocoele and an omphalocoele with liver as content. Clinical examination revealed multiple facial anomalies. There was no spontaneous respiration. In spite of ventilatory support, he was unable to maintain saturation and succumbed in spite of resuscitative measures.
In view of multiple external anomalies, a complete autopsy was requested. The baby was 42 centimeters in length and weighed two kilograms. On external examination, the baby had multiple facial anomalies like cleft lip [Table/Fig-1a], cleft palate, absent nasal bridge [Table/Fig-1a], proptosis of the right eye and hydrocephalus [Table/Fig-1b] with the fontanelles open. In addition, the baby had micropenis and eversion of both feet. There was a lumbosacral meningomyelocoele [Table/Fig-1c] and an omphalocoele on the anterior abdominal wall measuring 14cm in diameter [Table/Fig-1d] as seen on ultrasound.
Clinical images showing multiple anomalies: (a): Facial anomalies: Cleft lip and absence of nasal bridge; (b): Hydrocephalus; (c): Sacral meningomyelocoele; (d): Omphalocoele: 14 centimeters in diameter; (e): Fused cerebral hemispheres; (f): Ventricular cyst measuring 15X14 centimeters.
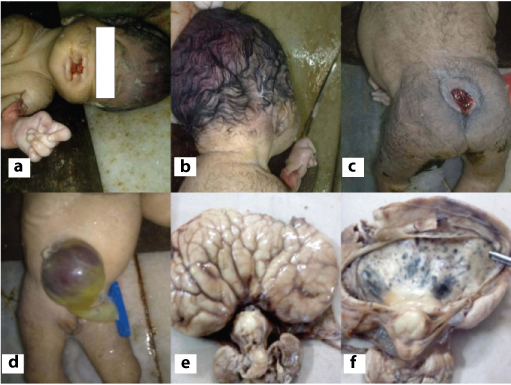
On opening of the skull cavity, there were fused cerebral hemispheres with a single large ventricular cyst measuring 15x14cm [Table/Fig-1e and f]. On opening the omphalocoele sac it showed liver tissue as content. Rest of the organs did not show any abnormality.
On microscopic examination, the brain showed mild cerebral oedema. The liver tissue was confirmed microscopically. All other organs showed signs of prematurity. Cause of death given was alobar holoprosencephaly with multiple congenital anomalies.
Discussion
Holoprosencephaly (HPE) is a rare congenital anomaly with an incidence of 1:16000 live births and 1:250 in utero [1]. The term holoprosencephaly was coined by Demyer and Zeman way back in 1963 [2]. It is a disorder of incomplete or absent division of the prosencephalon occurring during the 4th and 8th week of gestation. This rare anomaly is classified into four types based on [3] the degree of involvement of forebrain-alobar (absence of the interhemispheric fissure, falxcerebri, the third ventricle, and fused thalami, and often absence of neurohypophysis and olfactory tracts), semilobar (posterior partial formation of the interhemispheric fissure, with only a single ventricle), lobar (presence of an interhemispheric fissure but the cingulate gyrus and the lateral ventricles are fused, and there is no septum pellucidum), and a middle interhemispheric fusion variant (deficient interhemispheric fissure with failure of separation of posterior frontal and parietal lobes).
Alobar holoprosencephaly, the most severe subtype, is the com-plete absence of division of the prosencephalon structures resul-ting in completely absent interhemispheric fissure and corpus callosum, fused cerebral hemispheres with only one ventricle which is the prominent feature in our case. Along with the lack of division of embryo’s forebrain there is a defect in the development of the face as also seen in our case. Hence, as rightly mentioned by DeMyer et al., the face predicts the development of the brain 80% of the times [2].
Chang reported two cases of alobar holoprosencephaly of which one had polydactyly and the other has polysplenia whereas, in our case it was omphalocoele and meningomyelocoele [4]. Lami F et al., have discussed four cases of holoprosencephaly of which one had omphacoele, similar to our case, detected on ultrasonography but the pregnancy was terminated at 16 weeks of gestation [5]. Most of the cases of alobar holoprosencephaly do not reach term however one case described by Chang LH survived for 3 days of life [4].
The aetiological factors for holoprosencephaly include environmental and genetic factors including chromosomal anomalies [6]. Environmental factors suggested are maternal diabetes, maternal alcoholism, intrauterine Toxoplasmosis, Rubella, Cytomegalovirus, Herpes simplex, and Syphilis (TORCH) infections, none of which could be elicited in our case. The most common chromosomal anomalies associated with holoprosencephaly are trisomy 13 and trisomy 18, seen in 40% cases [3]. We could not demonstrate any such correlation in our case as genetic studies were not done. Omphalocoele and meningomyelocoele could be a part of the spectrum of midline defects, however information regarding this association is not found in literature.
The prognosis of holoprosencephaly is very poor and it depends on the type, grade of HPE and also on the extent of facial dysmorphic features. Only 50% of patients with alobar HPE survive by 4-5 months of age and 20% of these cases survive by 12 months of age [7,8].
Conclusion
Alobar holoprosencephaly is a disorder with fatal outcome. Timely antenatal diagnosis by ultrasound can allow medical termination of pregnancy and avoid the mental trauma to the parents. Its association with meningomyelocoele and omphalocoele has rarely been described in literature. Hence, this case is presented for its rare occurrence and association with unusual findings. This will enrich the information available on this rare entity.
[1]. Aruna E, Chakravarthy VK, Rao DN, Rao DR, Holoprosencephaly with Multiple Anomalies of the Craniofacial Bones - An Autopsy ReportJ Clin and Diagn Res 2013 7(8):1722-24. [Google Scholar]
[2]. DeMyer W, Zeman W, Palmer CG, The face predicts the brain: Diagnostic significance of median facial anomalies for holoprosencephaly (arhinencephaly)Pediatrics 1964 3:256-63. [Google Scholar]
[3]. Poenaru MO, Vilcea LD, Marin A, Holoprosencephaly: Two Case ReportsMedica Jr of Clinical Medicine 2012 7:58-62. [Google Scholar]
[4]. Chang LH, Alobar Holoprosencephaly: Report of Two Cases with Unusual FindingsMed J 2003 26:700-06. [Google Scholar]
[5]. Lami F, Carli D, Ferrari P, Marini M, Alesi V, Iughetti L, Percesepe A, Holoprosencephaly: report of four cases and genotype–phenotype correlationsJ. Genet 2013 92:97-101. [Google Scholar]
[6]. Kauvar EF, Solomon BD, Curry CJR, van Essen AJ, Janssen N, Dutra A, Holoprosencephaly and agnathia spectrum: Presentation of two new patients andreview of the literatureAm J Med Genet Part C (Semin Med Genet) 2010 154C:158-69. [Google Scholar]
[7]. Gupta AO, Leblanc P, Janumpally KC, Tanya P, A preterm infant with semilobar holoprosencephaly and hydrocephalus: A case reportCases Journal 2010 3:35 [Google Scholar]
[8]. Barr M, Cohen MM, Holoprosencephaly survival and performanceAm J Med Genet 1999 89:116-20. [Google Scholar]