Several authors have studied the relationship between anatomic variants of the middle meatus and the incidence of Chronic Rhinosinusitis (CRS) [1]. Conclusions reported by a great part of literature are discordant. Indeed in contrast with many authors [2–6] who assert that CRS is favored by the presence of anatomic variants, other authors believe that CRS is not related to any anatomic variant [1]. In order to establish the presence of a relationship between CRS and anatomic variants, it is mandatory to establish when sinonasal mucosal is pathological. According to Som [7] sinonasal mucosa should not be visible and any thickening should be considered anomalous. However, the progressive evolution of radiological instrumentations has led to an ever greater image definition. Some authors [8–10] have therefore, defined more precisely a threshold of mucosal thickening above which it is correct to diagnose sinonasal pathology. Maillet et al., defined that a mucosal thickening ≥ 2mm is indicative of sinus inflammation [11]. In the indexed study we first established the level of mucosal thickening associated with maxillary sinus inflammation and then verified its effective relationship with common anatomical variants (concha bullosa, maxillary accessory ostium and Haller cell). Finally, we tested the relationship between thickening of the sinus mucosa and obstruction of the maxillary ostium.
Materials and Methods
A retrospective study was conducted on 70 patients. All patients came to our Rhinological Center from March 2014 to February 2016 and underwent a Cone Beam Computed Tomography (CBCT) of the maxillary sinus by Galileos GAX9 (Sirona Dental System GmbH Bensheim, Germany). The images were analysed by Sidexis XG software (Sirona X-ray Imaging System Next Generation, Sirona Dental System GmbH, Bensheim, Germany) [Table/Fig-1,2].
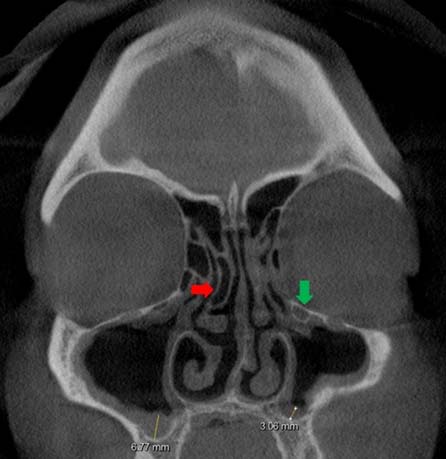
Measurement of mucosal thickening of maxillary sinus [facial CBCT, coronal section].

Mucosal thickening, Concha bullosa (red arrow) and Haller’s cell (green arrow) [facial CBCT coronal section].
All patients performed a 15 days long preparatory treatment before CBCT, using nasal washes with saline and no one was been previously treated with vasoconstrictors. Moreover, before the CBCT, a nasal endoscopy and a cytological analysis of the mucosa were performed for all the patients. These assessments allowed us to exclude patients with acute rhinosinusitis. We also excluded the patients who were previously treated with endoscopic nasal surgery, had allergic rhinitis, maxillary cysts, sinonasal polyposis, odontogenic sinusitis, fungal sinusitis, sinonasal mucocele, neoplastic diseases, severe systemic metabolic disorders and cystic fibrosis. Thus, using axial and coronal scans, both osteo-meatal complex together with maxillary sinuses were analysed for a total of 140 meatus-maxillary units.
We divided the population into two groups: the study group, which included 34 patients (68 meatus–maxillary units) formed by patients presenting symptoms of CRS in accordance with the European Position Paper on Rhinosinusitis and Nasal Polyps 2012 criteria (EPOS), and the control group which included 36 patients (72 meatus-maxillary units) formed by patients who did not present symptoms of CRS. All patients gave their informed consent for the examination. We evaluated in each patient the degree of thickening of the mucosa of the maxillary sinus distinguishing between < or ≥ 2mm. We evaluated the relationship between thickening of the maxillary mucosa and the presence of some common anatomical variants (concha bullosa, accessory maxillary ostium and Haller cell) and the relationship between symptoms of CRS and the presence of those anatomic variants. Finally, we evaluated the association between the closure of maxillary ostium and maxillary mucosal thickening as well as the relationship between a close ostium and CRS.
Statistical analyses were done using dedicated software programs: MINITAB Inc. 17 and R Development Core Team (2015). A p-value less than 0.01 were considered statistically significant in Chi-square tests and in binary logistic regressions.
Results
Of the 70, 36 were females and 34 males, aged between 14 and 80 years with a mean age of 46 years [Table/Fig-3].
| Age (years) | n | % |
|---|
| 14 -35 | 18 | 25.71 |
| 35 -45 | 15 | 21.43 |
| 45 -60 | 19 | 27.15 |
| 60 -80 | 18 | 25.71 |
| Mean-age (years) | 45.69 | |
| Standard deviation-age (years) | 15.45 | |
Chi-square test was used to compare: the mucosal thickening between study and control group [Table/Fig-4]; the presence of anatomic variations (e.g., concha bullosa, Haller’s cell, accessory ostium and natural sinus ostium) between study and control group [Table/Fig-5] and between mucosal thickening < 2mm and ≥ 2mm [Table/Fig-6];
Chi-square test to compare mucosal thickening between study and control group.
| Group | Mucosal Thickening | p-value |
|---|
| < 2mm | ≥ 2mm |
|---|
| Study | 4 | 64 | < 0.01 |
| Control | 51 | 21 |
Chi-square tests to compare anatomic variants and the natural sinus ostium between study group and control group.
| Group | Concha bullosa | p-value |
|---|
| Present | Absent |
|---|
| Study | 28 | 40 | >0.01 |
| Control | 32 | 40 |
| Accessory Ostium | |
| Study | 14 | 54 | > 0.01 |
| Haller’s cell | |
| Study | 31 | 37 | > 0.01 |
| Control | 24 | 48 |
| Natural sinus ostium | |
| Study | 31 | 37 | <0.01 |
| Control | 69 | 3 |
Chi-square tests to compare anatomical variations between mucosal thickening <2 and ≥2mm.
| Mucosal Thickening (mm) | Concha bullosa | p-value |
|---|
| Present | Absent |
|---|
| < 2 | 26 | 29 | > 0.01 |
| ≥ 2 | 34 | 51 |
| Accessory Ostium | |
| < 2 | 18 | 37 | > 0.01 |
| ≥ 2 | 20 | 65 |
| Haller’s cell | |
| < 2 | 24 | 31 | > 0.01 |
| ≥ 2 | 31 | 54 |
| Natural Sinus Ostium | |
| < 2 | 54 | 1 | < 0.01 |
| ≥ 2 | 46 | 39 |
A binary logistic regression was used to prove the relationship between closed natural sinus ostium and the presence of a mucosal thickening ≥ 2mm [Table/Fig-7] and the membership of patients to the study group [Table/Fig-8].
Binary logistic regression between mucosal thickening and the presence of common anatomic variants and natural sinus ostium.
| Mucosal Thickening | Coefficient | p-value |
|---|
| Concha bullosa |
| Present | 0.044 | > 0.01 |
| Absent | 0.0 |
| Haller’s Cell |
| Present | -0.641 | > 0.01 |
| Absent | 0.0 |
| Accessory Ostium |
| Present | 0.210 | > 0.01 |
| Absent | 0.0 |
| Natural sinus ostium |
| Open | 0.0 | < 0.01 |
| Close | 3.99 |
Final model
0: Mucosal Thickening< 2
1: Mucosal Thickening ≥ 2
Mucosal Thickening = - 0.16 + 3.82 . Natural Sinus Ostium (Close)
Binary logistic regression between the membership to a specific group and the presence of common anatomic variants and natural sinus ostium.
| Group | Coefficient | p-value |
|---|
| Concha bullosa |
| Present | -0.336 | > 0.01 |
| Absent | 0.0 |
| Haller’s Cell |
| Present | -0.522 | > 0.01 |
| Absent | 0.0 |
| Accessory Ostium |
| Present | | > 0.01 |
| Absent | 0.0 |
| Natural sinus ostium |
| Open | 0.0 | <0.01 |
| Close | -3.355 |
Final model
0: Studygroup
1: Control group
Group = 0.8 - 3.312 . Natural Sinus Ostium (Close)
In our study, we considered 140 sides (e.g., 68 from the study group and 72 from the control group). There was a statistically significant relationship between mucosal thickening ≥ 2mm and membership of patients to the study group [Table/Fig-4].
Then, we analysed anatomic variations in order to determine their effects on the severity of mucosal thickening and if the patients truly belonged to the specific group.
The most common anatomic variant was concha bullosa, present in 52.9% of our population, then the Haller cell (in 45.7%) and finally the accessory maxillary ostium (41.4%). They were also calculated for the incidence rates of anatomic variants in male and female population and compared with each other. We did not find statistically significant differences between genders [Table/Fig-9].
Sample structure by anatomic variants.
| Anatomic variation | Total | Male | Female |
|---|
| n | % | n | % | n | % |
|---|
| Concha bullosa | 37 | 52.86 | 19 | 27.15 | 18 | 25.71 |
| Right | 8 | 11.43 | 1 | 1.43 | 7 | 10.00 |
| Left | 6 | 8.57 | 3 | 4.29 | 3 | 4.29 |
| Bilateral | 23 | 32.86 | 15 | 21.43 | 8 | 11.43 |
| Haller’scell | 32 | 45.72 | 18 | 25.71 | 14 | 20.01 |
| Right | 1 | 1.43 | 1 | 1.43 | 0 | 0.00 |
| Left | 8 | 11.43 | 5 | 7.14 | 3 | 4.29 |
| Bilateral | 23 | 32.86 | 12 | 17.14 | 11 | 15.72 |
| Accessory Ostium | 29 | 41.43 | 13 | 18.57 | 16 | 22.86 |
| Right | 9 | 12.86 | 3 | 4.29 | 6 | 8.57 |
| Left | 11 | 15.71 | 5 | 7.14 | 6 | 8.57 |
| Bilateral | 9 | 12.86 | 5 | 7.14 | 4 | 5.72 |
Discussion
There are still many doubts about the radiological definition of chronic maxillary rhinosinusitis. According to Som, sinus mucosa in normal conditions should not be evident and its thickening would be considered pathological [7]. Conversely other authors defined a significant thickening of the sinus mucosa to be normal [12–15]. Rak et al., stated that a mucosal thickening > 3mm can be detected in an asymptomatic patient [12] while Phothikhun et al., concluded that a 5mm thickness in many cases is not accompanied by clinical manifestations [13]. We believe that a correct knowledge of the maxillary inflammatory disease and its radiological presentation has a clinical importance and is of fundamental importance in the planning of certain surgical procedures such as sinus augmentation. As for the mucosal thickening, we used the criteria of Maillet et al., and Lu et al., in which the thickening of the mucosa beyond 2 mm was considered pathological [11,16]. Our data show that a maxillary mucosal thickening ≥ 2mm is statistically associated to CRS according to EPOS2012. We also observed a statistically significant association between healthy patients and maxillary mucosa thickening <2mm [Table/Fig-4]. Therefore, we had considered a thickening of maxillary mucosa ≥ 2mm as pathological.
After establishing a pathological mucosal thickness, we evaluated the relationship between the presence of common anatomical variants and maxillary disease. Among the known anatomical variants we have studied the concha bullosa, the maxillary accessory ostium and Haller cell, because of their easily visible radiological features. The concha bullosa was described for the first time in 1862 by Zuckerlandl who called it a pneumatization of the middle turbinate. Since then many authors have debated its correct definition. Some authors define the concha bullosa as any pneumatization of middle turbinate while others consider it a pneumatization corresponding to 50% of the vertical diameter of the turbinate [1]. In our study, we considered concha bullosa as any pneumatization of middle turbinate. The incidence of concha bullosa varies widely in literature (14-53%) [1]. In our study population, we observed an incidence of 52.9% of concha bullosa with a similar distribution between males and females. Also the incidence of accessory maxillary ostium is widely varied (0-43%) [17] as the incidence of the Haller cell (2-45%) [1,2,5]. We observed an accessory maxillary ostium in 41.4% of the population and an Haller cell in 45.7%. We did not observe a significant prevalence according to gender [Table/Fig-9]. Results of our study and few other authors [1,18], show that anatomic variants analysed are not significantly associated with symptoms of CRS [Table/Fig-8] and furthermore, they are not significantly associated with an abnormal thickening of the maxillary mucosa [Table/Fig-7]
Finally, we observed a significant relationship between the closure of the natural maxillary ostium, pathological thickening of the mucosa and symptoms of CRS. These data, according to Carmeli et al., suggest an evident influence from natural ostium towards the status of maxillary sinus [19]. We believe that, the ostium-infundibulum unit should therefore, be subject to new and more extensive research in order to understand more clearly the pathogenetic mechanisms of chronic maxillary rhinosinusitis. According to other authors we also emphasize the usefulness of CBCT for the radiological study of diseases of the paranasal sinuses [20].
Conclusion
We conclude that in patients with CRS a mucosa maxillary thickening ≥ 2mm, is not associated with the presence of concha bullosa, accessory maxillary ostium and Haller cell. Finally, in patients with CRS and pathological thickening of the maxillary mucosa we observed an association with the closure of the natural maxillary ostium.
Final model
0: Mucosal Thickening< 2
1: Mucosal Thickening ≥ 2
Mucosal Thickening = - 0.16 + 3.82 . Natural Sinus Ostium (Close)
Final model
0: Studygroup
1: Control group
Group = 0.8 - 3.312 . Natural Sinus Ostium (Close)