An Osteologic Study of Cranial Opening of Optic Canal in Gujarat Region
Binita Jigneshkumar Purohit1, Praveen R Singh2
1 Assistant Professor, Department of Anatomy, Pramukhswami Medical College, Karamsad, Anand, Gujarat, India.
2 Professor, Department of Anatomy, Pramukhswami Medical College, Karamsad, Anand, Gujarat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Binita Jigneshkumar Purohit, Assistant Professor, Department of Anatomy, Pramukhswami Medical College, Karamsad, Anand, Gujarat, India.
E-mail: purohitbinita@gmail.com
Introduction
Optic canal is a bony canal situated in between the roots of lesser wings of sphenoid, lateral to body of sphenoid. It transmits optic nerve and ophthalmic artery, surrounded by meninges. Various authors have studied variations in skull foramina and correlated clinically, as variants in the body structures have been found to be associated with many inherited or acquired diseases.
Aim
The present study aimed to examine morphologic and morphometric variations in cranial openings of optic canals.
Materials and Methods
The study was undertaken in total 150 dry adult human skulls. The variations in size, shape, presence or absence and duplication or multiplication if any, in optic canal were observed bilaterally. Unusual features such as recess, fissure and notch were also observed bilaterally. Student’s t-test was applied to compare size of cranial openings of optic canal on both sides. Similarly, morphologic features related with the canal were studied by calculating frequency and proportions of various parameters.
Results
Optic canal was present in all 150 skulls studied bilaterally. The mean maximum dimension of the canal at cranial opening was 5.03±0.72 mm on right side and 5.02±0.76 mm on left side. The shape of the canal was ovoid at cranial opening in all the skulls studied. Duplication of optic canal was present in one skull on left side. Recess was found in 105(35%) sides of total skulls observed. Fissure was found in 20(6.67%) sides and notch was observed in 30(10%) sides of total skulls.
Conclusion
The optic canal showed variability in various parameters. Knowledge regarding variations in size, shape and unusual features on cranial opening of optic canal can be helpful to clinicians while approaching optic canal for various invasive procedures such as optic nerve decompression.
Morphology, Morphometry, Optic nerve
Introduction
Foramina or opening in the skull are very important as many important structures such as nerves and blood vessels traverse through them. Variations in foramina have been studied by various authors. They showed that these variants have been associated with many clinical conditions such as osteopetrosis, osteoporosis, cruzons syndrome, neurofibromatosis, brachymicrocephaly, mental retardation [1–6]. The precise knowledge of variability in human morphology is important to improve diagnostic and interventional procedures in various clinical conditions [6].
Optic canal is located in between two roots of lesser wing of sphenoid and body of sphenoid bone. The anterior border of sulcus chiasmatis leads laterally into optic canal. However, optic chiasma does not occupy this sulcus but lies postero-superior to it. The canal is traversed by optic nerve with its meningeal coverings and ophthalmic artery. Optic canal is one of the channel of communication between orbit and middle cranial fossa. It has two openings i.e., orbital opening and cranial opening [7]. At cranial opening, the shape of optic canal is ovoid. Here, the transverse diameter is greater than the vertical diameter [8].
Optic nerve is the nerve of special sense i.e., vision. It arises from ganglionic neurons of retina and enters orbit through optic canal along with ophthalmic artery. At optic chiasma, shape of the nerve is flattened. However, it becomes rounded as it passes through optic canal. The nerve has a tortuous course within orbit to allow for movements of eyeball [7].
Ophthalmic artery, a branch of internal carotid artery enters orbit through optic canal, inferolateral to optic nerve. The main trunk of the artery continues along medial wall of orbit and divides into terminal branches to supply structures within orbit. The development of ophthalmic artery and middle meningeal artery show a fundamental relationship with development of the embryonic system of stapedial artery. Therefore, anomalies of vascularization of the orbit and dural covering of brain can be correlated. Middle meningeal artery arising from ophthalmic artery is the commonest of these anomalies [9].
The study of optic canal has enormous clinical significance as the optic nerve “The Nerve of Vision” travels through it. Any pathology involving this nerve leads to visual disturbances. The present study aimed to observe variability in morphology and morphometry in cranial opening of optic canal which can be helpful for clinicians while they approach the optic canal for various invasive procedures.
Materials and Methods
The present study was performed in total 150 dry adult human skulls collected from the Department of Anatomy of Pramukhswami medical college, Karamsad; Government medical college, Surat; Government medical college, Baroda; Waghodiya medical college, Baroda; B J medical college, Ahmedabad; Government dental college, Ahmedabad and DD university dental college, Nadiad from December 2012 to November 2015 after obtaining permission from the institutional human research ethics committee.
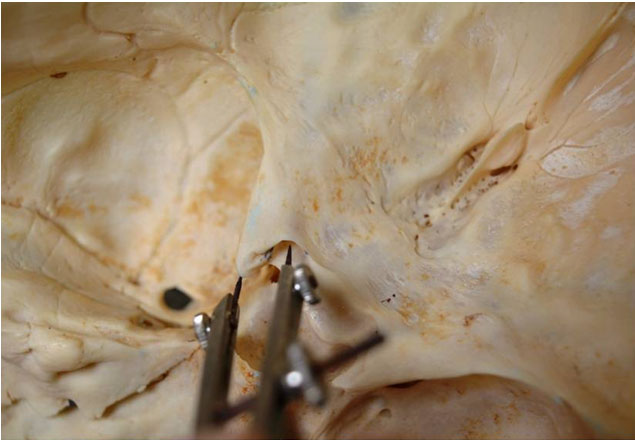
The skulls having crack or fracture lines in the region of orbit were excluded from the study. The presence of optic canal was noted on the both sides of cranial cavity through its cranial aperture. Absence or presence of multiple foramina if any, were noted. The probe (steel wire) was used to confirm patency of foramina and to rule out false passages. Measurement of the canal (at cranial aperture) was taken along the maximum diameter with the help of vernier calliper and geometric compass [Table/Fig-1,2]. The maximum diameter lies along transverse axis of the canal. The measurement from optic canal (canial aperture) to the tip of anterior clinoid process [Table/Fig-3] was also taken on both sides and compared. The shape of the canal was then observed bilaterally. The presence of unusual features (recess, fissure, notch) on the optic canal were observed bilaterally too. Recess [8] is an extension along lateral wall of optic canal having variable length and depth. Fissure [8] is an irregular discontinuity located above the recess. Notch [8] is a gap in posterior-most part of roof of cranial opening having variable size and shape.
Shows two prongs of geometric compass spread apart along maximum diameter of optic canal.

Shows the measurement of optic canal (two prongs spread along maximum diameter) taken with vernier calliper.

Shows two prongs of geometric compass spread from cranial opening of optic foramen to the tip of anterior clinoid process.
All the data were tabulated. Analysis of data was done in SPSS software, version 14. Student’s t-test was applied to compare maximum diameters of the canal on the both right and left sides. The results were considered significant when p-value was ≤0.05. The distribution of shape and other morphological features related to canal were calculated by applying frequency and proportions for each parameter.
Results
[Table/Fig-4] shows comparison of mean maximum diameters of right and left sided optic canal and the mean distance from optic canal (at cranial aperture) to anterior clinoid process. Here, p-value is ≥ 0.05. Hence, there is no statistically significant bilateral difference.
Mean maximum diameter of optic canal/distance (mm).
| Foramen/distance | Right side n=150Mean (SD) | Left side n=150Mean (SD) | p-value |
|---|
| Optic canal | 5.03±0.72 | 5.02±0.76 | 0.887 |
| Distance between optic canal and anterior clinoid process | 7.36±1.06 | 7.20±0.99 | 0.203 |
The shape of the canal at cranial opening was ovoid in all skulls observed. [Table/Fig-5] shows distribution of unusual features on cranial opening of optic canal such as recess, fissure and notch. Duplication of optic canal was observed in one skull on left side out of 150 observed.
Distribution of recess, fissure and notch on cranial opening of optic canal.
| Unusual features | Distribution of unusual features on optic canal |
|---|
| Right siden= 150 | Left siden= 150 | Totaln=300 |
|---|
| Recess | 40(13.34%) | 65(21.67%) | 105(35%) |
| Fissure | 7(2.34%) | 13(4.34%) | 20(6.67%) |
| Notch | 8(2.67%) | 22(7.34%) | 30(10%) |
Discussion
Optic canal is situated in between the two roots of lesser wing of sphenoid, connecting middle cranial fossa with orbit [7,10]. The development of optic canal starts during third fetal month. The development of this foramen is a part of formation of lesser wing of sphenoid. At first, there is formation of cartilaginous foramen. Later on, ossification of cartilaginous foramen occurs. Lastly, bony foramen is converted into optic canal. Formation of optic canal occurs first laterally, then medially and then towards and along the superior margin of this foramen. This development is attributed to formation of optic strut [7,8,10]. The formation of optic foramen into a canal is a slow process which continues during childhood. The developmental arrest at an early or intermediate stage leads to formation of recess and fissure in the lateral wall [8].
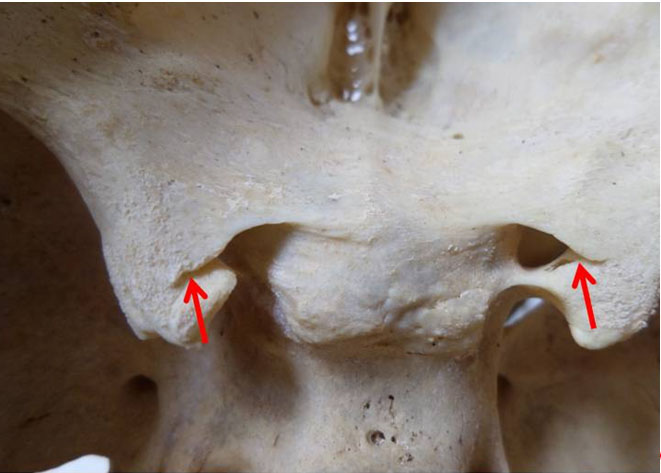
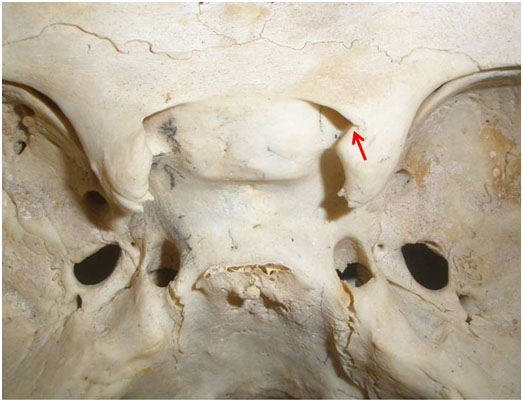
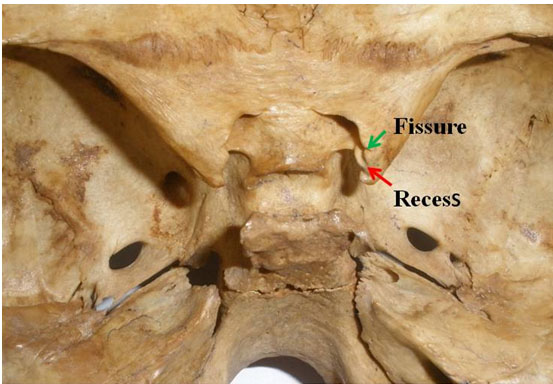
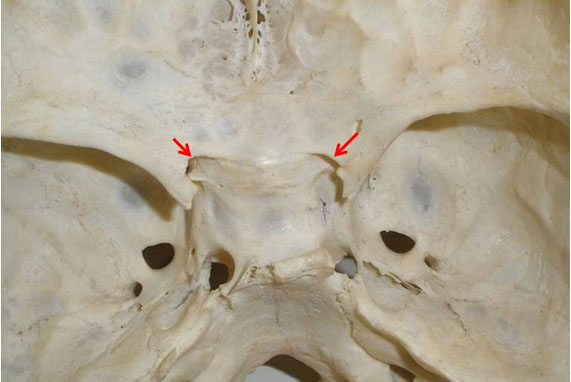
Unusual features such as recess, fissure and notch on cranial opening were observed in present study as shown in [Table/Fig-6,7,8 and 9]. [Table/Fig-6] shows bilateral presence of recesses at the cranial opening of optic canal, while [Table/Fig-7] shows unilateral (right side) presence of recess. The unilateral (right side) presence of recess and fissure is shown in [Table/Fig-8]. Bilateral presence of notches is shown in [Table/Fig-9]. These features have embryological as well as clinical significance while performing invasive procedures through optic canal. However, the incidence of recess (35%), fissure (6.67%) and notch (10%) was less as compared to study performed by Choudhry et al., [8].
Shows bilateral presence of recesses on cranial opening of optic canal (Red arrows).
Shows recess on right cranial opening of optic canal (Red arrow).
Shows presence of recess and fissure on right cranial opening of optic foramen (Red and green arrows).
Shows bilateral presence of notches on cranial opening of optic foramen (Red arrows).
The mean maximum diameter of optic foramen was found similar to that of Gosva et al., [11]. Here, width or transverse diameter of the foramen is taken into consideration. The same diameter in present study was greater than that observed by Orish et al., [12]. Patil et al., [10] found the range of transverse diameter to be 5-10mm which is quite a wide range.
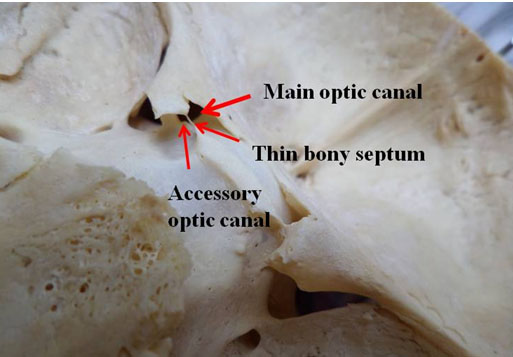
Duplication of optic canal is developmental in origin and the reason for the same is due to anomalous growth of optic strut [10,13]. Duplication of optic canal is rare. It is seen in the both genders and in various races. The larger canal is traversed by the optic nerve the smaller one by ophthalmic artery. Bilateral duplication is a very rare phenomenon which is shown in the study done by some authors [10,14–18]. However, Vanitha et al., and Shinde et al., showed unilateral duplication of the canal [19,20]. The current study presented unilateral duplication of optic canal in one skull (left side) as shown in [Table/Fig-10]. Here, thin bony septum is separating larger main optic canal supero-laterally and smaller accessory canal infero-medially. The larger canal shows presence of recess and the transverse diameter is 5.20mm. The transverse diameter of accessory optic canal is 2.38mm.
Shows thin bony septum separating main optic canal and accessory optic canal on left side (Red arrows).
The comparison of morphometric and morphologic parameters of optic canal with various authors is shown in [Table/Fig-11] [10–18,20].
Comparison of different parameters of optic canal with various researchers [11–18,20].
| Name of researcher | Transverse diameter(mm) | Duplication (%) | Recess (%) | Fissure (%) | Notch (%) |
|---|
| Patil et al, [10] (2011) | 5-10 | 2.75 | - | - | - |
| Gosva et al., [11] (1999) | 4.91±0.49(right side)4.71±0.43(left side) | - | - | - | - |
| Orish et al., [12] (2010) | 4.21±0.11(right side- male)4.04±0.40(left side-male)4.12±0.18(right side-female)4.32±0.20(left side-female) | - | - | - | - |
| Ghai et al., [13] (2012) | - | 2.57 | - | - | - |
| Singh et al., [14] (2005) | - | 4 | - | - | - |
| Choudhary et al., [15] (1999) | - | - | 61.5 | 42.4 | 17.7 |
| Orhan et al., [16] (1996) | - | 0.54 | - | - | - |
| Math et al., [17] (2010) | - | 0.63 | - | - | - |
| Sweta et al., [18] (2014) | - | 4.47 | - | - | - |
| Shinde et al., [20] (2013) | - | 1 | - | - | - |
| Present study (2016) | 5.03±0.72(right side)5.02±0.76(left side) | 0.67 | 35 | 6.67 | 10 |
Optic nerve is formed by axons of ganglion cells of retina. In the intra-canalicular course, dura mater surrounding the nerve is firmly attached to the bone especially in the upper part. The nerve becomes fixed in optic canal, thus not allowing it to be withdrawn into the cranial cavity. Hence, optic nerve becomes vulnerable to injury in cases of fracture of bone or increased intracranial pressure or concussion [8]. Optic nerve can be compressed in direct or indirect maxillo-facial injuries, fibrous dysplasia, osteopetrosis and tumours of this region. Optic nerve decompression is required in such cases where optic canal can be approached through trans-ethmoidal, trans-sphenoidal or supraorbital route. The aim of this procedure is to remove bony wall surrounding the canal so that oedematous optic nerve is relieved from compression by surrounding structures [21–23].
Ophthalmic artery, the first branch of internal carotid artery supplies most intra-orbital structures. The branches of ophthalmic artery which pierce dural sheath and envelop optic nerve are clinically important. The knowledge of relationship of optic nerve with ophthalmic artery is essential to prevent damage to both the structures in orbital surgery [24]. The circulatory variations of ophthalmic artery can be there. Thus, collateral pathways of this artery are important in occlusive carotid vascular disease and interventional radiology [25].
Conclusion
The current study showed variations in size and shape, as well as showed presence of unusual features in the cranial opening of this canal. The duplication of optic foramen is a rare phenomenon which has been observed in this study. The findings of this study will add extra knowledge to neurosurgeons while approaching optic canal for various invasive procedures.
[1]. Singh PR, Raibagkar CJ, Study of variation in atypical foramina of dry human skullNJIRM 2011 2(2):1-5. [Google Scholar]
[2]. Richardson ML, Helms CA, Vogler JB, Genant HK, Skeletal changes in neuromuscular disorders mimicking juvenile rheumatoid arthritis and haemophiliaAJR 1984 143:893-97. [Google Scholar]
[3]. Little BB, Knoll KA, Klein VR, Heller KB, Hereditary cranium bifidum and symmetric parietal foramina are the same entityAm J Med Genet 1990 35(4):453-58. [Google Scholar]
[4]. Reddy AT, Hedlund GL, Percy AK, Enlarged parietal foramina - association with cerebral venous and cortical anomaliesNeurology 2000 54(5):1175-78. [Google Scholar]
[5]. Shaffer LG, Hecht JT, Ledbetter DH, Greenberg F, Familial interstitial deletion 11(p11.12p12) associated with parietal foramina, brachymicrocephaly, and mental retardationAm J Med Genet 1993 45:581 [Google Scholar]
[6]. Ogeng’o J, Clinical significance of anatomical variationsAnatomy Journal of Africa 2013 2(1):57-60. [Google Scholar]
[7]. Standring S, Gray’s Anatomy, The Anatomical Basis of Clinical PracticeIntracranial region 2008 40theditionLondonChurchill Livingstone Elsevier:424-25. [Google Scholar]
[8]. Choudhry S, Kalra S, Choudhry R, Choudhry R, Tuli A, Kalra N, Unusual features associated with cranial openings of optic canal in dry adult human skullsSurg Radiol Anat 2005 27(5):455-58. [Google Scholar]
[9]. Manjunath KY, Anomalous origin of the middle meningeal artery-A reviewJ Anat Soc India 2001 50(2):179-83. [Google Scholar]
[10]. Patil GV, Kolagi S, Padmavathi G, Rairam GB, The duplication of the optic canal in human skullsJournal of Clinical and Diagnostic Research 2011 5(3):536-37. [Google Scholar]
[11]. Govsa F, Erturk M, Kayalioglu G, Pinar Y, Ozer MA, Ozgur T, Neuro-arterial relations in the region of the optic canalSurg Radiol Anat 1999 21(5):329-35. [Google Scholar]
[12]. Orish C, Didia B, Macrometric and micrometric study of sexual dimorphism in the foramina of middle cranial fossa of adult NigeriansInt. J. Morphol 2010 28(2):519-24. [Google Scholar]
[13]. Ghai R, Sinha P, Rajguru J, Jain S, Khare S, Singla M, Duplication of optic canal in human skullsJ Anat Soc India 2012 61(1):33-36. [Google Scholar]
[14]. Singh M, Duplication of optic canal in adult Japanese human skullsJ Anat Soc India 2005 54(2):62-63. [Google Scholar]
[15]. Choudhry R, Anand M, Choudhry S, Tuli A, Meenakshi A, Kalra A, Morphologic and imaging studies of duplicate optic canals in dry adult human skullsSurg Radiol Anat 1999 21(3):201-05. [Google Scholar]
[16]. Orhan MA, Kaynak SR, Bilateral duplication of optic canalsAnn Anat 1996 178(1):61-64. [Google Scholar]
[17]. Math AC, Kulkarni SR, Jatti VKB, Shobha A study of duplication of optic canals in Human adult skulls of North KarnatakaIndian Journal of Forensic Medicine and Toxicology 2010 4(2):1 [Google Scholar]
[18]. Sweta VR, Saravana SK, Accessory optic canal in South Indian dry skullJ Pharm Sci and Res 2014 6(5):224-25. [Google Scholar]
[19]. Vanitha Fatima T, Kadlimatti HS, Unilateral duplication of optic canal. A case reportJournal of Dental and Medical Sciences 2014 13(4):82-83. [Google Scholar]
[20]. Shinde VS, Patil R, Channabasanagouda Mallikarjun M, Study of duplication of optic canal in hundred dry human skull bonesInternational Journal of Biochemical Research 2013 4(11):633-35. [Google Scholar]
[21]. Anand KV, Sherwood C, Mefty O, Optic nerve decompression via transethmoid and supraorbital approachesOperative techniques in Otolaryngology-Head and Neck Surgery 1991 2(3):157-66. [Google Scholar]
[22]. Li J, Wang J, Jing X, Zhang W, Zhang X, Qiu Y, Trans-sphenoidal optic nerve decompression: an endoscopic anatomic studyJ Craniofac Surg 2008 19(6):1670-74. [Google Scholar]
[23]. Locatelli M, Caroli M, Pluderi M, Motta F, Gaini SM, Tschabitscher M, Scarone P, Endoscopic transsphenoidal optic nerve decompression: an anatomical studySurg Radiol Anat 2011 33(3):257-62. [Google Scholar]
[24]. Kocabiyik N, Yazar F, Ozan H, The intraorbital course of ophthalmic artery and its relationship with the optic nerveNeuroanatomy 2009 8:36-38. [Google Scholar]
[25]. Grossman RI, Davis KR, Taveras JM, Circulatory variations of the ophthalmic arteryAJNR 1982 3:327-29. [Google Scholar]