Variation of Cost among Anti-cancer Drugs Available in Indian Market
Bhanu Prakash Kolasani1, Divyashanthi Chellathambi Malathi2, Raghunatha Rao Ponnaluri3
1 Associate Professor, Department of Pharmacology, Vinayaka Missions Medical College and Hospital, Karaikal, Puducherry, India.
2 Associate Professor, Department of Pharmacology, Vinayaka Missions Medical College and Hospital, Karaikal, Puducherry, India.
3 Assistant Professor, Department of Pharmacology, Guntur Medical College, Guntur, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Bhanu Prakash Kolasani, Associate Professor, Department of Pharmacology, Vinayaka Missions Medical College & Hospital, Karaikal, Puducherry, India.
E-mail: kolasanibhanu@yahoo.co.in
Introduction
Although cancer remains a major health problem all over the world, its treatment is limited by affordability of patients in a developing country like India. Information generated from cost analysis studies will be helpful for both the doctors in choosing the correct medicine for their patients and also for policy makers in successfully utilizing the meager resources that are available.
Aim
The aim of the present observational study was to analyse the price variations of anti-cancer drugs available in India.
Materials and Methods
The cost of a particular anti-cancer drug being manufactured by different companies, in the same dose and dosage form, was obtained from latest issue of “Current Index of Medical Specialties” (CIMS) January–April, 2016. The difference between the maximum and minimum prices of various brands of the same drug was analysed and percentage variation in the prices was calculated. The results of the study were expressed as absolute numbers and percentages.
Results
Overall, the price of a total of 23 drugs belonging to 6 different categories available in 52 different formulations were analysed. Among alkylating agents, oxaliplatin (50mg; injection) showed the maximum price variation of 125.02%. In anti-metabolites, methotrexate (2.5mg; tablet) showed the maximum price variation of 75.30%. The maximum price variation among natural products was seen with paclitaxel (260 mg; injection) of 146.98%, among hormonal drugs, was seen with flutamide (250mg; tablet) of 714.24%, among targeted drugs was seen with imatinib mesylate (100mg; film coated tablet) of 5.56% and among supportive drugs, granisetron (1mg; tablet) showed the maximum price variation of 388.68%.
Conclusion
The average percentage variations of different brands of the same anti-cancer drug in same dose and dosage form manufactured in India is very wide. The government and drug manufacturing companies must direct their efforts in reducing the cost of anti-cancer drugs and minimizing the economic burden on the patients.
Alkylating agents, Antimetabolites, Cost analysis, Targeted drugs
Introduction
Cancer is a major health problem responsible for 9% of deaths worldwide. In developed countries like USA, 25% of deaths are related to some form of cancer [1], whereas in India there are 2-2.5 million cases of cancer at any point of time and 0.7 to 0.9 million new cases are being detected every year and approximately half of these cases die [2]. Like in any other country, cancer consumes a major portion of health budget in India also.
Generally, anti-cancer drugs are costlier than any other category of drugs and they substantially contribute to the growing drug expenditure by the patients [3]. There are many causes for the high cost of anti-cancer drugs like high cost of drug development [4], virtual monopoly [5], lack of reduction of cost even after generic versions are available [6], lack of threshold for clinical benefits [7], incentive for more chemotherapy [8] and also the sheer seriousness of the disease as many cancers except the early stage cancers, testicular cancer, and certain blood cancers, are incurable and patients willing to pay any amount of money to get the latest drugs [9].
In developed countries, where a system of medical insurance is in place, it may not be a concern but in developing countries like India, where the medical insurance is only in an emerging stage, affordability to anti-cancer drugs becomes a major concern [10]. The compliance of the patient also significantly depends on the cost of the prescribed medicines [11] and higher cost means a decreased compliance.
Pharmaceutical market in India has over 20,000 medicine formulations [12] and majority of them are sold under brand names [13]. Indian markets are flooded with a huge number of anti-cancer drugs and the same drugs are sold under different brands [14] which puts the prescribing physicians in a difficult state to choose the best drug for a given patient.
Information generated from cost analysis studies will be helpful both for the doctors in choosing the correct medicine for their patients and also for policy makers in successfully utilizing the meager resources that are available [15]. A comprehensive search in various databases and internet was done for studies which analysed the variation of prices among anti-cancer drugs in India and it did not yielded any positive result. So, the present study was done to analyse the variation of cost among different brands of anti-cancer drugs available in the Indian market.
Materials and Methods
The study was done in the Department of Pharmacology of a tertiary care teaching hospital in south India. Latest volume of Current Index of Medical Specialities (CIMS) i.e., January–April, 2016 was used to analyse the prices of anti-cancer drugs.
The cost of a particular anti-cancer drug in the same dose and dosage forms being manufactured by different companies was compared. The drugs manufactured by only one company or by different companies, however, in different strengths were excluded. Formulations containing combination of drugs were also excluded. The difference between the maximum and minimum costs of the same drug manufactured by different pharmaceutical companies was calculated. The following formula was used to calculate the price variation.

Statistical Analysis
The findings of our observational study were expressed as absolute numbers and percentages.
Results
The prices of a total of 23 anti-cancer drugs belonging to 6 different categories available in 52 different formulations were analysed.
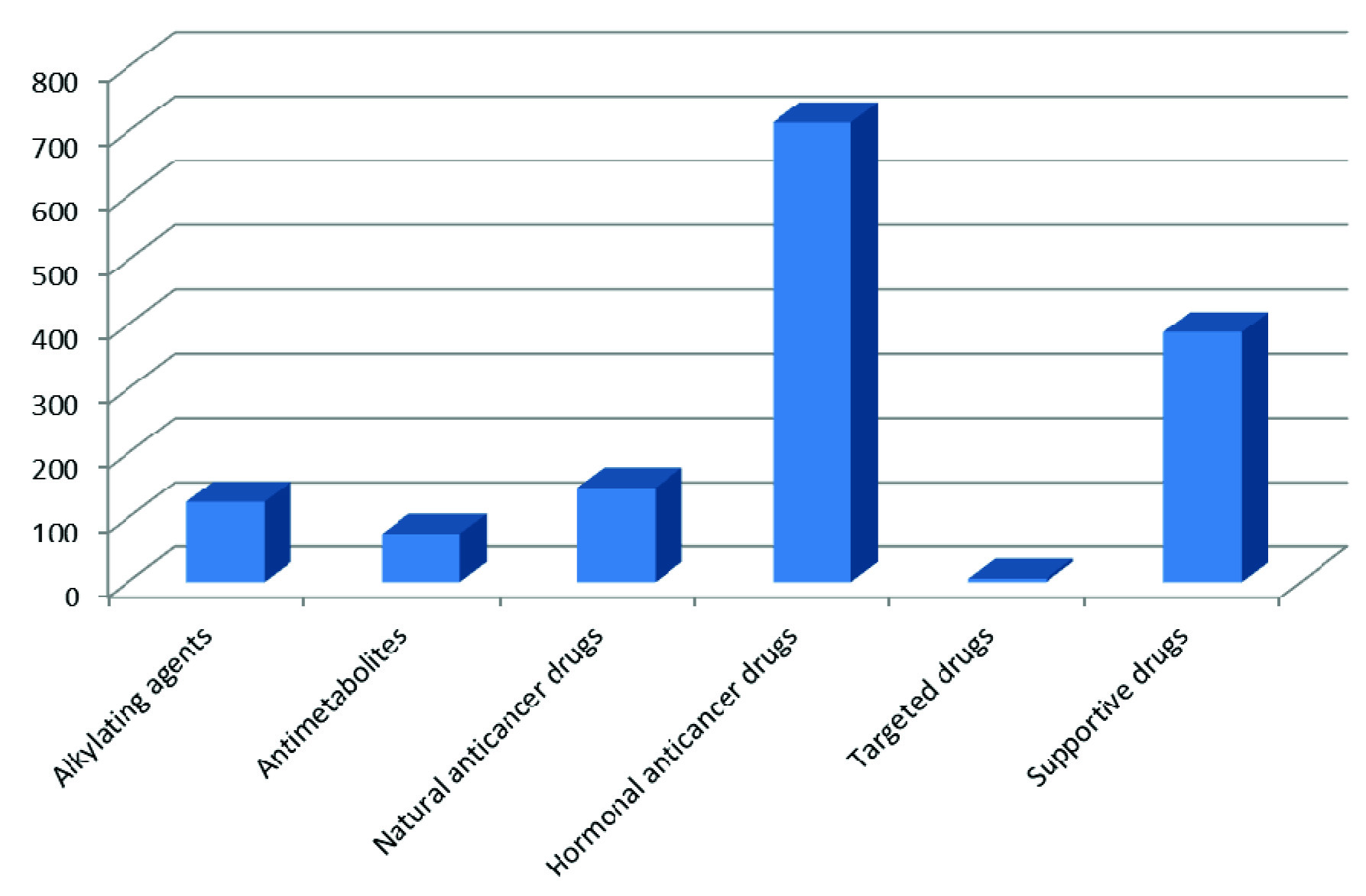
With regard to various categories of anti-cancer drugs analysed in our study, the maximum price variability was found to be highest with hormonal drugs (714.24%) and lowest with targeted anti-cancer drugs (5.56 %) [Table/Fig-1].
Maximum price variability (percentage) among various categories of anti-cancer drugs.
Among alkylating agents, oxaliplatin showed the maximum price variation while cisplatin showed the minimum price variation [Table/Fig-2].
Price variation among alkylating agents.
| S. No | Drug | Dosage form | Dose(mg) | Number ofmanufacturingcompanies | Minimum price(INR)* | Maximum price(INR)* | Price variation |
|---|
| 1. | Busulfan | Tablet | 2 | 2 | 260.12 | 415.00 | 59.54 % |
| 2. | Ifosfamide | Injection | 10002000 | 22 | 377.88775.00 | 551.65936.55 | 45.99 %20.85 % |
| 3. | Cisplatin | Injection | 0.51 | 22 | 76.00316.20 | 86.70360.00 | 14.08 %13.85 % |
| 4. | Oxaliplatin | Injection | 50100 | 44 | 2132.304450.00 | 4798.009495.00 | 125.02 %115.60 % |
*INR: Indian rupees.
In relation to anti-cancer anti-metabolites, methotrexate showed the maximum price variation while gemcitabine showed the minimum price variation [Table/Fig-3].
Price variation among anti-cancer anti-metabolites.
| S. No | Drug | Dosage form | Dose(mg) | Number ofmanufacturingcompanies | Minimum price(INR)* | Maximum price(INR)* | Price variation |
|---|
| 1. | Methotrexate | TabletInjection | 2.557.51550 | 53422 | 33.0071.0090.0046.5060.00 | 57.8584.85125.0859.3569.25 | 75.30 %19.51 %38.98 %27.63 %15.42 % |
| 2. | Fluorouracil | Injection | 250500 | 22 | 10.3019.00 | 13.5022.00 | 31.07 %15.79 % |
| 3. | Cyatarabine | Injection | 1005001000 | 333 | 163.00424.28767.13 | 176.00550.001003.00 | 7.98 %29.63 %30.75 % |
| 4. | Gemcitabine | Injection | 2001000 | 22 | 1493.006145.00 | 1495.006201.00 | 0.13 %0.91 % |
*INR: Indian rupees.
With regard to naturally obtained anti-cancer drugs, paclitaxel showed maximum price variation while epirubicin showed the minimum price variation [Table/Fig-4].
Price variation among naturally obtained anti-cancer drugs.
| S. No | Drug | Dosage form | Dose(mg) | Number ofmanufacturingcompanies | Minimum price(INR)* | Maximum price(INR)* | Price variation |
|---|
| 1. | Doxorubicin | Injection | 1050 | 44 | 205.00920.00 | 265.201188.30 | 29.37 %29.16 % |
| 2. | Daunorubicin | Injection | 20 | 2 | 360.00 | 423.81 | 17.73 % |
| 3. | Epirubicin | Injection | 1050100 | 332 | 403.202012.403906.00 | 522.002200.003906.00 | 29.46 %9.32 %0.00 % |
| 4. | Mitomycin | Injection | 210 | 22 | 95.00395.00 | 207.00540.00 | 117.90 %36.71 % |
| 5. | Paclitaxel | Injection | 30100260300 | 5553 | 1520.004022.004393.0010875.00 | 2100.005500.0010850.0010950.00 | 38.16 %36.75 %146.98 %0.69 % |
| 6. | Docetaxel | Injection | 2080120 | 443 | 3202.7010569.8014000.00 | 4687.5217640.0016354.00 | 46.36 %66.89 %16.81 % |
*INR: Indian rupees
Among hormonal anti-cancer drugs, maximum price variation was seen with flutamide and minimum price variation was seen with anastrazole [Table/Fig-5].
Price variation among hormonal anti-cancer drugs.
| S. No | Drug | Dosage form | Dose(mg) | Number ofmanufacturingcompanies | Minimum price(INR)* | Maximum price(INR)* | Price variation |
|---|
| 1. | Tamoxifen | Tablet | 1020 | 43 | 16.4026.60 | 40.0049.00 | 143.90 %84.21 % |
| 2. | Anastrazole | Tablet | 1 | 3 | 464.00 | 524.29 | 12.99 % |
| 3. | Letrozole | Tablet | 2.5 | 3 | 160.00 | 378.00 | 136.25 % |
| 4. | Flutamide | Tablet | 250 | 3 | 90.51 | 736.97 | 714.24 % |
*INR: Indian rupees.
As far as targeted anti-cancer drugs are concerned, the maximum price variation was seen with imatinib - 100mg; film coated tablet and the minimum price variation was seen with imatinib - 400mg; film coated tablet [Table/Fig-6].
Price variation among targeted anti-cancer drugs.
| S. No | Drug | Dosage form | Dose(mg) | Number ofmanufacturingcompanies | Minimum price(INR)* | Maximum price(INR)* | Price variation |
|---|
| 1. | Imatinib | Film coatedTablet | 100400 | 22 | 9003000 | 9503000 | 5.56 %0.00 % |
| 2. | Gefitinib | Film coatedTablet | 250 | 2 | 3152.13 | 3303.00 | 4.79 % |
*INR: Indian rupees.
Among the supportive drugs used in treatment of cancer patients, the maximum price variation was seen with granisetron whereas the minimum price variation was seen with palanosetron [Table/Fig-7].
Price variation among supportive drugs used in cancer patients.
| S. No | Drug | Dosage form | Dose(mg) | Number ofmanufacturingcompanies | Minimum price(INR)* | Maximum price(INR)* | Price variation |
|---|
| 1. | Ondansetron | TabletMD† TabletSyrupInjection | 4842mg/5ml2mg/ml (2 ml)2mg/ml (4 ml)2mg/ml (10 ml) | 16741318103 | 19.8044.1026.6025.1410.0016.5021.33 | 80.80125.0075.0036.0035.0057.6044.00 | 308.08 %183.45 %181.96 %43.20 %250.00 %249.09 %106.28 % |
| 2. | Granisetron | TabletInjection | 11 | 32 | 16.7830.00 | 82.0040.00 | 388.68 %33.33 % |
| 3. | Palanosetron | Injection | 0.25 | 2 | 138.15 | 140.00 | 1.34 % |
*INR: Indian rupees; †MD: Mouth dissolving.
Discussion
To the best of our knowledge, there was no study done to evaluate the variability of prices of anti-cancer drugs in India. Our study for the first time analysed the variation of cost among different brands of anti-cancer drugs available in the Indian market. Our findings revealed that the prices of various anti-cancer drug formulations showed great variation.
Cancer is associated not only with physical symptoms but also with a tremendous psychological impact [16]. The cost of anti-cancer drugs plays a major influence on the availability and utilization of them by the patients especially in resource poor country like India. Due to lack of information on comparative drug prices and quality, it is difficult for physicians to prescribe the most economical treatment.
The difference in cost between the various brands of the same drug varies from two fold to more than 100-fold [17]. There are various reasons for this price variation which include majority of them being under patent protection and also the present market for new chemical entities being monopolistic in nature. In this market structure, the sellers retain appreciable influence over the price of a product [18]. Prescribing physicians are usually influenced by information provided to them in the form of formularies, promotional literature and marketing tactics of the medical representatives of that particular brand. The notion that new drug is always better than old drugs is also prevalent among physicians which need not be true always. This kind of biased information restricts both prescribers and patient’s choices [18]. Lack of information on quality, non-availability and conflicts of interest are also responsible for physicians not prescribing the least expensive medication. Manufacturing companies claim high cost of research involved in developing new anti-cancer drugs as a reason for higher pricing of drugs.
There are many middlemen involved in the process of a drug reaching to the consumer after it gets manufactured. Even though many times, the manufacturing cost of a particular anti-cancer drug is less, these middlemen who are involved in distribution and retail sale of drugs because of their bargaining power and based on demand are quite often responsible for high and indiscriminate variability of prices seen among various drugs [19].
Differences in guidelines of drug regulating authorities of various countries and their pricing policies account for the varying prices of drugs among different countries. Drug Price Control Order (DPCO) is an order issued by the Indian government in 2013 to fix the price of drugs, which covers 680 formulations at present. Once any medicine is brought under the purview of DPCO, it cannot be sold at a price higher than that fixed by the government [20]. In the past few years, the number of medicines that are under DPCO have been decreasing slowly due to which the cost of drugs are escalating [21,22].
Even in developed counties like US, the problem of variation and high costs of anti-cancer drugs is highly prevalent. For example, in one study done by Guirgis HM et al., where the value of anti-cancer drugs in metastatic castrate-resistant prostate cancer were studied, it was found that generic docetaxel had the lowest costs and cost/outcome whereas other drugs like abiraterone, enzalutamide and cabazitaxel were overpriced for their values [23]. In another study, it was found that the launch prices of many new anti-cancer drugs are unrelated to the magnitude of the expected health benefits. For example in 2011, Bristol-Myers Squibb set the price of its newly approved melanoma drug, ipilimumab at $120,000 for a course of therapy with an increase in life expectancy of only four months [24].
A study done by Siddique M et al., have found that lack of true generic price check and high cost of generic cancer drugs also are the problems present in developed countries too [25]. A study done by Mailankody S et al., in US found that price of cancer drugs is independent of novelty and current pricing models are not rational [26]. Even a recent study done by Vogler S et al., has found that the price of new cancer drugs varies widely from 28% to 388% between high-income countries like 16 European countries, Australia and New Zealand. The greatest differences in price were noted for gemcitabine followed by zoledronic acid, interferon alfa 2b and gefitinib. Overall, prices of various anti-cancer drugs were found to be low in Greece and were high in Sweden, Switzerland, and Germany [27].
There are various interventions or changes in policies advised that can help in lowering the cost of anti-cancer drugs like breaking the monopoly in anti-cancer drug manufacturers, changing the regulatory guidelines by government agencies in favour of those companies which manufacture cheaper anti-cancer drugs and making the new anti-cancer drug approvals faster, increasing the cost effectiveness ratio of anti-cancer drugs [28], achieving a balance between physician autonomy in prescribing anti-cancer drugs and costs incurred by patients [29], encouraging non-profit generic companies which manufacture anti-cancer drugs by giving them tax incentives and other measures, value based reimbursement by medical insurance companies [30] and bringing more anti-cancer drugs under DPCO.
So, it becomes the need of the hour by not only government, but also by all the stake holders like NGOs, health care providers and general public to make a concerted effort in order to put pressure on the pharmaceutical manufacturing companies whereby the prices of both branded and generic drugs can be brought down and can be made affordable to common man.
Limitation
The limitation of this study is that the price variations among formulations containing combination of drugs were not analysed. We were also unable to compare the prices of many anti-cancer drugs as they were manufactured by only one company.
Conclusion
This study shows that there is a wide variation in the prices of most of the anti-cancer drugs available in India. Health care providers must be aware of availability of low cost brands or generics available among anti-cancer drugs and prescribe accordingly based on the economic status of the patient for successful treatment of cancers. There is an urgent need to decrease the cost of anti-cancer drugs by the government in order to save many lives due to cancer related mortality.
*INR: Indian rupees.
*INR: Indian rupees.
*INR: Indian rupees
*INR: Indian rupees.
*INR: Indian rupees.
*INR: Indian rupees; †MD: Mouth dissolving.
[1]. Stone MJ, Aronoff BE, Evans WP, Fay JW, Lieberman ZH, Matthews CM, History of the baylor Charles A. Sammons cancer centerProc (Bayl Univ Med Cent) 2003 16:30-58. [Google Scholar]
[2]. Park K, Epidemiology of chronic non-communicable diseases and conditionsIn: Parks text book of preventive and social medicine 2009 Vol. 620 th edJabalpur, MP, IndiaM/S Banarasi Das Bhanot Publishers:332-35. [Google Scholar]
[3]. Suda KJ, Motl SE, Kuth JC, Inpatient oncology. Length of stay and hospital costs: Implications for rising inpatient expendituresJ Appl Res 2006 6:127 [Google Scholar]
[4]. DiMasi JA, Grabowski HG, Economics of new oncology drug developmentJ Clin Oncol 2007 25(2):209-16. [Google Scholar]
[5]. DiMasi JA, Feldman L, Seckler A, Wilson A, Trends in risks associated with new drug development: success rates for investigational drugsClinic Pharmacol Ther 2010 87(3):272-77. [Google Scholar]
[6]. Karaca-Mandic P, McCullough JS, Siddiqui MA, Van Houten H, Shah ND, Impact of new drugs and biologics on colorectal cancer treatment and costsJ Oncol Pract 2011 7(3 suppl):e30s-7s. [Google Scholar]
[7]. Jabbour E, Cortes JE, Kantarjian HM, Suboptimal response to or failure of imatinib treatment for chronic myeloid leukemia: what is the optimal strategy?Mayo Clin Proc 2009 84(2):161-69. [Google Scholar]
[8]. Jacobson M, Earle CC, Price M, Newhouse JP, How Medicare’s payment cuts for cancer chemotherapy drugs changed patterns of treatmentHealth Aff (Millwood) 2010 29(7):1391-99. [Google Scholar]
[9]. Moreno-Aspitia A, Perez EA, Treatment options for breast cancer resistant to anthracycline and taxaneMayo Clin Proc 2009 84(6):533-45. [Google Scholar]
[10]. Meropol NJ, Schulman KA, Cost of cancer care: Issues and implicationsJ Clin Oncol 2007 25:180-86. [Google Scholar]
[11]. Rao KS, Nundy M, Dua AS, National Commission on Macroeconomics and HealthFinancing and Delivery of Health Care Services in India 2005 New DelhiMinistry of Health & Family Welfare, Government of India, Delivery of Health Services in the Private Sector:89-104. [Google Scholar]
[12]. Sakthivel S, Access to essential drugs and medicines. In: Lal PG (Ed.)National Commission on Macroeconomics and Health 2005 New DelhiMinistry of Health:185-210. [Google Scholar]
[13]. Jadhav NB, Bhosale MS, Adhav CV, Cost analysis study of oral antidiabetic drugs available in Indian marketInt J Med Res Health Sci 2013 2(1):63-69. [Google Scholar]
[14]. Sundaram VM, Pharma industry in IndiaDrugs News Perspect 2008 21(1):59-63. [Google Scholar]
[15]. Adam T, Evans DB, Murray CJL, Cost Effectiveness and Resource Allocation 2003 1:3Available from: http://www.resource-allocation.com/content/1/1/3. [Last accessed on 2009 Aug 11] [Google Scholar]
[16]. Jakobsen JC, Gluud C, Kongerslev M, Larsen KA, Sorensen P, Winkel P, Third-wave cognitive therapy versus mentalisationbased treatment for major depressive disorder. A randomized clinical trialBMC Psychiatry 2014 4(8):232 [Google Scholar]
[17]. Lofolm PW, Katzug BG, Rational prescribing and prescription writing. In: Katzug BG (Ed.)Basic and Clinical Pharmacology9th ednNew YorkMcGraw-Hill:1091-100. [Google Scholar]
[18]. Roy V, Gupta U, Agarwal K, Cost of medicines and their affordability in private pharmacies in Delhi (India)Indian J Med Res 2012 136(5):827-35. [Google Scholar]
[19]. Das SC, Mandal M, Mandal SC, A critical study on availability and price variation between differrent brands: Impact on access to medicinesIndian Journal of Pharmaceutical Sciences 2007 69(1):160-63. [Google Scholar]
[20]. Annual report of Department of pharmaceuticals 2014-15. http://pharmaceuticals.gov.in/sites/default/files/AnnualReport201415.pdf [Google Scholar]
[21]. Paunikar AP, Bhave KA, Cost analysis of oral antidepressant drugs available in IndiaNatl J Physiol Pharm Pharmacol 2015 5(5):367-71. [Google Scholar]
[22]. Kumar V, Gupta NV, Kumar KA, A comparison between old and latest systems in DPCOInternational Journal of Pharmacy and Pharmaceutical Sciences 2014 6(2):19-20. [Google Scholar]
[23]. Guirgis HM, The value of anticancer drugs in metastatic castrate-resistant prostate cancer: economic tools for the community oncologistJ Community Support Oncol 2015 13(10):362-66. [Google Scholar]
[24]. Howard DH, Bach PB, Berndt ER, Conti RM, Pricing in the market for anti-cancer DrugsJournal of Economic Perspectives 2015 29(1):139-62. [Google Scholar]
[25]. Siddiqui M, Rajkumar SV, The high cost of cancer drugs and what we can do about ItMayo Clinic Proceedings 2012 87(10):935-43. [Google Scholar]
[26]. Mailankody S, Prasad V, Five years of cancer drug approvals: innovation, efficacy, and CostsJAMA Oncol 2015 1(4):539-40. [Google Scholar]
[27]. Vogler S, Vitry A, Babar ZU, Cancer drugs in 16 European countries, Australia, and New Zealand: a cross-country price comparison studyLancet Oncol 2015 17:39-47. [Google Scholar]
[28]. Learn PA, Bach PB, Pem and the cost of multicycle maintenanceJ Thorac Oncol 2010 5(8):1111-12. [Google Scholar]
[29]. de Souza JA, Polite BN, Zhu S, Utilization and costs of non-evidence-based (non-EBM) antineoplastic agents in patients with metastatic colon cancer (mCC)ASCO Meeting Abstracts 2011 29:6002 [Google Scholar]
[30]. Russell LB, Gold MR, Siegel JE, Daniels N, Weinstein MC, The role of cost-effectiveness analysis in health and medicine: Panel on cost-effectiveness in health and medicineJAMA 1996 276(14):1172-77. [Google Scholar]