Renal Cell Carcinoma with Unusual Skeletal Metastasis to Tibia and Ankle: A Case Report and Review of Literature
Kiran Shankar1, Durgesh Kumar2, Kariyanakatte Veeraiah Veerendra Kumar3, Chennagiri Premlata4
1 Senior Resident, Department of Surgical Oncology, Kidwai Memorial Institute of Oncology, Bangalore, Karnataka, India.
2 Senior Resident, Department of Surgical Oncology, Kidwai Memorial Institute of Oncology, Bangalore, Karnataka, India.
3 Professor, Department of Surgical Oncology, Kidwai Memorial Institute of Oncology, Bangalore, Karnataka, India.
4 Associate Professor, Department of Pathology, Kidwai Memorial Institute of Oncology, Bangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Durgesh Kumar, Room no 102, Married Doctors Accommodation, Shanthidhama, Kidwai Memorial Institute of Oncology, Banglore-560029, Karnataka, India.
E-mail: dr.durgesh06@gmail.com
Renal Cell Carcinoma (RCC) accounts for 5% of the epithelial malignancies worldwide with clear cell carcinoma accounting for 85% of these malignancies. One third of these patients experience synchronous metastatic disease and 20-30% of the remaining patients experience metachronous metastatic RCC. Bony metastasis accounts for 20% of metastatic RCC. They most commonly affect the axial skeleton and rarely the long bones or the small bones of the hands and feet. Bone metastases from RCC are predominantly osteolytic in nature, leading to significant patient morbidity due to the associated Skeletal Related Events (SRE). SREs may significantly decrease patient quality of life. Bone pain is most common SRE and radiotherapy is most common form of treatment. Only 2% of the patients require surgery. Here we present a case of advanced RCC with tibial and ankle metastasis who presented to us after one year of radical nephrectomy with severe pain and inability to walk and underwent above knee amputation.
Amputation, Bony metastasis, Epithelial malignancies
Case Report
A 67-year-old male patient, presented to the Department of Surgical Oncology with severe pain in his left knee and inability to walk since, 2 months. He had undergone a left radical nephrectomy one year ago for left Renal Cell Carcinoma (RCC) at our institute and the final histopathology was clear cell variant of RCC. Patient had been asymptomatic for the last 8 months and was not on any treatment after the surgery. Examination revealed a diffuse bulge in the region of the upper tibia and the ankle with restriction of the movement of the left leg. Diffuse tenderness was present around the lesion with a Visual Analogue Score (VAS) of 8-9/10. X-Ray (anterior-posterior and lateral view) of the knee suggested a complete destruction of the upper end of the metaphysis of the tibia with a soft tissue reaction. A working diagnosis of a metastatic deposit was made in view of the previous history of RCC.
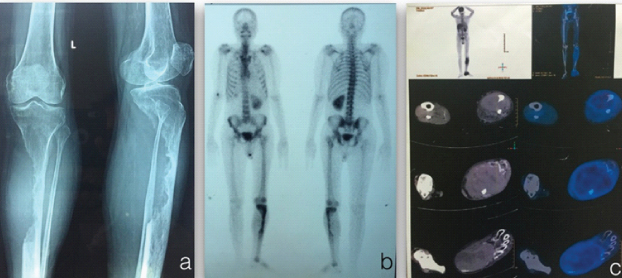
A Positron Emission Tomography (PET) scan was ordered to look for other areas of metastasis [Table/Fig-1]. To our surprise there were only two areas of metastasis i.e., left upper end of tibia and the ankle. Fine Needle Aspiration Cytology (FNAC) of the soft tissue reaction showed the possibility of a poorly differentiated carcinoma, suspicious of a metastatic deposit from the RCC.
(a) X-ray antero-posterior/lateral view of the knee showing cortical destruction of the proximal tibia and thinning of the fibula; (b,c) PET-CT showing activity in both the proximal and distal end of the tibia with minimal activity in the renal bed (suggestive of post-operative changes).
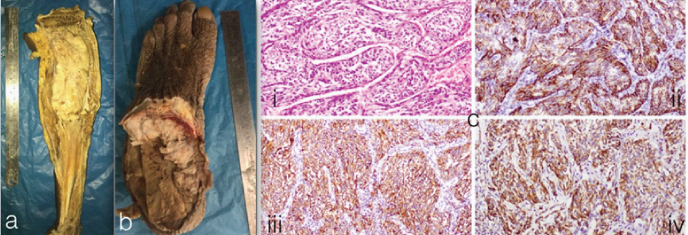
With the above investigation, a decision of above knee amputation was taken, upon counseling the patient. The patient underwent planned procedure. Post-operative recovery and rehabilitation was uneventful. The final histopathology report revealed a RCC and was confirmed by immunohistochemistry [Table/Fig-2]. Patient was started on adjuvant sunitinib 50mg daily per oral every day for four weeks with a gap of two weeks and was disease free at one year of follow-up.
(a,b) Gross examination showing tumour in the upper tibial metaphysis and in the ankle joint; (c) Metastatic renal cell carcinoma on histopathology with the characteristic (i) alveolar pattern (ii) Immunohistochemistry showing positive for cytokeratin (iii) CD10 (iv) vimentin.
Discussion
Bone metastases are more commonly seen in breast and prostate cancers, accounts for 60-70% of cases while lung, thyroid and RCC metastasize to bone in 30-40% of advance cases. Approximately one third of the newly diagnosed RCC presents with the synchronous metastasis disease and additional 30-40% patients develop metastasis eventually. The most common sites of metastatic RCC are the lung (75% of cases), liver (40%), bone (40%), soft tissue (34%), and pleura (31%) [1]. On a detailed pubmed search we found less than 20 cases of such cases. In the year 2010 three cases of tibia metastasis were reported from a retrospective study from Munich [2] and one case reported from India in 2012 [3].
RCC has a high mortality rate, with a five year survival rate of <10%. The bone remains one of the most common distant metastatic sites of RCC either synchronous or metachronous presentation. The mechanism of tumour growth in bone is complex and involve tumour driven stimulation of osteoclast, osteoblast and other components of the bone, leading to significant patient morbidity due to the associated Skeletal Related Events (SREs). SREs are defined as pathological fractures, bone pain, impending fracture, spinal cord and nerve root compressions and hypercalcemia. SREs may significantly decrease patient quality of life [4].
Patient’s quality of life is negatively impacted by bone damage due to developing bone metastases, causing severe pain and poor performance status. Moreover, there are not any proved systemic chemotherapeutic agents active against metastatic RCC. Surgery is the best form of palliation in case of bony metastasis unless contra-indicated.
Improved disease free and overall survival have been reported with metastasectomy in RCC but majority of these studies are retrospective [4]. In a series of 278 patients from Memorial Sloan Kettering Cancer Center (MSKCC) with metachronous metastasis, 211 were reported to have either complete or incomplete resection from variety of metastatic sites. They have reported, a 5 year survival of 44% vs 14% in patients who underwent complete resection. Multivariate analysis also identified several factors associated with good outcome including: (1) a solitary metastatic lesion (2) age less than 60 years (at the time of presentation of the metastatic disease) (3) disease free interval of more than 1 year and in case of pulmonary metastasis tumour size less than 4cm. Although not supported by convincing evidence from randomised trials yet various studies showed good improvement in Overall Survival (OS) and Disease Free Survival (DFS) after resection of isolated metastatic lesions [5].
Patients with bony metastasis from RCC have better prognosis, as compared to other tumours like lung cancer but inferior to breast and prostate cancer. Lack of effective chemotherapeutic drugs, is possibly the main reason for the poor prognosis of RCC with bony metastasis [6]. Patients with solitary bone metastasis from RCC reportedly have the best prognosis, with a 5 year-survival rate between 35% and 60%. Owing to the longer survival of patients with solitary bone metastasis, a number of authors recommend an aggressive surgical approach with curative intent to prevent local disease progression [7].
Sunitinib is a multiple tyrosine kinase inhibitor, recommended for use in metastatic RCC. Various studies have shown increased disease free survival of more than 2 years and with prolonged treatment have even better survival with acceptable complications like rashes, hypothyroidism and hypertension. Recommended dose of sunitinib is 50mg daily per oral every day for four weeks with a gap of two weeks, which constitutes one cycle for one year or until the patient developed complications. Prolonged treatment with sunitinib is not associated with any increased severity of dose related toxicity or appearance of new side effects except hypothyroidism [8].
Various other options for treatment exist in treating solitary bony metastatis including radiotherapy, angiography and embolisation (RCC metastatic tumours are vascular). The aim of resorting to surgical resection in this case was for palliation and for the fact that, there were synchronous metastases in the same limb. To the best of our knowledge this is the only case in literature to present with unilateral synchronous metastasis to the tibia and the ankle in a metachronous fashion.
Conclusion
Bone metastases from RCC are predominantly osteolytic in nature, leading to significant patient morbidity due to the associated skeletal related events. Bone pain is most common SRE and radiotherapy is most common form of treatment. Only 2% of the patients require surgery. Early recognition and careful evaluation of the symptoms is required for diagnosis and early treatment to prevent the complications and achieve good quality of life.
[1]. Prasad SR, Humphrey PA, Catena JR, Narra VR, Srigley JR, Cortez AD, Common and uncommon histologic subtypes of renal cell carcinoma: imaging spectrum with pathologic correlationRadio Graphics 2006 26:1795-810. [Google Scholar]
[2]. Fottner A, Szalantzy M, Wirthmann L, Stähler M, Baur-Melnyk A, Jansson Bone metastases from renal cell carcinoma: patient survival after surgical treatmentBMC Musculoskeletal Disorders 2010 11:145 [Google Scholar]
[3]. Anand M, Deshmukh SD, Gulati HK, Devasthali DA, Bilateral renal cell carcinoma presenting as fracture tibiaIndian J Cancer 2012 49:316-17. [Google Scholar]
[4]. Russo P, Snyder M, Vickers A, Kondagunta V, Motzer R, Cytoreductive nephrectomy and complete metastasectomy for metastatic renal cancerSCI World J 2007 7:768-78. [Google Scholar]
[5]. Murthy SC, Kim K, Rice TW, Rajeswaran J, Bukowski R, DeCamp MM, Can we predict long term survival after pulmonary metastasectomy for renal cell carcinoma?Ann Thorac Surg 2005 79:996-1003. [Google Scholar]
[6]. Lin PP, Mirza AN, Lewis VO, Cannon CP, Tu SM, Tannir NM, Patient survival after surgery for osseous metastases from renal cell carcinomaJ Bone Joint Surg Am 2007 89(8):1794-801. [Google Scholar]
[7]. Zekri J, Ahmed N, Coleman RE, Hancock BW, The skeletal metastatic complications of renal cell carcinomaInt J Oncol 2001 19:379-82. [Google Scholar]
[8]. Porta C, Gore ME, Rini BI, Escudier B, Hariharan S, Charles LP, Long-term safety of Sunitinib in Metastatic Renal Cell CarcinomaEur Urol 2016 69(2):345-51. [Google Scholar]