Cephalometric analyses comprises of various angular and linear measurements which assist the clinician in recognizing antero- posterior discrepancies. Down introduced the A-B plane angle to determine the sagittal denture base relationship whereas, Riedel recommended the use of SNA, SNB, and ANB angles [1,2]. The ANB angle is most commonly manipulated and well recognized indicator for skeletal sagittal discrepancy [3,4]. Several authors elucidated the shortcomings of ANB due to number of distorting factors [4–9] and recommended linear measurements to be made on occlusal plane [5,6] while others endorsed linear or angular measurements on palatal plane, Maxillary-Mandibular Bisector (MMB) and Frankfort Horizontal (FH) plane [10–12]. Some authors suggested other measurements to analyze anterio-posterior discrepancies but all these used cranial or dental reference plane [13,14]. Each one of these planes had its own limitations.
In determining the apical base relationship and for comparison of pre- and post-treatment sagittal correlation of the jaws, an assessment independent of cranial reference planes or dental occlusion would be a preferable supplement. In this context, beta angle was originated by Baik CY which does not depend on any cranial landmark or dental occlusion to evaluate the sagittal jaw relationship [15]. It would be especially valuable where the previously established cephalometric measurements, such as ANB angle and the Wit’s appraisal (point A and B projects in two perpendicular lines, along the functional occlusal plane called as AO and BO. The plane in between AO and BO is referred to as the Wit’s appraisal), cannot be accurately used because of its dependence on varying factors (length of SN plane, jaw rotation, occlusal plane etc.). Beta angle indicates the severity and the type of skeletal dysplasia in the sagittal dimension and it can be useful in evaluating the growth pattern of the patient. Any alteration in Frankfort-Mandibular Plane Angle (FMA) values may also modify the beta angle [16]. Sundareswaran S et al., in their analytical work determined that the vertical growth patterns significantly increased Beta angle values; thus, influencing its authenticity as a sagittal discrepancy appraisal tool [16]. Consequently, Beta angle may not be a substantial tool for assessment of sagittal jaw discrepancy in patients manifesting vertical growth patterns with skeletal Class I and Class II malocclusions. Therefore, it is a fundamental need to study the impact of Beta angle on the growth pattern. The parameters used for evaluation of skeletal malocclusion also show ethnic variation [17–21]. Hence, the present study was undertaken to evaluate correlation of Beta angle with antero-posterior dysplasia indicators and FMA in skeletal Class I, Class II and Class III group and to establish norms of Beta angle. The objectives that were taken into consideration were to evaluate the normal values of beta angle for skeletal Class I, II and III malocclusions; the correlation of Beta angle with ANB, App-Bpp, Wit’s appraisal and MMB in skeletal Class I, Class II and Class III malocclusion groups and the correlation of beta angle with FMA.
Materials and Methods
After obtaining the institutional ethical clearance from the institute and informed consent from all the participants, the present cross- sectional institution based study was conducted in Department of Orthodontics and Dentofacial Orthopaedics of Swami Devi Dyal Dental College and Hospital, Barwala, Haryana, India, for a period of 9 months. Pre-treatment lateral head cephalograms of 120 subjects in age group of 15-25 years belonging to Haryana/Punjab population were obtained. Determination of sample size was done using a power calculation that is based upon mean Beta angle value of Class I occlusion i.e., 31.1±2° [15]. To identify a change of 2° from this mean value with 95% confidence and 80% power, a minimum sample size of 16 in each group was required. Out of 120 cephalograms, 40 each for skeletal Class I, skeletal Class II and skeletal Class III group were assorted. The distribution of cases into these three categories was achieved using existing antero-posterior indicators of skeletal malocclusion (ANB, MMB, App-Bpp, Wit’s, FMA).
Subjects in the permanent dentition stage and those with completed pre-treatment records taken within a period of 6 months were included in the study. The exclusion criteria for the study were patients having craniofacial anomalies, previous history of trauma, orthodontic treatment or orthognathic surgery and functional mandibular shifts or congenital defects.
Cephalometric Radiograph and Analyses: The 120 selected pre-treatment lateral head cephalogram were traced manually on an acetate paper with a 3H drawing pencil. Landmarks, planes, angular and linear measurements used in the study were:
Cephalometric Planes [Table/Fig-1]:
Cephalometric plane considered in the study.
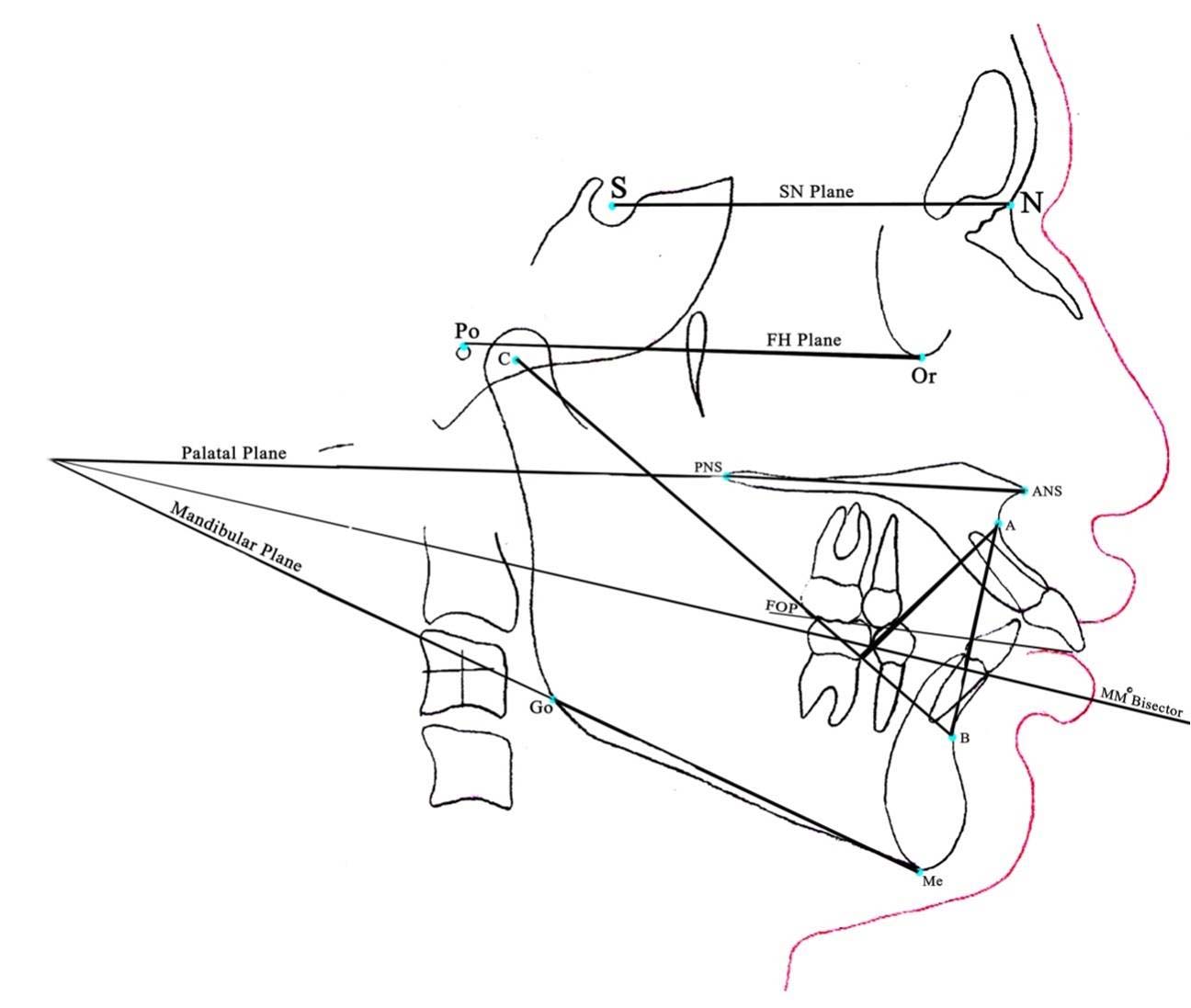
Sella-Nasion (SN) plane: The line connecting S and N.
Frankfort Horizontal (FH) plane: The line connecting Po and Or.
Functional Occlusal Plane (FOP): Drawn through the cuspal overlap of maxillary first molar and bicuspids.
C-B line: Line connecting the centre of the Condyle (C) with point B.
A-B line: Line connecting A and B points.
Line from point A perpendicular to C-B line.
Line bisecting mandibular and palatal plane.
Line connecting ANS and PNS.
Linear Measurements [Table/Fig-2]:
Linear measurements considered in the study.
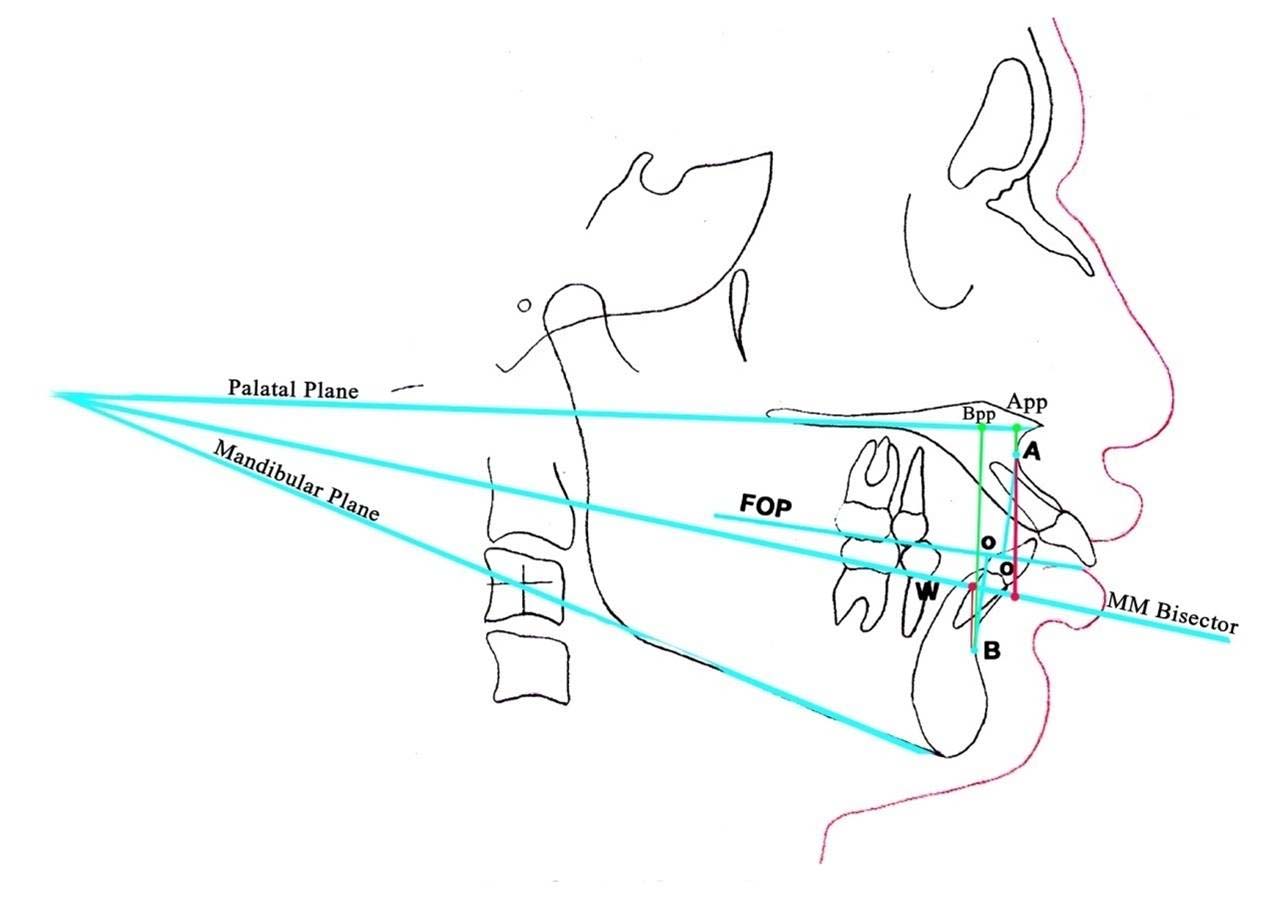
AO-BO (mm): The distance between perpendiculars drawn from point A and point B on to the occlusal plane [5,6].
Values for skeletal Class I: -1mm to 2 mm
MMB (mm): The distance between perpendiculars drawn from point A and B on to bisector plane of mandibular and palatal plane [11].
Value for skeletal Class I: -4mm
App-Bpp (mm): The distance between perpendiculars drawn from point A and B on to palatal plane [12].
Value for skeletal Class I: 4.8±3.6mm
Angular Measurements [Table/Fig-3]:
Angular measurements (1-Beta angle, 2-SNA, 3-SNB, 4-ANB and 5-FMA angle) considered in the study.
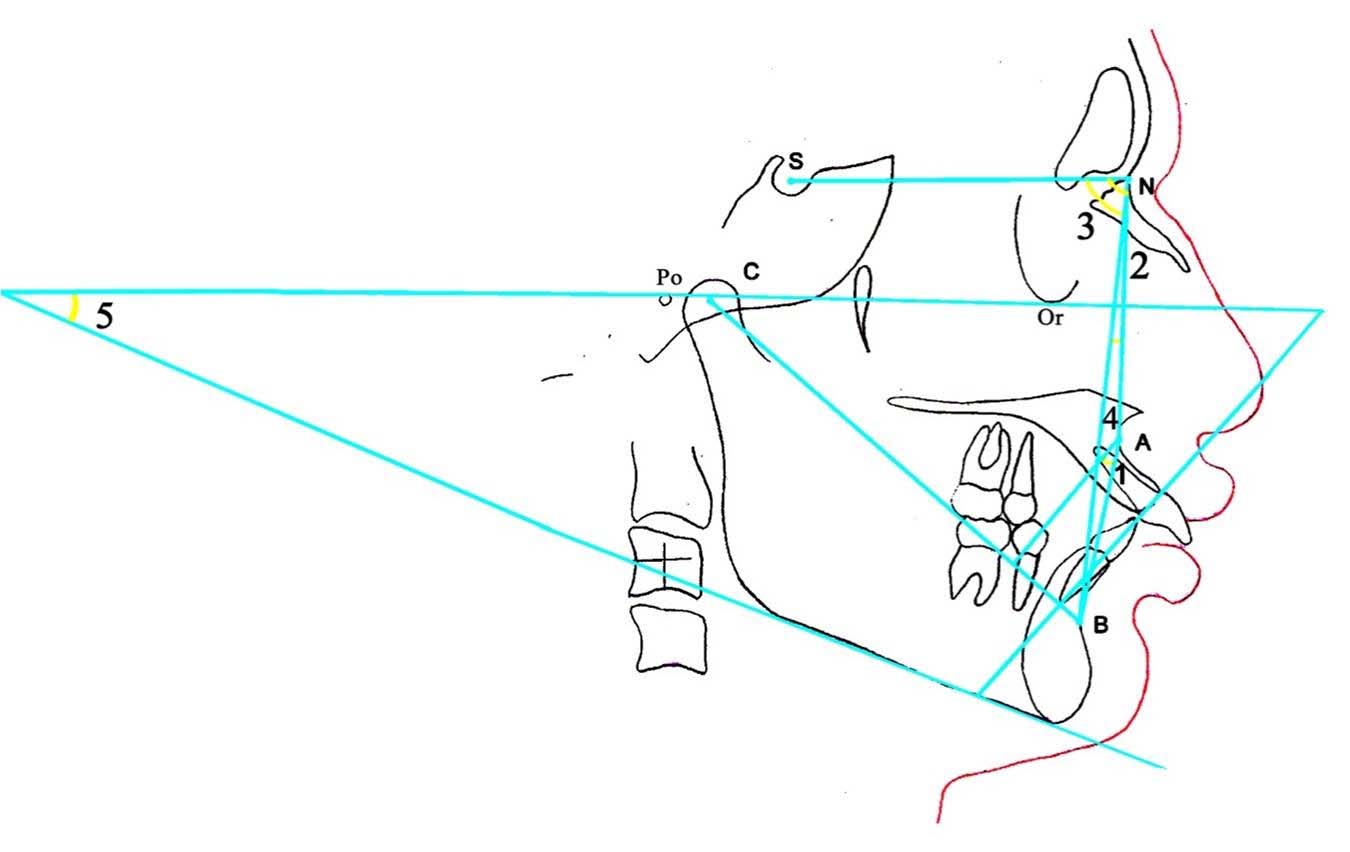
Beta angle: Angle formed between A-B line and the perpendicular line dropped from point A and C-B line [15].
SNA-The angle from sella to nasion to point A.
SNB-The angle from sella to nasion to point B.
ANB-The angle from point A to nasion to point B, SNA-SNB difference.
Value for skeletal Class I: 2°±2°.
FMA-The angle formed between Frankfort horizontal plane and mandibular plane (Tweed’s).
Statistical Analysis
All measurements were entered into SPSS software package (version 15.0) and mean standard deviation was obtained. Analysis of variance (ANOVA) and unpaired t-test was used to determine the difference between mean Beta angle values in all three skeletal classes. Bivariate correlations among different parameters of these groups were also obtained.
Results
Out of total 120 subjects enrolled in the present study, each of skeletal Class I, II and III malocclusion groups had 40 subjects (33.3%). The cephalometric analysis was conducted and measurement of Beta angle and other antero-posterior indicators of malocclusion were done.
Establishment of Normative Data for Beta Angle: The beta angle measurement was done on the lateral cephalogram for all the 120 subjects enrolled in the study. [Table/Fig-4] shows the range (minimum and maximum) of beta angle measurements in different skeletal Class groups with calculated mean and standard deviation values.
Beta angle measurements in different skeletal class groups.
| S. No. | Skeletal Class | N | Mean | SD | Median | Min | Max | 95% CI |
|---|
| Lower Bound | Upper Bound |
|---|
| 1. | I | 40 | 31.33 | 3.25 | 32 | 26 | 42 | 30.28 | 32.37 |
| 2. | II | 40 | 25.28 | 4.28 | 25 | 17 | 35 | 23.90 | 26.65 |
| 3. | III | 40 | 40.93 | 4.55 | 40 | 28 | 50 | 39.47 | 42.38 |
N: Number of subjects, SD: Standard Deviation
Comparision of Measurements of Beta Angle in Skeletal Class I, II and III Malocclusion Groups: Analysis of variance and mean differences were calculated to compare the skeletal Class I, the skeletal Class II and skeletal Class III groups which showed a statistically significant intergroup difference (p<0.001) [Table/Fig-5]. Comparison of beta angle, showed a mean difference of 6.05° between Class I and Class II, -9.60° between Class I and Class III and -15.65° between Class II and Class III groups. This comparison between the groups revealed that skeletal Class I had significantly higher mean beta angle as compared to skeletal Class II but had a significantly lower mean value as compared to Class III (p<0.001) [Table/Fig-6].
Analysis of variance (ANOVA) of beta angle in skeletal Class I, II and III.
| Sum of Squares | Df | Mean Square | F | Sig. |
|---|
| Between Groups | 4982.47 | 2 | 2491.23 | 150.592 | <0.001 |
| Within Groups | 1935.53 | 117 | 16.54 | | |
| Total | 6917.99 | 119 | | | |
Comparison of mean differences using unpaired t-test in beta angle measurements in Skeletal Class I, II and III., p<0.001: Statistically highly significant
| S.No. | Comparison | Meandifference | SE of Meandifference | "t" | p |
|---|
| 1. | Class I vs Class II | 6.05 | 0.85 | 7.112 | <0.001 |
| 2. | Class I vs Class III | -9.60 | 0.88 | -10.858 | <0.001 |
| 3. | Class II vs Class III | -15.65 | 0.99 | -15.840 | <0.001 |
On the basis of above evaluation, the increasing order of beta angle values were observed in different malocclusion groups as follows:
Class III > Class I > Class II.
Correlation of Beta Angle with Wit’s Appraisal, ANB, App-Bpp, MMB and FMA in Skeletal Class I, Class II and Class III Groups: Overall beta angle showed a strong negative correlation with all the other variables except FMA [Table/Fig-7]. Only MMB showed significant correlation for skeletal Class I, followed by ANB and Wit’s with the existence of weak correlation, whereas for App-Bpp and FMA the correlation was not significant [Table/Fig-8]. For skeletal Class II, the correlation of beta angle with all parameters (ANB, Wit’s App-Bpp, FMA and MMB) was non-significant and among them MMB shows strongest correlation [Table/Fig-9]. For skeletal Class III, beta angle showed a strong significant correlation with all the indicators (ANB, Wit’s, MMB, App-Bpp) except FMA. The result of correlation matrix confers very weak co-relation of FMA with beta angle [Table/Fig-10]. The findings of the present study revealed that beta angle show weak correlation with FMA in all types of malocclusion groups.
Overall correlation matrix showing bivariate correlation among different parameters under evaluation.
| ANB | Wit’s | MMB | App-Bpp | FMA | Beta Angle |
|---|
| r | p | r | p | r | p | r | p | r | p | r | p |
|---|
| ANB | 1.000 | <0.001 | 0.840 | <0.001 | 0.865 | <0.001 | 0.878 | <0.001 | 0.247 | 0.007 | -0.865 | <0.001 |
| Wit’s | | | 1.000 | <0.001 | 0.879 | <0.001 | 0.833 | <0.001 | 0.113 | 0.220 | -0.856 | <0.001 |
| MMB | | | | | 1.000 | <0.001 | 0.899 | <0.001 | -0.012 | 0.893 | -0.904 | <0.001 |
| App-Bpp | | | | | | | 1.000 | <0.001 | 0.283 | 0.002 | -0.830 | <0.001 |
| FMA | | | | | | | | | 1.000 | <0.001 | -0.020 | 0.827 |
| Beta Angle | | | | | | | | | | | 1.000 | <0.001 |
r: Correlation coefficient, p<0.001: Statistically highly significant
Correlation matrix showing bivariate correlation among different parameters under evaluation for skeletal Class I.
| ANB | Wit’s | MMB | App-Bpp | FMA | Beta Angle |
|---|
| r | p | r | p | r | p | r | p | r | p | r | p |
|---|
| ANB | 1.000 | <0.001 | 0.399 | 0.011 | 0.395 | 0.012 | 0.612 | <0.001 | 0.356 | 0.024 | -0.300 | 0.060 |
| Wit’s | | | 1.000 | <0.001 | 0.207 | 0.201 | 0.043 | 0.794 | -0.020 | 0.903 | -0.331 | 0.037 |
| MMB | | | | | 1.000 | <0.001 | 0.370 | 0.019 | -0.151 | 0.351 | -0.656 | <0.001 |
| App-Bpp | | | | | | | 1.000 | <0.001 | 0.587 | <0.001 | -0.108 | 0.508 |
| FMA | | | | | | | | | 1.000 | <0.001 | 0.197 | 0.222 |
| Beta Angle | | | | | | | | | | | 1.000 | <0.001 |
r: Correlation coefficient, p<0.001: Statistically highly significant
Correlation matrix showing bivariate correlation among different parameters under evaluation for skeletal Class II.
| ANB | Wit’s | MMB | App-Bpp | FMA | Beta Angle |
|---|
| r | p | r | p | r | p | r | p | r | p | r | p |
|---|
| ANB | 1.000 | <0.001 | 0.076 | 0.641 | -0.083 | 0.612 | 0.190 | 0.240 | 0.407 | 0.009 | -0.241 | 0.134 |
| Wit’s | | | 1.000 | <0.001 | 0.202 | 0.212 | 0.267 | 0.096 | 0.233 | 0.147 | -0.140 | 0.390 |
| MMB | | | | | 1.000 | <0.001 | 0.344 | 0.030 | -0.170 | 0.295 | -0.350 | 0.027 |
| App-Bpp | | | | | | | 1.000 | <0.001 | 0.443 | 0.004 | 0.050 | 0.760 |
| FMA | | | | | | | | | 1.000 | <0.001 | 0.247 | 0.125 |
| Beta Angle | | | | | | | | | | | 1.000 | <0.001 |
r: Correlation coefficient, p<0.001: Statistically highly significant
Correlation matrix showing bivariate correlation among different parameters under evaluation for skeletal Class III.
| ANB | Wit’s | MMB | App-Bpp | FMA | Beta Angle |
|---|
| r | p | r | p | r | p | r | p | r | p | r | p |
|---|
| ANB | 1.000 | <0.001 | 0.636 | <0.001 | 0.717 | <0.001 | 0.650 | <0.001 | -0.115 | 0.481 | -0.782 | <0.001 |
| Wit’s | | | 1.000 | <0.001 | 0.786 | <0.001 | 0.649 | <0.001 | -0.300 | 0.060 | -0.829 | <0.001 |
| MMB | | | | | 1.000 | <0.001 | 0.790 | <0.001 | -0.510 | 0.001 | -0.840 | <0.001 |
| App-Bpp | | | | | | | 1.000 | <0.001 | -0.032 | 0.845 | -0.783 | <0.001 |
| FMA | | | | | | | | | 1.000 | <0.001 | 0.280 | 0.080 |
| Beta Angle | | | | | | | | | | | 1.000 | <0.001 |
r: Correlation coefficient, p<0.001: Statistically highly significant
Discussion
The present study showed that the beta angle had a value of 31.33±3.25° for skeletal Class I group, 25.28±4.28° for skeletal Class II group, 40.93±4.55° for skeletal Class III group. For the beta angle, any value < 28° indicates Class II skeletal pattern and any value > 35° indicates Class III skeletal pattern. These results are in accordance with the norms for Caucasian population given by Baik CY et al., who introduced beta angle as a powerful tool to assess sagittal discrepancies [15]. Similarly, Prasad M et al., designed a study to validate the norms of beta angle to assess the sagittal discrepancy for Nellore district population. There was statistically significant difference for beta angle within the three skeletal patterns and no difference among Nellore district population and Caucasian norms [22]. Zeng ZS et al., reported ethnic differences among Asian and Caucasian population using various cephalometric variables [23]. On contrary, beta angle may not be a definitive tool for evaluating the sagittal jaw discrepancy in patients exhibiting vertical growth patterns in skeletal Class I and Class II malocclusions according to Sundareswaran S et al. However, it is a reliable indicator of sagittal dysplasia in normal and horizontal growth patterns. Additionally, skeletal Class III malocclusions showed complete adherence to beta angle values irrespective of the growth pattern [16].
A study also compared cephalometric mean values of Saudi population with the norms suggested for a white Caucasian population by Down’s and Steiner’s and significant differences were noticed [19]. Another research work encountered significant differences between white and black subjects using various hard tissues, dental and soft tissue variables [20]. Singh SP et al., established cephalometric norms for North Indians and compared those measurements with Caucasians. In this study North Indians had more retruded maxilla and mandible, more facial convexity as compared to the Caucasians. Upper incisor inclination and wit’s value were also more among North Indians; whereas, Caucasians had more values of maxillary and mandibular lengths, chin depth, vertical skeletal and dental heights [21]. There are several other studies in literature presenting distinct cephalometric norms for different populations [17,18].
Analysis of variance and mean differences were calculated to compare the Skeletal Class I, the Skeletal Class II and Skeletal Class III groups. Analysis of variance showed a statistically significant intergroup difference (p<0.001). Beta angle showed strong correlation with all anterio-posterior dysplasia parameters. Thus, beta angle gives equally good assessment of skeletal malocclusion. Moreover, in the present study, the beta angle showed strongest correlation with MMB which indicates both can be used interchangeably with less chance of error.
The correlation of beta angle with FMA in the present study was very weak or non-significant. Thus, the assumption that the increase or decrease in FMA may affect the values of beta angle has been proved false. We conclude that the beta angle can be used efficiently without any effect of FMA and it is not dependent on growth pattern.
Limitation
The limitation of the present study was that we have assumed point A to be constant in the present study, but in real it changes, which further modify the value of beta angle. This part has not been considered in the study. As the present study was conducted on Haryana/ Punjab population, the collected data can be used in future for further research on the particular population group. Certainly, prospective studies are mandatory to assess the vertical change in the position of point A with its effect on beta angle.
Conclusion
The normal values of beta angle in the three skeletal malocclusion groups are in the same range as mentioned in previous studies. Thus, the study interprets the stability of beta angle irrespective of the difference in craniofacial morphology. The overall beta angle showed a strong correlation with ANB, MMB, App-Bpp and Wit’s; thus, can be used interchangeably in diagnosis of skeletal malocclusion. Beta angle can be used efficiently without any effect of FMA. The growth pattern does not affect the interpretation of malocclusion using beta angle.
N: Number of subjects, SD: Standard Deviation
r: Correlation coefficient, p<0.001: Statistically highly significant
r: Correlation coefficient, p<0.001: Statistically highly significant
r: Correlation coefficient, p<0.001: Statistically highly significant
r: Correlation coefficient, p<0.001: Statistically highly significant