Good oral health is important for overall well-being of the individuals and community. It requires the retention of deciduous as well as permanent teeth as long as possible, because teeth are important for mastication, phonetics and aesthetics. Thus, oral health is an imperative aspect of quality of life, but it is still the most neglected as oral diseases are not considered life threatening [1]. With changing times, life expectancy of the people is increasing all over the world and the same can be reflected in India too. In India, life expectancy has increased from 23 years in 1901 to 32 years in 1951; from 63 years in 2001 to 66 years in 2011 [2]. This implies that there can be more people surviving for longer time and with considerable amount of accumulated oral diseases. Therefore, there arises the need for retention of tooth in the oral cavity for longer time in order to regulate the various functions of the dentition.
Tooth retention is considered as a complex phenomenon, because studies conducted in the past have shown that, it is influenced by the cultural beliefs, socio-economic status and other behavioural variables [3]. Understanding these various factors affecting tooth retention can help us to develop the strategies for intervention to prevent tooth loss. Further, studies related to tooth retention will have more benefits than the studies conducted on tooth mortality for assessment of the efficiency of the impaired dentition [4]. Therefore, studies on tooth retention can provide ideas not only on the oral health status of the people but also on the magnitude of the oral problems. Moreover, studies on tooth retention can also help in determining the arch and tooth showing maximum retention and also the teeth commonly lost at an early age. Such information will help the health and social policy-makers to translate the knowledge on tooth retention into action programs for improving the oral health of the people.
Simultaneously, many studies have been conducted previously in Indian context related to tooth loss as compared to studies on tooth retention [5]. This implies that, there is a paucity of information pertaining to factors influencing tooth retention.
Hence, the present study was designed to determine the influence of various factors on tooth retention among the adult population of Dharwad district, India.
Materials and Methods
Study Area: The present cross-sectional study was conducted in urban and rural areas of Dharwad district. This district has an area of 4,263 km2 comprising five talukas namely Dharwad, Hubli, Kalaghatgi, Navalgund and Kundagol with 390 rural areas and 6 urban areas. For administrative purposes, the urban areas are further divided into wards by municipal authorities [6].
Study Population: Study subjects belonged to the age group of 18-59 years from urban and rural areas of Dharwad district. They were distributed according to the demographic profile of India. According to this profile, a greater percentage of population is distributed among the lower age groups and lesser percentage in the higher age groups.
Sample Size Determination: The population of Dharwad district, as obtained from Dharwad district statistics office was 16,04,253 (Population Census of India, 2001). The urban and rural populations in this district were 8,81,917 and 7,22,336 respectively, which was distributed at the ratio of 56:44 [6]. The sampling frame for age group 18-59 years age group was approximately 9,00,000. Results of pilot study showed tooth retention to be 45%. Using this, sample size was calculated with the formula.

From the above formula, a total sample size (n) =1056 was obtained which was approximated to a final sample size of 1100. Out of this, urban and rural samples were calculated as per the demographic profile of Dharwad district as 616 urban and 484 rural subjects.
Sampling Procedure: A multistage, random sampling procedure was followed and the study area was divided into two clusters of urban and rural area.
Urban Area: In the first stage, out of 6 urban areas, 4 urban areas were randomly selected by lottery method. In the second stage, among the selected urban areas, wards were identified from which few wards were randomly selected, and in the third stage among the selected wards, few households were identified from which suitable subjects for the study were selected. Thus, the data was collected from a total of 616 urban subjects, using self-designed questionnaire through interview and oral examination methods.
Rural Area: A similar procedure was followed to select the study subjects from the rural areas. In the first stage, a total of 390 rural areas were listed. In the second stage, a total of 11 villages were selected randomly. In the third stage, among the selected 11 villages, few households were identified from which suitable subjects for the study were selected. Thus, the data was collected from a total of 484 rural subjects selected, using self-designed questionnaire through interview and oral examination methods.
Methodology: Prior to start of the current study, ethical clearance was obtained from the Institutional Review Board, SDM Dental College, Dharwad, following which, official permission was taken from the District Health and Family Welfare Office of Dharwad District and their co-operation was sought for this study. The study was scheduled during the period of May 2011 to July 2011 from 10:00 AM to 5:00 PM. Informed consent was obtained from all the study participants.
The data was collected using a form which was prepared pertaining to the objectives of the study. Language used in the questionnaire was English. Face validity of the questionnaire was 0.73 and reliability as estimated by Cronbach’s alpha was 0.82. Single investigator who was trained and calibrated performed all oral examinations (Kappa=0.90).
Initially, study samples were subjected to face-to-face interview to collect the information regarding their socio-demographic factors, daily oral hygiene practices which included type, materials used, frequency, time, method and duration of brushing, frequency of change of tooth brush and use of any other oral hygiene aids; and dietary practices, adverse oral habits and the frequency of dental visits. Once the interview was completed, oral cavity examination was carried out among the study subjects to record the number of teeth remaining in the oral cavity. However, tooth retention was recorded for all the natural teeth with the exclusion of third molars.
Further, for the analysis of data; Income groups were classified into 5 groups: ≤5000, 5001-10000, 10001-15000, 15001-20000 and >20000 and also family size was classified into two categories, one with 1-5 members and other with ≥6 members. This is supported by the data that average Indian family size is 4.62 [7].
The following codes were provided for recording the tooth retention:
1=Sound tooth, 2=Carious tooth, 3=Root canal treated teeth, 4=Teeth with any form of fillings, 5=Teeth with crowns, 6=Grade I or Grade II mobile tooth, 7=Missing teeth, 8=Any others
All the instruments used for oral examination were sterilized in the Central Sterile Supplies Department (CSSD), S.D.M College of Dental Sciences and Hospital, Dharwad, before proceeding for the survey. An average number of 25 to 30 subjects were interviewed and examined per day. Interview and oral examination of single subject took about 10-15 minutes in most of the instances.
Statistical Analysis
The data were statistically analyzed by applying the one way ANOVA, unpaired t-test and backward stepwise multiple regression using the statistical package – STATA 10.0 version. The normality of data was assessed using the Kolmogorov-Smirnov test. Karl Pearson’s correlation coefficient was used to test the correlation between the two quantitative variables. The statistical significance was set at 5% level of significance (p≤0.05).
Results
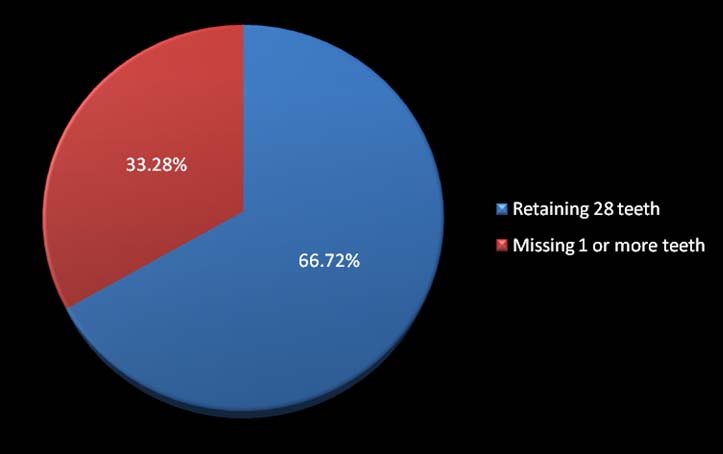
The results showed that 66.72% subjects retained all the 28 teeth [Table/Fig-1] and mean number of teeth retained were 25.33 (90.46%). There was gradual reduction in tooth retention with increase in age. Males (95.8%) compared to females (94.07%) and unmarried (98.8%) than married study subjects (93.3%) retained more teeth. Tooth retention was comparatively higher among the subjects with intermediate or post high school diploma (97.5%) than those who were illiterate (89.5%) and other low educational level study subjects. Further mean values of tooth retention for other socio demographic factors i.e., occupation, income and family size were not statistically significant [Table/Fig-2].
Distribution of tooth retention among the study subjects
Comparison of socio-demographic factors with tooth retention among study subjects.
| Socio Demographic Factors | Number of Study Subjects(n) | Mean Values of Tooth Retention | Std. Dev. |
|---|
| Age Groups | 18-27 years | 453(41.1%) | 27.80(99.2%) | 0.64 |
| 28-37 years | 272(24.7%) | 27.37(97.7%) | 1.32 |
| 38-47 years | 182(16.5%) | 26.60(95%) | 2.45 |
| 48-57 years | 157(14.2%) | 23.70(84.6%) | 5.80 |
| ≥58 years | 36(3.2%) | 21.17(75.6%) | 6.99 |
| F-value=100.349, p=0.000*, One way ANOVA *(p≤ 0.05) statistically significant |
| Gender | Male | 762(69.2%) | 26.85(95.8%) | 2.89 |
| Female | 338(30.7%) | 26.34(94.07%) | 4.03 |
| t-value=2.110, p=0.035*, Student’s t-test *(p≤ 0.05) statistically significant |
| Occupation | Unemployed | 437(39.7%) | 26.67(95.2%) | 3.67 |
| Unskilled | 170(15.4%) | 26.15(93.3%) | 3.80 |
| Semi skilled worker | 174(15.8%) | 27.08(96.7%) | 2.11 |
| Skilled worker | 103(9.3%) | 26.97(96.3%) | 2.07 |
| Clerk, shop or farm owner | 128(11.6%) | 26.81(95.7%) | 2.89 |
| Semi profession | 64(5.8%) | 26.39(94.2%) | 4.23 |
| Profession | 24(2.1%) | 27.08(96.7%) | 1.55 |
| F-value=1.481, p=0.181, One way ANOVA *(p≤ 0.05) statistically significant |
| Income Groups | ≤5000 | 660(60%) | 26.57(94.8%) | 3.56 |
| 5001-10000 | 292(26.5%) | 26.88(96%) | 2.78 |
| 10001-15000 | 60(5.4%) | 27.08(96.7%) | 1.95 |
| 15001-20000 | 46(4.1%) | 27.06(96.6%) | 1.95 |
| >20000 | 42(3.8%) | 26.40(94.2%) | 4.41 |
| F-value=0.901, p=0.463, One way ANOVA *(p≤ 0.05) statistically significant |
| Education | Illiterate | 117(10.6%) | 25.07(89.5%) | 5.24 |
| Primary school | 86(7.8%) | 26.59(94.9%) | 3.02 |
| Middle school | 125(11.3%) | 26.38(94.2%) | 3.31 |
| High school | 328(29.8%) | 26.68(95.2%) | 3.38 |
| Intermediate or post high school diploma | 214(19.4%) | 27.32(97.5%) | 2.01 |
| Graduate | 213(19.3%) | 27.17(97%) | 2.63 |
| Professional or post graduate | 17(1.6%) | 27.12(96.8%) | 1.83 |
| F-value=7.288, p=0.000*, One way ANOVA *(p≤ 0.05) statistically significant |
| Marital Status | Married | 709(64.4%) | 26.14(93.3%) | 3.76 |
| Unmarried | 391(35.5%) | 27.69(98.8%) | 1.81 |
| t value = -9.201, p=0.000*, Student’s t-test *(p≤ 0.05) statistically significant |
| Family size | 1-5 | 730 | 26.63(95.1%) | 3.45 |
| ≥6 | 370 | 26.81(95.7%) | 2.92 |
| t value = -0.894, p=0.371, Student’s t-test *(p≤ 0.05) statistically significant |
In addition, it was observed that subjects using tooth brush (96.6%) and tooth paste (96.6%) for cleaning the teeth [Table/Fig-3] and subjects practicing mixed diet (96.6%) showed statistically significant greater tooth retention [Table/Fig-4]. Further, subjects who never visited the dentist (96.5%) in their lifetime showed statistically significant greater tooth retention than study subjects who visited the dentist infrequently (92.7%) [Table/Fig-4].
Comparison of oral hygiene practices with tooth retention among study subjects.
| Oral Hygiene Practices | Number of Study Subjects(n) | Mean Values of Tooth Retention | Std. Dev. |
|---|
| Type of Aid | Brush | 891(81%) | 27.07(96.6%) | 2.41 |
| Finger | 195(17.7%) | 25.11(89.6%) | 5.33 |
| Twig | 14(1.2%) | 25.07(89.5%) | 6.51 |
| F-value=31.845, p=0.000*, One way ANOVA *(p≤ 0.05) statistically significant |
| Materials Used | Tooth paste | 872(79.2%) | 27.06(96.6%) | 2.48 |
| Tooth powder | 103(9.3%) | 25.51(91.1%) | 4.70 |
| Charcoal | 103(9.3%) | 25.02(89.3%) | 5.44 |
| Others | 22(2%) | 25.45(90.8%) | 5.60 |
| F-value=18.918, p=0.000*, One way ANOVA *(p≤ 0.05) statistically significant |
Comparison of type of diet and visit to dentist with tooth retention among study subjects.
| Type of diet and visit to dentist | Number of Study Subjects(n) | Mean Values of Tooth Retention | Std. Dev. |
|---|
| Type of Diet | Vegetarian | 440(40%) | 26.15(93.3%) | 4.14 |
| Mixed | 660(60%) | 27.06(96.6%) | 2.51 |
| t-value=-4.147, p=0.000*, Student’s t-test *(p≤ 0.05) statistically significant |
| Visit to Dentist | Never visited | 749(68.09%) | 27.04(96.5%) | 2.85 |
| Infrequently | 351(31.91%) | 25.97(92.7%) | 3.98 |
| t-value=5.093, p=0.000*, Student’s t-test *(p≤ 0.05) statistically significant |
A significant positive correlation was found between education (r=0.172, p=0.00), marital status (r=0.225, p=0.00), frequency of change of brush (r=0.184, p=0.00) and type of diet (r=0.136, p=0.00) in relation to tooth retention among the study subjects (p≤0.05). However, a significant negative correlation was observed between age (r=-0.476, p=0.00), gender (r=-0.072, p=0.017), type of aid (r=0.227, p=0.00), material used for teeth cleaning (r=-0.208, p=0.00), smoking habits (r=-0.077, p=0.009) and visit to dentist (r=-0.151, p=0.00) in relation to tooth retention among the study subjects (p≤0.05) (r=observed value, p=significance level) [Table/Fig-5].
Correlation coefficient between tooth retention and various factors by Karl Pearson’s method.
| Factors | Correlation Coefficient | p-value |
|---|
| Location | 0.011 | 0.706 |
| Age | -0.476 | 0.000* |
| Gender | -0.072 | 0.017* |
| Education | 0.172 | 0.000* |
| Occupation | 0.023 | 0.440 |
| Income/month(family) | 0.027 | 0.357 |
| Marital status | 0.225 | 0.000* |
| Number of family members | 0.025 | 0.397 |
| Religion | 0.002 | 0.939 |
| Type of aid in cleaning | -0.227 | 0.000* |
| Material used | -0.208 | 0.000* |
| Frequency of brushing | 0.015 | 0.600 |
| Method of brushing | 0.036 | 0.229 |
| Duration of brushing | 0.035 | 0.234 |
| Frequency of change of brush | 0.184 | 0.000* |
| Use of other aid | -0.022 | 0.465 |
| Type of diet | 0.136 | 0.000* |
| Frequency of sweet consumption | -0.037 | 0.219 |
| Chewing habits | 0.006 | 0.821 |
| Smoking Habits | -0.077 | 0.009* |
| Alcohol habits | -0.004 | 0.883 |
| Visit to dentist | -0.151 | 0.000* |
Results of regression analysis are presented in [Table/Fig-6]. Chewing habits, frequency of change of brush, occupation, type of diet and method of brushing were found to have positive influence and age, visit to dentist, marital status and type of aid used in cleaning were found to have negative influence on the tooth retention respectively.
Estimates of backward step wise linear regression of tooth retention by different variables.
| Independent Variables | BETA | SE of BETA | Regression Coefficient | Standard Error | t-value | p- value |
|---|
| Intercepts | | | 29.679 | 0.705 | 42.072 | 0.000* |
| Age | -0.49 | 0.03 | -1.361 | 0.092 | -14.663 | 0.000* |
| Visit to dentist | -0.12 | 0.03 | -0.841 | 0.191 | -4.399 | 0.000* |
| Chewing habits | 0.08 | 0.03 | 0.334 | 0.110 | 3.026 | 0.002* |
| Frequency of change of brush | 0.10 | 0.03 | 0.360 | 0.123 | 2.929 | 0.003* |
| Marital status | -0.09 | 0.03 | -0.601 | 0.221 | -2.719 | 0.006* |
| Occupation | 0.07 | 0.03 | 0.136 | 0.051 | 2.663 | 0.007* |
| Type of aid in cleaning | -0.08 | 0.04 | -0.591 | 0.271 | -2.181 | 0.029* |
| Type of diet | 0.05 | 0.03 | 0.365 | 0.175 | 2.084 | 0.037* |
| Method of brushing | 0.05 | 0.03 | 0.134 | 0.072 | 1.979 | 0.050* |
Discussion
Study results showing gradual decrease in tooth retention with increase in age among the Dharwad subjects implies that with increasing age, long standing oral diseases might have a cumulative effect on dentition [8], eventually leading to decrease in tooth retention. There may be several other factors such as multiple chronic diseases, side effects of medications and psychological factors as depression and isolation (because of loss of spouse, friends and feeling of being unwanted by family) leading to neglect of personal and oral hygiene resulting in higher tooth loss among the aged people [9]. Above findings were in agreement with the other studies [10–12].
It is particularly noteworthy that the males retained more teeth as compared to females. This is attributed to malnutrition and hormonal disturbances occurring during the time of puberty, pregnancy and child births among females [13]. Comparable findings were reported by previous studies [10,12,14].
It was also evident from the present study that tooth retention was comparatively higher among the subjects with intermediate or post high school diploma than those who were illiterate and other low educational level study subjects which is in agreement with the other studies [10,11,15,16]. Higher education reflects increased awareness, utilization of oral health care services, favourable attitude towards oral health and importance given to preventive oral health care and hence, maintaining good oral health.
Further, study showed that unmarried subjects retained more teeth compared to married subjects. This finding was not in accordance with the results from investigations among other populations which did not show significant effect of marital status on tooth loss [17]. In contrast, other study conducted in past showed married retaining more teeth than unmarried subjects [10]. Finding of the present study can be attributed to the reason that most of the study subjects belonged to the unmarried age group (18-28 years), which amounted to 41.18% of total population.
Additionally, subjects who were using toothbrushes and tooth paste for cleaning their teeth retained more teeth when compared to other aids and materials. Similar observation was found in adults of Davangere taluk, India [5,10,18]. Higher tooth retention among tooth brush users may be due to superior plaque control among them, as the bristles of the tooth brush can reach the interproximal areas as well as pits and fissures of the teeth more efficiently than finger or other indigenous materials; thus, resulting in better oral hygiene.
Subjects practicing mixed diet retained more number of teeth as compared to those who were restricted to vegetarian diet. Analogous finding was observed in a previous study [10]. A well-balanced nutritious mixed diet, including adequate amount of proteins, vitamins, essential fatty acids and micronutrients, can play an important role in the resistance to infectious conditions, including periodontitis; which is required for maintenance of optimal general and oral health [19]; thus, enhancing tooth retention.
Further subjects who never visited the dentist in their lifetime showed greater tooth retention than subjects who visited dentist infrequently. Similar results were reported in Japanese aged 50-80 years [18]. But this finding was contradicted by study conducted among Brazilian adults which showed positive effect of routine visits for dental check-up on maintaining teeth [20]. This result of the study does not necessarily mean that regular dental visits are undesirable. It may be accredited to the fact that, subjects with oral health problems visit the dental clinics and subjects who never visited, might have not had any problem and hence, retained more number of teeth.
Limitation
The veracity on the information provided about income and alcohol habits are questionable. So these factors could have not shown any significant influence on tooth retention in the study. Further, reasons for visiting and not visiting the dentist were not included in the present study. The study employed random sampling. Hence, age and gender matching was not done, which has caused ambiguous and misleading results. This problem can be avoided in future studies by careful and good planning.
Conclusion
Males compared to females, lower age, professionals compared to illiterates, unmarried and mixed diet population, tooth brush and tooth paste users and population who never visited dentist showed more tooth retention. Thus, this study threw light on the factors affecting tooth retention in the population of Dharwad district, India. This information will help the health and social policy-makers to translate the knowledge on tooth retention into action programs for improving the oral health of the people.
Appendix