Femoral and Tibial Tunnel Widening following Anterior Cruciate Ligament Reconstruction using Various Modalities of Fixation: A Prospective Observational Study
Dileep Krishnamoorthy Srinivas1, Mahesha Kanthila2, Rama Prakasha Saya3, JVS Vidyasagar4
1 Assistant Professor, Deparatment of Orthopaedics, K.S.Hegde Medical Academy, Mangalore, Karnataka, India.
2 Consultant Orthopaedic Surgeon, Mangalore, Karnataka, India.
3 Associate Professor, Department of Medicine, JIPMER, Pondicherry, Pondicherry, India.
4 Consultant, Department of Orthopedic and Arthroscopy, Aware Global Hospitals, Hyderabad, Telangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dileep Krishnamoorthy Srinivas, Assistant Professor, Department of Orthopaedics, K.S. Hegde Medical Academy, Mangalore - 575018, Karnataka, India.
E-mail: dileepsri08@gmail.com
Introduction
Bone tunnel enlargement after Anterior Cruciate Ligament Reconstruction (ACL-R) is a well-accepted phenomenon but there are very few published data comparing the extent of tunnel widening by various methods of fixation after ACL-R.
Aim
To compare the femoral and tibial tunnel widening following ACL-R with different methods of fixation using CT scan.
Materials and Methods
This one year prospective study included all patients with chronic Anterior Cruciate Ligament (ACL) injury who underwent primary arthroscopic ACL-R using tripled hamstring tendon autograft. The graft was fixed to the tibial tunnel by Interference Screw (IFS) or Suture Disc (SD) and to the femoral tunnel by IFS, SD, Cross-Pin (CP) or Endo-button CL (Smith & Nephew). The widening of the tibial and femoral tunnels in different methods of fixation was assessed by Computed Tomography (CT) at 12 months follow-up; and was compared using paired sample test.
Results
A total of 63 patients were included in the study of which 58 (92%) were males and 5 (8%) were females, with a mean age of 29.1 ± 5.9 years. The tibial tunnel widening at one year follow-up was 1.680 ± 1.08794 (19.37%) and 1.517 ± 0.94834 mm (17.39%) by IFS and SD methods respectively. Femoral tunnel widening at one year follow-up was 1.294 ± 0.231, 1.809 ± 0.912, 1.320 ± 0.238, 1.779 ± 0.889 mm by IFS, SD, EB, and CP methods respectively. Femoral tunnel widening following suture disc method of fixation was very highly significant (p<0.001) in comparison with other methods.
Conclusion
Femoral tunnel and tibial tunnel widening varies with different methods of fixation and was maximum with suture disc method compared to others at one year follow-up after ACL-R.
Computed tomography, Femoral tunnel, Graft
Introduction
Reconstruction of torn Anterior Cruciate Ligament (ACL) is a standard procedure in orthopaedic practice. Different types of grafts and fixation methods are used for ACL reconstruction. Various post-operative complications have been described following this procedure. The enlargement of bone tunnels after Anterior Cruciate Ligament Reconstruction (ACL-R) is a well-known entity seen in different graft techniques and methods of fixation [1].
The knowledge about the origin and natural history of bone tunnel widening after ACL-R is scarce. It usually occurs during the first six months following surgery but may continue for two years post-operatively [2]. Although many studies have proven that this phenomenon does not affect the clinical outcome following ACL-R [3–8], few have demonstrated anterior knee laxity and graft failure due to tunnel widening [9,10]. Tunnel enlargement also is associated with a risk of staged revision surgery [11]. CT has been reported to be the best method for identifying tunnels and provides most accurate measurements. The fixation method used in the primary reconstruction can change the extent of tunnel widening [12]. There are very few published data comparing the extent of tunnel widening by various methods of fixation. Hence this study was conducted to compare the femoral and tibial tunnel widening following ACL-R with different methods of fixation using CT scan.
Materials and Methods
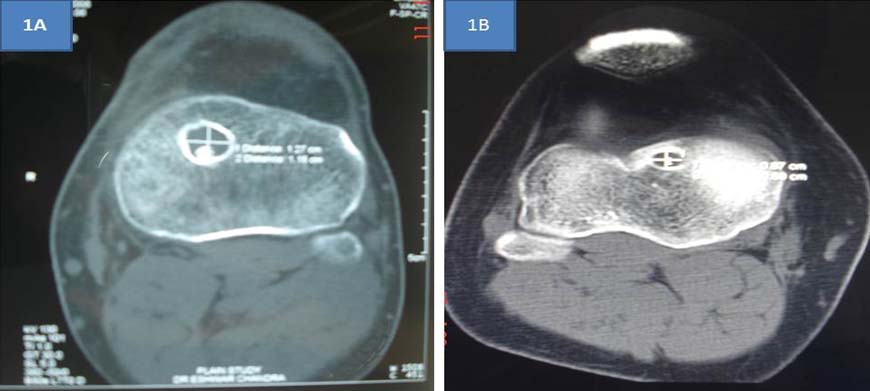
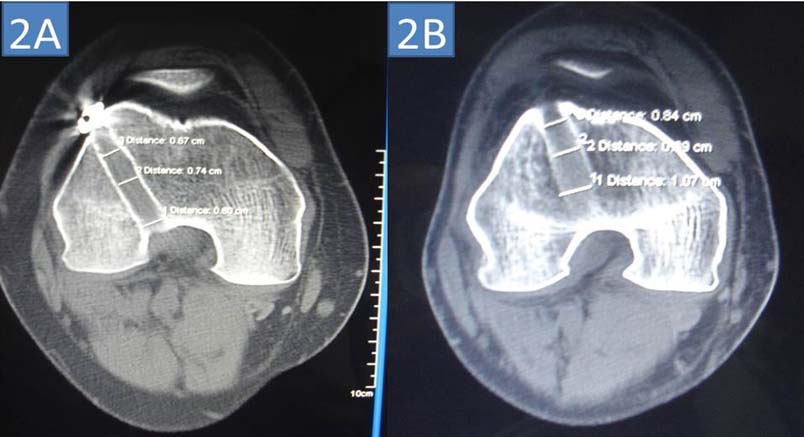
This was one-year prospective study conducted from January to December 2009 at a tertiary-care hospital in Southern India. Informed written consent was taken from all the patients. Institutional ethical clearance was obtained for this study. All patients with chronic ACL injury who underwent primary arthroscopic ACL-R using tripled hamstring tendon autograft were included in the study. Patients with associated medial or lateral collateral ligament injury or those undergoing revision ACL-R were excluded from the study. The graft was fixed to the tibial tunnel by Interference Screw (IFS) or Suture Disc (SD) and to the femoral tunnel by IFS, SD, Cross-Pin (CP) or Endo-button CL (Smith & Nephew). The reamed diameters of the tibial and femoral tunnels were noted. Post-operatively immediate accelerated physiotherapy protocol was followed in all patients to mobilize the knee joint. Closed chain exercises and isometric muscle strengthening exercises were started by 2nd post-operative day. Full weight-bearing walking was started from 2nd post-operative day. Patients were followed up at two weeks, six weeks, three months, six months and at one year. Patients were expected to achieve 90 range of motions at two weeks follow-up. Isokinetic and isotonic exercises were started at three months post-operatively and return to sports was allowed after six months. CT scan measurements of the femoral and tibial tunnels using Philips MX 8000 multislice CT scanner was done at one year follow-up [Table/Fig-1&2]. The slice thickness was 1 mm. Transosseous tibial tunnel diameter was measured at four levels; axial section at plateau and midpoint and sagittal section at plateau and midpoint. Femoral tunnel measurements were also done at four points; the axial section at notch, middle and the end of the tunnel and the coronoal image in the middle of the tunnel. The average of these tunnel diameters was tabulated. The widening of the tibial and femoral tunnels in different methods of fixation at 12 months follow-up was compared using paired sample test. The statistical analysis was done using SPSS version 17 software. A p-value of < 0.05 was considered significant.
CT scan measurement of tibial tunnel.
CT scan measurement of femoral tunnel.
Results
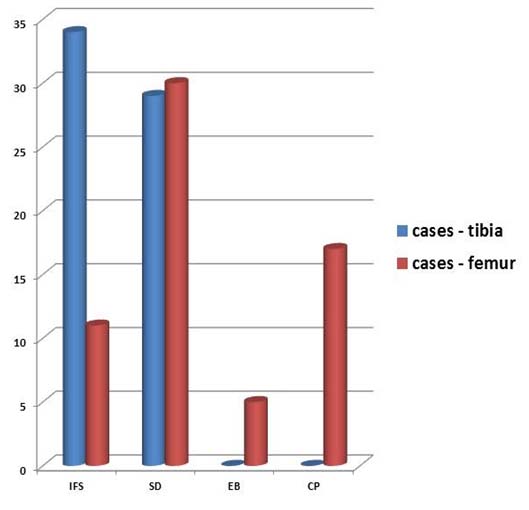
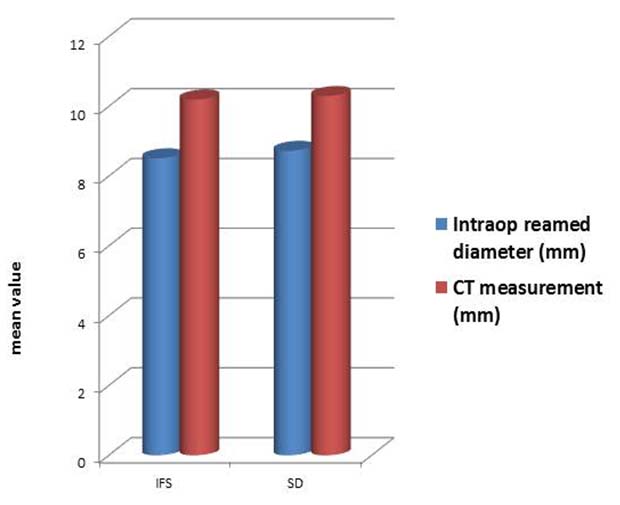
A total of 63 patients were included in the study of which 58 (92%) were males and 5 (8%) were females. The age group varied from 18 to 43 years with mean age of 29.1 ± 5.9 years. Of the 63 patients, fixation of graft to the tibial tunnel was performed with IFS in 34 patients (54%) and SD in 29 patients (46%). On the femoral side, fixation of graft was performed using IFS in 11 patients (17%), SD in 30 patients (47.6%), Endobutton CL in 5 patients (7.9%) and CP in 17 patients (27%) [Table/Fig-3]. Average follow-up period was 12 months in different methods of fixation. The tibial tunnel widening at one year follow-up was 1.680 ± 1.08794 (19.37%) and 1.517 ± 0.94834 mm (17.39%) by IFS and SD methods respectively [Table/Fig-4]. This was found to be statistically significant (p<0.05) [Table/Fig-5]. Femoral tunnel widening at one year follow-up was 1.294 ± 0.231, 1.809 ± 0.912, 1.320 ± 0.238, 1.779 ± 0.889 mm by IFS, SD, EB, and CP methods respectively [Table/Fig-6]. Tunnel widening was found to be statistically significant (p<0.05) by all the methods. However, widening following SD method of fixation was highly significant (p<0.001) in comparison with other methods [Table/Fig-7].
Tibial tunnel widening at one year.
Tibial tunnel widening comparison.
| Method | Intra-operative diameter (mm) | CT measurement at 1 year (mm) | Widening (mm) | p-value |
|---|
| IFS | 8.515±1.033 | 10.195±2.283 | 1.680 ± 1.08794 | 0.001 |
| SD | 8.724±1.005 | 10.295±1.491 | 1.517 ± 0.94834 | < 0.001 |
Femoral tunnel widening at one year.
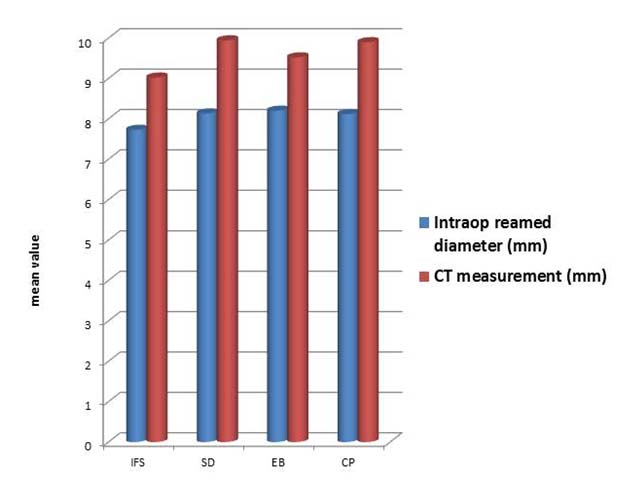
Femoral tunnel widening comparison.
| Method | Intra-operative diameter (mm) | CT measurement at 1 year (mm) | Widening (mm) | p-value |
|---|
| IFS | 7.727±1.506 | 9.021±2.059 | 1.294 ± 0.231 | 0.002 |
| SD | 8.133±0. .765 | 9.942±1.103 | 1.809 ± 0.912 | <0.001 |
| EB | 8.200±0.837 | 9.520±0. .473 | 1.320 ± 0.238 | 0.035 |
| CP | 8.118±0. .928 | 9.896±1.667 | 1.779 ± 0.889 | 0.003 |
Discussion
Despite its recognition, there is a paucity of knowledge about the origin and natural history of bone tunnel widening. The hamstring autograft used in ACL-R heals in three phases inside the tunnel by three major histological changes; the maturation of fibrous tissue, the new bone formation and the bone remodelling. The aetiology of tunnel widening is still not well understood. A complex interplay of biologic and mechanical factors probably contributes to tunnel widening. Biologic factors include immune-mediated increased cytokine levels or the inflammatory response caused by synovial fluid leakage within the bone tunnel. Mechanical factors include the types of graft, various methods of fixation and rehabilitation protocols [4].
CT is a standard method to measure the bone tunnel enlargement. Compared to X-ray, geometric factors like knee positioning differences or exposing distance from film surface do not influence the CT images. According to Hoher et al., suspensory graft fixation resulted in significantly greater longitudinal graft motion, known as the “bungee effect” while an aperture fixation correlates with transverse graft motion known as the “wind shield-wiper effect”. Transverse motion of the graft is directly proportional to the distance between the fixation points, with maximum transverse motion at the tunnel aperture. Suspensory methods of fixation are associated with increased tunnel widening by causing more graft micro-motion than aperture fixation [13].
Peyrache et al., noted an increase in tunnel diameter at 3 months post-operatively and no changes between 3 months and 2 years and decreases after 3 years post-operatively [4]. Hence, we decided to observe tunnel widening at 12 months follow-up with CT scan measurements compared with reamed diameter. In our study, we observed femoral and tibial tunnel widening in all methods of fixation which correlates with other studies [14,15]. The tibial tunnel measurements increased by 19.73% and 17.39% in IFS and SD method respectively, both of which were statistically significant. The femoral tunnel measurements increased by 16.75% in IFS, 22.24% in SD, 16.1% in EB, and 21.91% in cross pin fixation methods. Tunnel widening was significant in all methods of fixation. The femoral tunnel widening was more in cross pin fixation method compared to Endobutton CL group. This is comparable to another study which concluded that transfixation pin system fixation caused greater femoral tunnel enlargement compared to extra-cortical fixation methods [16]. Tunnel widening following SD method of fixation was statistically very highly significant compared to other methods of fixation.
Conclusion
Femoral tunnel and tibial tunnel widening varies with different methods of fixation and was maximum with suture disc method compared to others at one year follow-up after ACL-R.
[1]. Iorio R, Di Sanzo V, Vadala A, Conteduca J, Mazza D, Redler A, ACL reconstruction with hamstrings: how different technique and fixation devices influence bone tunnel enlargementEur Rev Med Pharmacol Sci 2013 17:2956-61. [Google Scholar]
[2]. Marchant MH, Willimon SC, Vinson E, Pietrobon R, Garrett WE, Higgins LD, Comparison of plain radiography, computed tomography and magnetic resonance imaging in the evaluation of bone tunnel widening after anterior cruciate ligament reconstructionKnee Surg Sports Traumatol Arthrosc 2010 18:1059-64. [Google Scholar]
[3]. Kawaguchi Y, Kondo E, Kitamura N, Kai S, Inoue M, Yasuda K, Comparisons of femoral tunnel enlargement in 169 patients between single-bundle and anatomic double bundle anterior cruciate ligament reconstructions with hamstring tendon graftsKnee Surg Sports Traumatol Arthrosc 2011 19:1249-57. [Google Scholar]
[4]. Peyrache MD, Dilan P, Christel P, Witvoet J, Tibial tunnel enlargement after anterior cruciate ligament reconstruction by autogenous bone-patellar tendon-bone graftKnee Surg Sports Traumatol Arthorsc 1996 4:2-8. [Google Scholar]
[5]. Webster KE, Feller JA, Hameister KA, Bone tunnel enlargement following anterior cruciate ligament reconstruction: a randomised comparison of hamstring and patellar tendon grafts with 2 year follow-upKnee Surg Sports Traumatol Arthrosc 2001 9:86-91. [Google Scholar]
[6]. Buelow JU, Siebold R, Ellermann A, A prospective evaluation of tunnel enlargement in anterior cruciate ligament reconstruction with hamstrings: extracortical versus anatomical fixationKnee Surg Sports Traumatol Arthrosc 2002 10:80-85. [Google Scholar]
[7]. Ito MM, Tanaka S, Evaluation of tibial bone-tunnel changes with X-ray and computed tomography after ACL reconstruction using a bone-patella-bone autograftInt Orthop 2006 30:99-103. [Google Scholar]
[8]. Fink C, Zapp M, Benedetto KP, Hackl W, Hoser C, Rieger M, Tibial tunnel enlargement following anterior cruciate ligament reconstruction with patellar tendon Journal of Clinical and Diagnostic Research 9 autograftArthroscopy 2001 17:138-43. [Google Scholar]
[9]. Siebold R, Kiss ZS, Morris HG, Effect of compaction drilling during ACL reconstruction with hamstrings on post-operative tunnel wideningArch Orthop Trauma Surg 2008 128:461-68. [Google Scholar]
[10]. Webster KE, Chiu JJ, Feller JA, Impact of measurement error in the analysis of bone tunnel enlargement after anterior cruciate ligament reconstructionAm J Sports Med 2005 33:1680-87. [Google Scholar]
[11]. Getelman MG, Friedman MJ, Revision anterior cruciate ligament reconstruction surgeryJ Am Scad Orthop Surg 1999 7:189-98. [Google Scholar]
[12]. Fauno P, Kaalund S, Tunnel widening after hamstring anterior cruciate ligament reconstruction is influenced by the type of graft used: a prospective randomised studyArthroscopy 2005 21:1337-41. [Google Scholar]
[13]. Hoher J, Livesay GA, Ma CB, Withrow JD, Fu FH, Woo SL, Hamstring graft motion in the femoral bone tunnel when using titanium button/polyester tape fixationKnee Surg Sports Traumatol Arthrosc 1999 7:215-19. [Google Scholar]
[14]. Iorio R, Vadalà A, Argento G, Di Sanzo V, Ferretti A, Bone tunnel enlargement after ACL reconstruction using autologous hamstring tendons: a CT studyInt Orthop 2007 31:49-55. [Google Scholar]
[15]. Weber AE, Delos D, Oltean HN, Vadasdi K, Cavanaugh J, Potter HG, Tibial and femoral tunnel changes after acl reconstruction: A prospective 2-year longitudinal MRI studyAm J Sports Med 2015 43:1147-56. [Google Scholar]
[16]. Lopes OV Jr, de Freitas Spinelli L, Leite LH, Buzzeto BQ, Saggin PR, Kuhn A, Femoral tunnel enlargement after anterior cruciate ligament reconstruction using RigidFix compared with extracortical fixationKnee Surg Sports Traumatol Arthrosc 2015 Nov 27 [Epub ahead of print] [Google Scholar]