Multiple Cerebrovascular Complications due to Sphenoid Sinusitis
Raghu Teja Sadineni1, Sandeep Velicheti2, Chandra Sekhar Kondragunta3, Narayan Chander Bellap4
1 Seniour Resident, Department of Radiology, Dr Pinnamaneni Siddhartha Institute of Medical Sciences & Research Foundation, Vijayawada, Andhra Pradesh, India.
2 Assistant Professor, Department of Radiology, Dr Pinnamaneni Siddhartha Institute of Medical Sciences & Research Foundation, Vijayawada, Andhra Pradesh, India.
3 Professor, Department of Radiology, Dr Pinnamaneni Siddhartha Institute of Medical Sciences & Research Foundation, Vijayawada, Andhra Pradesh, India.
4 Professor & HOD, Department of Radiology, Dr Pinnamaneni Siddhartha Institute of Medical Sciences & Research Foundation, Vijayawada, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Raghu Teja Sadineni, Flat 503, Aruna Residency, Netaji Street, Vijayawada-520010, Andhra Pradesh, India.
E-mail: sadineniraghu@gmail.com
Sphenoiditis is of particular interest because the sphenoid sinus has thin wall and its special anatomical location facilitate dissemination of infection to many intracranial structures including vascular structures. The main objective of this report is to gain insight into patterns of presentation and imaging findings in cerebrovascular complications of sphenoid sinusitis and to emphasize the need of reviewing Brain Computed Tomography Scan in all windows. This is a report of 32-year-old young female presented with fever and headache who was diagnosed to have sphenoid sinusitis after radiological examination.
Sphenoid sinusitis may involve several intracranial structures, with potentially severe or even fatal complications. Prompt diagnosis and antibiotic/antifungal therapy is essential to minimize mortality and morbidity.
Base of skull osteomyelitis, Cavernous sinus thrombosis, Meningitis, MR angiography
Case Report
A 32-year-old young female presented with history of fever and headache since 15 days, left hemiparesis along with blurred vision, diplopia and left ophthalmoplegia since 5 days. She was on treatment with antipyretics and analgesics for the first few days with a provisional diagnosis of viral fever and was then referred from a peripheral nursing home to tertiary hospital after she started developing eye symptoms and weakness. She had routine blood analysis which did not disclose any particular aetiology other than raised Erythrocyte Sedimentation Rate (ESR). Neurological assessment revealed features of left hemiparesis and ophthalmoplegia. A diagnosis of meningitis, venous sinus thrombosis or cerebrovascular ischemia was suspected and the patient was sent for imaging.
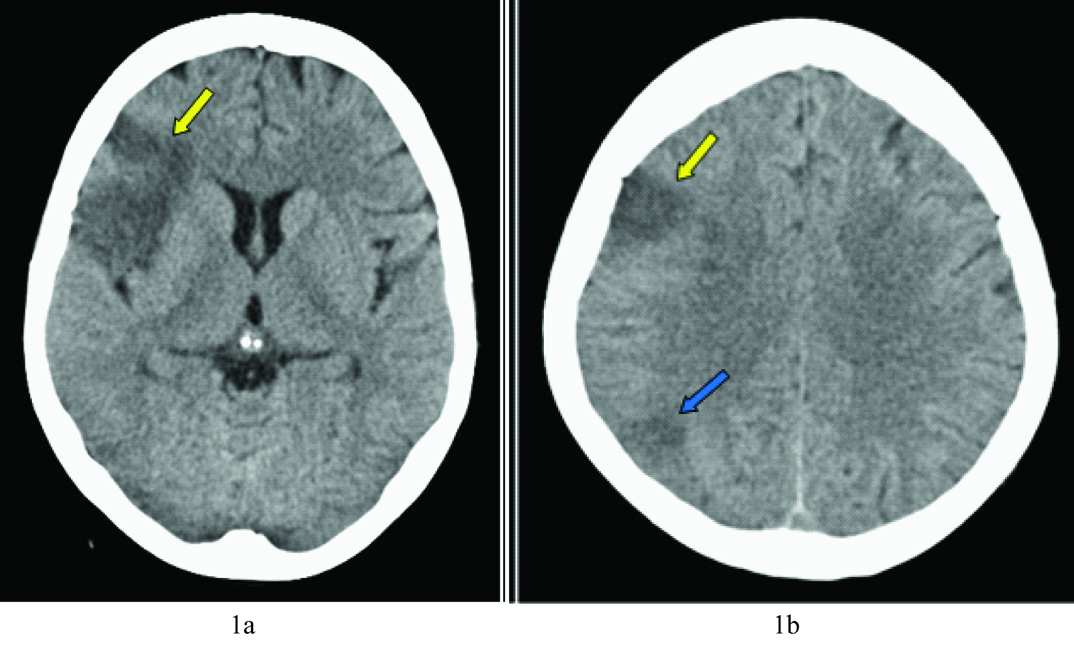
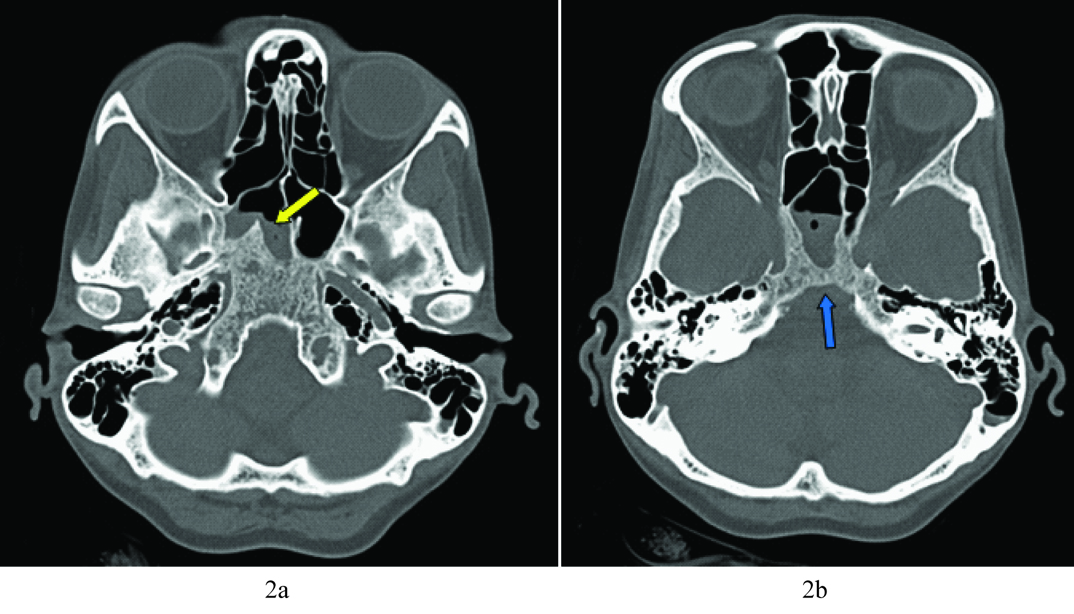
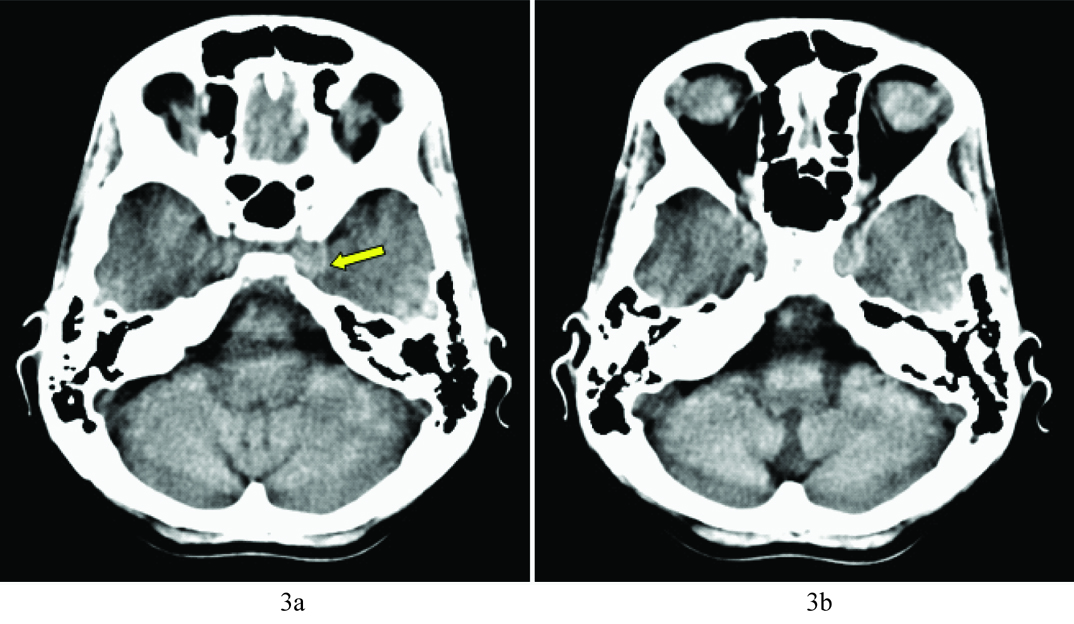
Plain Computed Tomography (CT) Brain was advised which showed Right Middle Cerebral Artery (MCA) territory infarct anteriorly and junctional zone between middle cerebral artery and posterior cerebral artery territories posteriorly [Table/Fig-1a,b]. Bone/sinus window revealed fluid collection with extensive mucosal thickening in right sphenoid sinus, bony erosions in the wall and diffuse osteopenia and permeative pattern of bone destruction in mid base of skull suggestive of underlying osteomyelitis [Table/Fig-2a,b]. Hyper density was seen in left cavernous sinus region possibly indicating thrombosis [Table/Fig-3a,b].
Axial non contrast CT images show hypodensities involving variably the right MCA territory anteriorly (yellow arrow) and junctional zone posteriorly (blue arrow) suggestive of infarction.
(a) Evaluation in bone window demonstrated extensive mucosal thickening in sphenoid sinus on right side (yellow arrow) with fluid collection. Bony erosion (blue arrow) was seen in walls of sphenoid sinus; (b) Basisphenoid, Clivus & Basiocciput showed diffuse Osteopenia and permeative pattern of bone destruction suggestive of underlying Osteomyelitis.
Careful scrutiny of base of skull revealed hyper density and mild bulging in region of left cavernous sinus (yellow arrow) - indicating thrombus or an aneurysm.
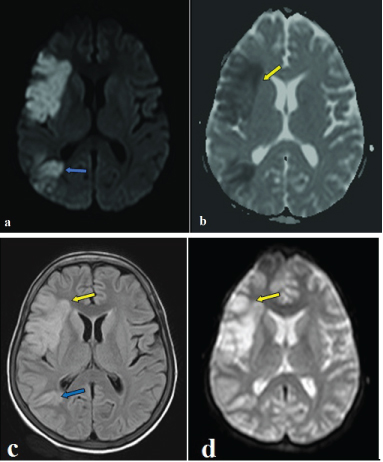
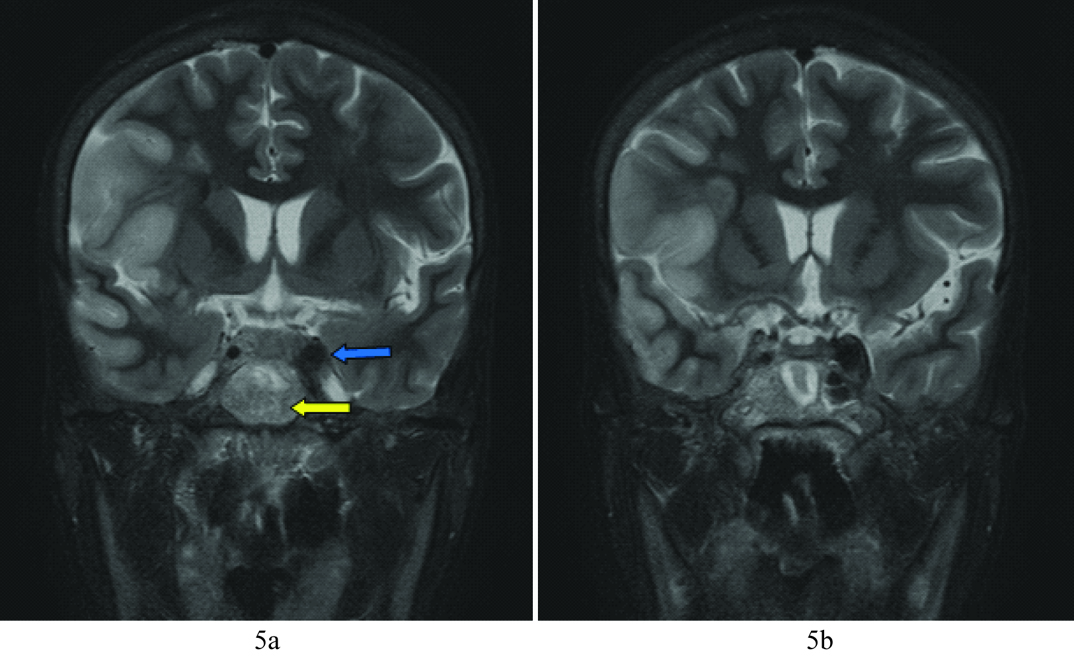
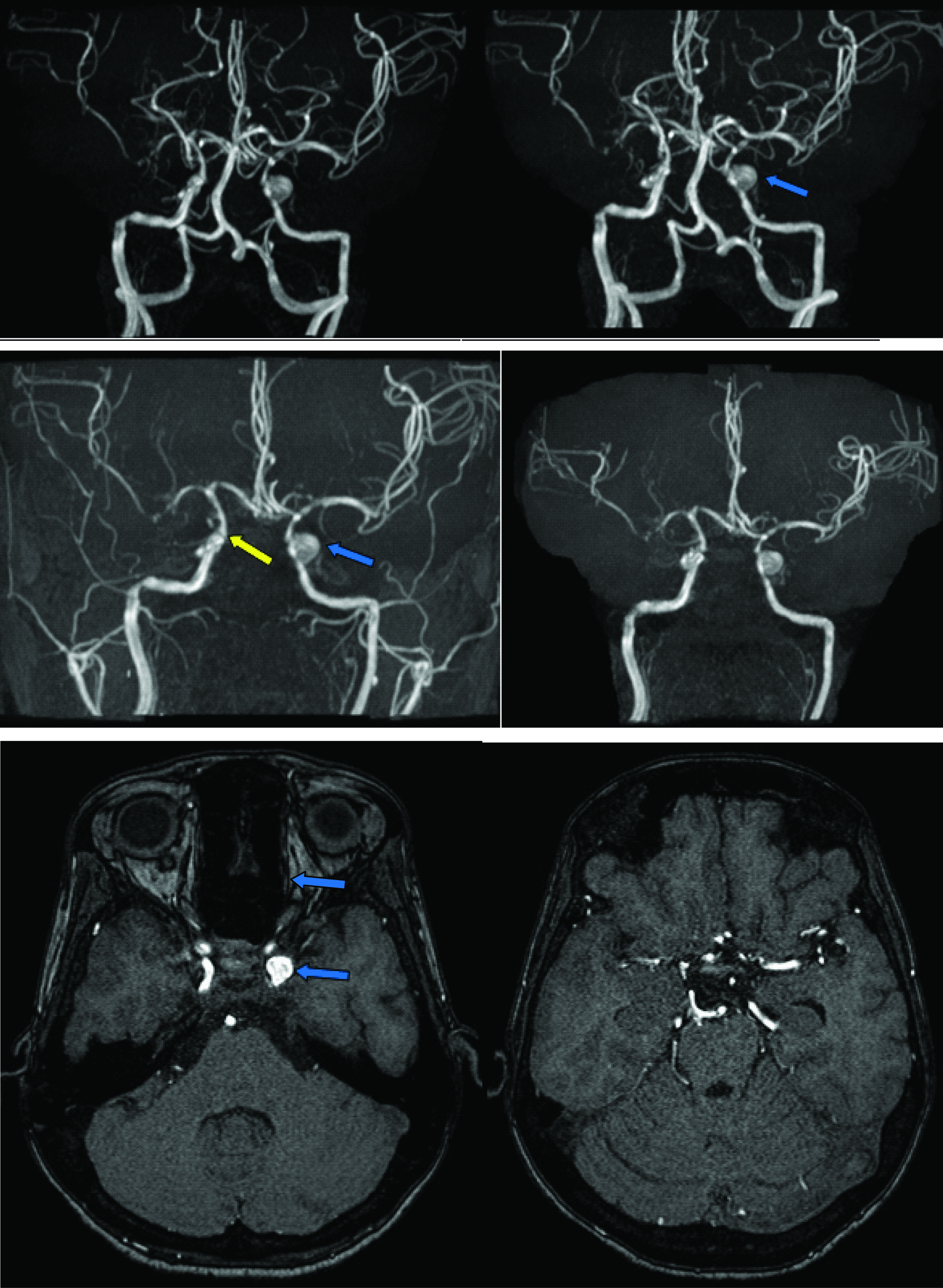
MRI brain and MR Angiography with contrast was advised for further assessment of the inconclusive CT findings which confirmed acute right MCA infarct [Table/Fig-4a-d] secondary to infective vasculitis and showed stenosis at petro cavernous part of right Internal Carotid Artery (ICA), left ICA showed similar stenosis with mycotic type of aneurysm at cavernous region [Table/Fig-5a,b,6a-f]. Left cavernous sinus & transverse sinus thrombosis was also demonstrated [Table/Fig-7a-f].
Findings: DWI & ADC images show restriction of diffusion, T2 FLAIR images show hyperintensity in right Middle Cerebral Artery (MCA) territory anterior part (yellow arrow) & at junctional zone posteriorly (blue arrow).
FAT SAT T2 coronal images demonstrate diffuse hyperintensity of clivus (yellow arrow) and enlarged carotid flow void in the left cavernous sinus (blue arrow).
(a,b) MRA showed poor visualization of Right MCA due to thromboembolism and vasculitis related stenosis at petro-cavernous part of distal ICA on both sides. Mycotic type of aneurysm (blue arrow) seen in cavernous portion of left ICA. However, normal flow seen in the left MCA. (c,d). Images displayed after subtraction of posterior circulation and smaller cortical branches further delineates distal ICA stenosis (yellow arrow) and aneurysm (blue arrow). (e,f). Source images displaying the aneurysm in left ICA (blue arrow) and stenosis in right MCA (yellow arrow).
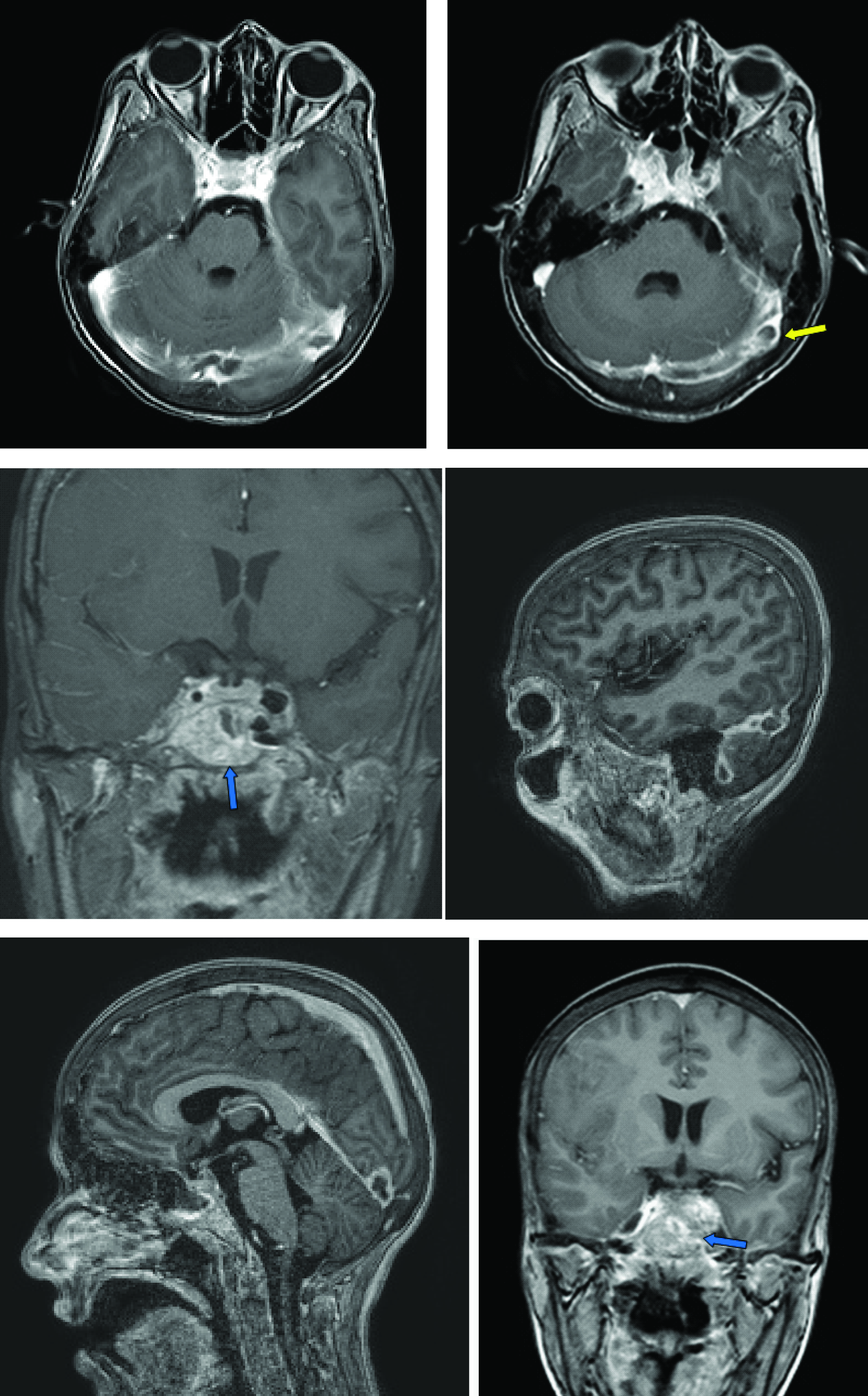
Post contrast study shows filling defect in left transverse sinus (yellow arrow) and small filling defect in the left cavernous sinus – suggestive of thrombosis. Aneurysm of left internal carotid artery, early features of meningitis surrounding right MCA and intense enhancement of clivus and walls of sphenoid sinus (blue arrow) noted.
Sphenoid sinusitis with mid Base of Skull (BOS) osteomyelitis involving sphenoid bone, clivus and occipital condyles, acute right MCA infarct secondary to infective vasculitis, stenosis at petro cavernous part of right ICA and stenosis due to vasculitis with mycotic type of aneurysm from Left ICA at cavernous region, left cavernous sinus & transverse sinus thrombosis & early features of Meningitis were given as the radiological diagnosis based on the imaging features. All the above mentioned features appear secondary to infection extending from acute or chronic sphenoid sinusitis.
The patient was managed conservatively with high doses of broad spectrum antibiotics and anti fungals (I.V. and oral). Anti thrombotics and antiplatelets were started. Though she was explained about the clinical scenario and the complications, she did not opt for sinus drainage and endovascular interventional management due to socio-economic constraints. She was stabilized and discharged with mild residual limb weakness and did not turn up for follow up.
Discussion
Infectious aneurysms are believed to represent only 2% to 5% of all intracranial aneurysms [1]. Intracranial aneurysms may also result from fungal infection, causing true “mycotic”, or fungal aneurysms, although the causative agent is usually bacterial [2].
Intracranial and intravascular complications of sphenoid sinusitis are very uncommon constituting less than 1% of cases, but have high morbidity. These include International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM) classification: subdural abscess, extradural abscess, brain abscess, meningitis, cavernous sinus or other intracranial venous sinus thrombophlebitis or osteomyelitis. Subdural empyema is the most frequently reported complication (33% {22%-45%}), followed by brain abscess (27% {19%-35%}) and meningitis (20% {15%-26%}). The complete recovery can be expected in majority of the cases (71% {61%-81%}), fatalities can occur in (6% {3-9%}) of cases of intracranial complication with bacterial rhino sinusitis [3].
Clinical features of sphenoid sinusitis and its complications remains a challenge. Many cases of sphenoiditis fail to present with rhinologic signs. Headache in these cases is the only symptom, and clinical diagnosis is challenging [3]. The clinical manifestations are variable and non-specific. Presenting symptoms may include headache or facial pain (88%), rhinorrhea (46%), and nasal congestion (26%) [4].
Imaging studies in sinusitis may be relatively non-specific with respect to the causative agent in the early stages of infection. Early findings include mucosal thickening involving the nasal cavity, as well as the maxillary or ethmoid sinuses. The sphenoid sinus is less frequently affected. CT imaging demonstrates bony changes or dehiscence’s (42%), a mass (24%), or complete opacification of the sphenoid sinus (22%) [4]. In a fungal aetiology, CT may demonstrate bony changes including sclerotic thickening, erosion, or remodeling, which are rare in acute bacterial infections.
Management of CNS fungal infections is often a complex problem in neurologic therapeutics. First line sinus treatment was basic drainage (trephination or sphenoidotomy) which proved to be effective, and not extended endoscopic sinus surgery which might expose patients to bleeding, synechia or complications, which may in turn warrant another procedure [3,5]. Intravenous amphotericin treatment following debridement is usually considered appropriate therapy in invasive fungal sinusitis [2]. Early diagnosis is of utmost importance as medical treatment has a favorable prognosis and no surgical intervention is required [6].
The uniformly poor outcomes reported following cerebrovascular invasion by fungus might indicate that the development of a fungal aneurysm is a clinical marker requiring more aggressive therapy than simple intravenous treatment, perhaps including intrathecal medication or hyperbaric therapy [2]. Testing for underlying immunocompromised states is warranted in patients with cerebral mycotic aneurysms [7].
Conclusion
Sphenoid sinusitis may thus involve many intracranial structures, with potentially severe or even fatal complications and hence a careful scrutiny for the related complications needs to be undertaken. Clinical findings may not be very conclusive for the diagnosis of sphenoid sinusitis reiterating the importance of early imaging and timely management to prevent such adverse complications. Particularly, fungal aetiology needs to be considered when the response to antibiotics alone is poor where imaging studies play a crucial role for etiological diagnosis.
[1]. Frazee J, In: Wilkins R, Rengachary S, eds. Inflammatory aneurysmsNeurosurgery 1996 New YorkMcGraw Hill:2378-2382. [Google Scholar]
[2]. Hurst RW, Judkins A, Bolger W, Chu A, Loevner LA, Mycotic Aneurysm and Cerebral Infarction Resulting from Fungal Sinusitis: Imaging and Pathologic CorrelationAm J Neuroradiol 2001 22(5):858-63. [Google Scholar]
[3]. Bayonne E, Kania R, Tran P, Huy B, Herman P, Intracranial complications of rhinosinusitis. A review, typical imaging data and algorithm of managementRhinology 2009 47:59-65. [Google Scholar]
[4]. Friedman A, Batra PS, Fakhri S, Citardi MJ, Lanza DC, Isolated sphenoid sinus disease: aetiology and managementOtolaryngol Head Neck Surg 2005 133(4):544-50. [Google Scholar]
[5]. Fenton JE, Smyth DA, Viani LG, Walsh MA, Sinogenic brain abscessAm J Rhinol 1999 4:299-302. [Google Scholar]
[6]. Lee SJ, Weon YC, Cha HJ, Kim SY, Seo KW, Jegal Y, A Case of Atypical Skull Base Osteomyelitis with Septic Pulmonary EmbolismJ Korean Med Sci 2011 26(7):962-65. [Google Scholar]
[7]. Allena LM, Fowlerb AM, Walkerc C, Derdeynb CP, Nguyena BV, Hassoa AN, Retrospective Review of Cerebral Mycotic Aneurysms in 26 Patients: Focus on Treatment in Strongly Immunocompromised Patients with a Brief Literature ReviewAJNR 2013 34:823-27. [Google Scholar]