Blunt Cardiac Rupture: A Diagnostic Challenge
Suraj Pinni1, Vineet Kumar2, Satish Balkrishna Dharap3
1 Post Graduate Resident, Department of General Surgery, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai, Maharashtra, India.
2 Assistant Professor, Department of General Surgery, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai, Maharashtra, India.
3 Professor, Department of General Surgery, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Suraj Pinni, Post Graduate Resident, Department of General Surgery, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai-400022, Maharashtra, India.
E-mail: surajpinni@gmail.com
Blunt Cardiac Rupture (BCR) is a life threatening injury. Majority of patients do not reach the hospital and in those who reach the emergency department, timely diagnosis and treatment is a challenge. The case is about a patient with multiple blunt injuries who presented in shock. Cardiac tamponade was suspected on clinical grounds and on evidence of mediastinal widening on radiograph. In the absence of songography, the diagnosis was confirmed by subxiphoid pericardial window. Emergency thoracotomy revealed a right atrial appendage rupture which was surgically corrected. The patient also underwent splenectomy for grade IV splenic injury. Liver injury, pubic diastasis and tibial spine avulsion fracture was managed conservatively. He recovered well. Systematic observance of trauma resuscitation guidelines can help salvage patients with life threatening complex injuries even in the absence of specialized imaging investigations.
Cardiac tamponade, Focussed assessment with sonography in trauma, Polytrauma, Right atrial appendage
Case Report
A 22-year-old unidentified male was brought to the emergency room with history of road traffic crash, with no witnesses to the accident. At presentation, patient was agitated, drowsy and diaphoretic with tachycardia of 130/min and Blood Pressure (BP) of 78mmHg systolic. There was bilaterally equal air entry, mild abdominal tenderness and blood tinged urine on inserting Foley catheter.
On fluid resuscitation, BP transiently rose and patient became responsive and obeyed commands. BP showed downward trend to 70 mmHg systolic over next ten minutes and Central Venous Pressure (CVP) was found to be 20cm of H2O. Heart sounds were muffled on auscultation. Chest radiograph was suggestive of a widened mediastinum [Table/Fig-1]. Pelvic radiograph was suspicious of pubic diastasis suggestive of open book pelvic fracture. The hospital ultrasound machine was out of order and patient was unstable to be shifted to radiology suite for Focused Assessment by Sonography in Trauma (FAST) or Trans Thoracic Echocardiography (TTE).
Portable radiograph depicting widened mediastinum.

A primary diagnosis of cardiac tamponade was considered and urgent cardiac surgery consultation was sought. The patient was intubated in view of progressive hypotension. On reassessment, air entry was reduced bilaterally, hence, bilateral intercostal drains were inserted and pneumothorax was drained bilaterally. Subsequently, air entry improved bilaterally. CVP persisted to be 20cm of H2O and patient continued to be hypotensive. Blind pericardiocentesis was attempted unsuccessfully. Patient was shifted into the operation theatre and subxiphoid pericardial window revealed a bulging pericardium. Diagnostic Peritoneal Lavage (DPL) was also done which showed haemoperitoneum. Median sternotomy was done and 250ml of clots and blood was evacuated on opening pericardium, following which BP showed an upward trend. A 0.5 cm actively bleeding rent was identified on right atrial appendage [Table/Fig-2]. The rent was closed with 5-0 polypropylene suture in two layers. Laparotomy was done and 600ml haemoperitoneum was evacuated. Splenectomy was done for grade four laceration. Large non-expanding pelvic and retroperitoneal hematoma and a small non-bleeding liver laceration were left untouched. Patient was transfused four units of blood and fresh frozen plasma each. Patient made an uneventful recovery. A postoperative TTE showed no abnormality. Patient also had a tibial spine avulsion fracture which was managed conservatively. The Revised Trauma Score (RTS) which is a physiological score which takes into consideration Glasgow Coma Scale (GCS), respiratory rate and systolic blood pressure was calculated to be 6.171 in this patient (range 0 - 7.8408; Lower score indicates more severe injury; higher scores have better survival). Injury Severity Score (ISS) is an anatomical trauma score and is the sum of squares of abbreviated injury scores of the three worst anatomical injuries; was 45 (52 + 42 + 22) in this patient (ranges from 0 to 75, score ≥16 is considered a severe injury).
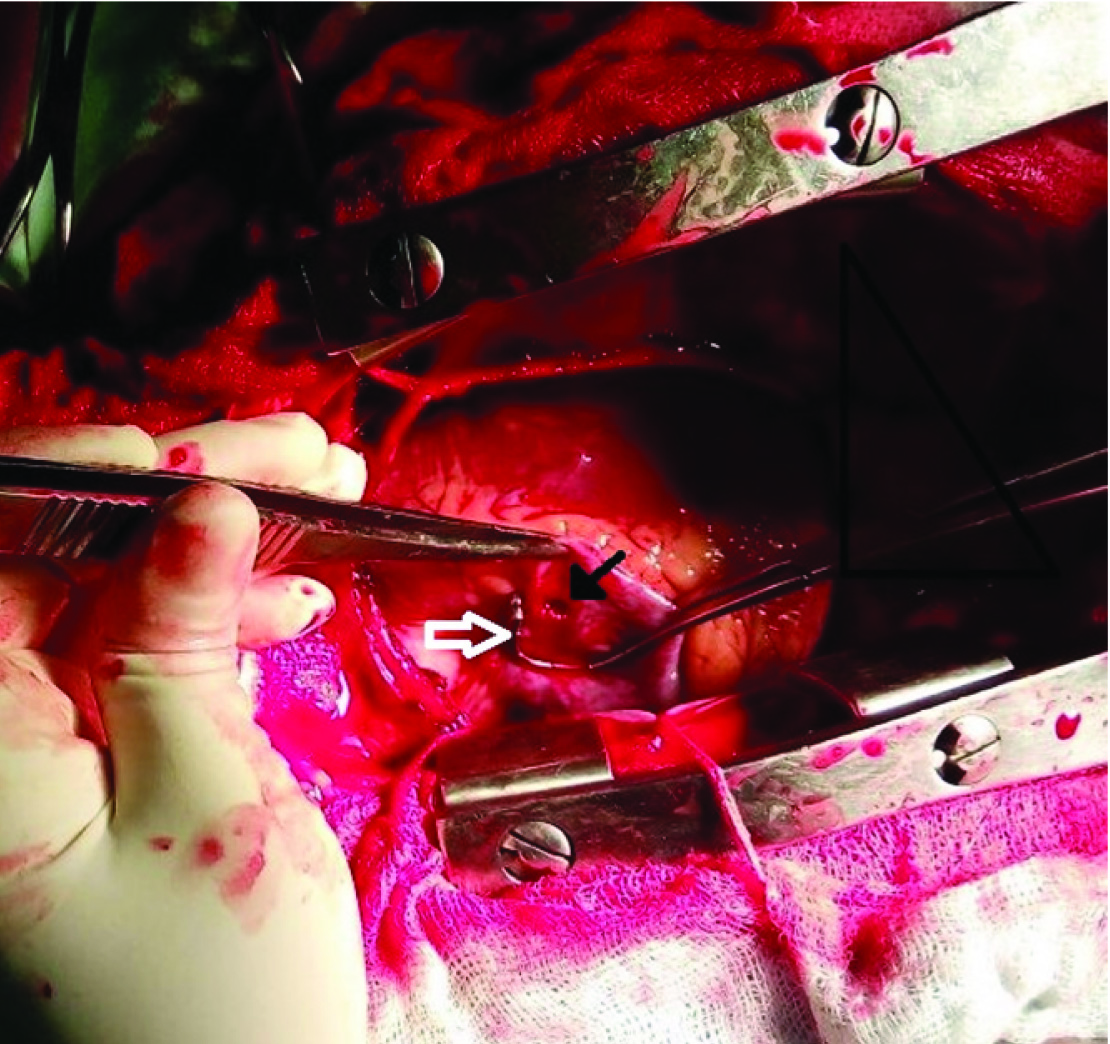
Intaoperative photo showing rent in right atrial appendage; Black arrow-Right atrial appendage rent, White arrow- Satinsky clamp providing temporary haemostasis.
Discussion
Blunt Cardiac Injuries (BCI), which in addition to BCR also include injuries such as myocardial contusion, have been reported in 8 to 86% of cases of blunt chest trauma and are associated with high mortality rates [1]. According to Kulshreshtha P et al., 2.2% of BCI reached the hospital alive as compared to 17.4% of penetrating cardiac injuries and unlike penetrating cardiac injuries in which the wound of entry is suggestive, blunt cardiac injuries often go unsuspected [2]. Though it has been more than six decades since the first reported successful treatment of BCR in 1955 [3], little progress has been made in defining nomenclature and treatment guidelines for the same. Motor vehicle accidents are the most common mode of blunt cardiac injuries [1,4,5]. BCR is associated with mortality rates ranging from 50 to 100 percent [4,6,7]. A number of mechanisms have been hypothesised for BCR which include deceleration injury, compression of heart between the sternum and vertebral column, rib fractures or transmission of venous pressure due to compression of abdomen or lower extremities [1,5,8,9]. The site of rupture depends on the phase of cardiac cycle where the blunt trauma occurred [8,9]. As there was no external sign of blunt chest trauma, in this case the likely mechanisms are transmitted venous pressure from blunt abdominal compression injury and deceleration injury.
Cardiac rupture commonly presents with signs of cardiac tamponade i.e., a clinical triad of hypotension, muffled heart sounds and distended neck veins except when there is a concomitant pericardial rent, in which case presentation is of massive haemothorax. Associated exsanguinating injuries are known to mask the signs of tamponade. Electrocardiogram and cardiac enzymes are believed to have a role in ruling out cardiac injuries rather than confirming them in the acute setting [10–13]. Although many reports describe radiographic findings of widened mediastinum and enlarged cardiac silhouette, radiography was found to be normal in many of the documented cases of tamponade in a National Trauma Data Bank (NTDB) study [1]. Almost all latest reviewed case reports and articles have reiterated the importance of FAST, TTE and Computed Tomography (CT) in setting of suspected BCR which were not possible in this case [10,14]. Ultrasound guided pericardiocentesis shows its utility in being both diagnostic as well as a temporary therapeutic measure. According to Hirai S et al., the color of blood aspirated on paracentesis gives a clue regarding the site of cardiac rupture [7]. Figuieredo AM et al., were able to diagnose tamponade in the absence of Ultrasonography (USG), on clinical suspicion, radiography and subxiphoid pericardial window as was done in this case [8]. Subxiphoid pericardial window followed by median sternotomy is the preferred incision. Median sternotomy offers a good exposure to all chambers of the heart as well as to the great vessels, provides an easy access for cardio pulmonary bypass and can be easily extended into a laparotomy if the need arose [7]. According to Braithwaite CE et al., the commonest site of cardiac rupture is right atrium (40.6%), followed by right ventricle (31%), left atrium (25%) and left ventricle (12%) [13]. Autopsy studies have proved that right atrial appendage is thinner then right atrial wall and hence theoretically is more susceptible to rupture which is opposite to the observations in previous studies showing right atrial wall rupture to be more common than right atrial appendage rupture [9]. Pledgeted or non pledgeted polypropylene suture repair has been preferred [6,8–10] in comparison to silk suture repair [15]. Postoperatively evaluation for occult septal defects or valvular injuries has been recommended [5]. Almost all authors have advised early diagnosis and management of tamponade based on use of portable ultrasound (FAST) and/or 2D-echocardiography which is very logical when these modalities are available in the trauma resuscitation area [14]. This case illustrates how cardiac tamponade may be managed successfully in a resource poor environment by following advanced trauma guidelines.
Conclusion
Diagnosis of cardiac rupture requires a very high index of clinical suspicion. A systematic approach to trauma patient assessment using advanced trauma guidelines can help reach the diagnosis and therefore management of cardiac tamponade following BCR.
[1]. Teixeira PGR, Inaba K, Oncel D, DuBose J, Chan L, Rhee P, Blunt Cardiac Rupture: A 5-Year NTDB AnalysisJ Trauma Injury Infect Crit Care 2009 67:788-91. [Google Scholar]
[2]. Kulshrestha P, Das B, Iyer KS, Sampath KA, Sharma ML, Rao IM, Cardiac Injuries-A Clinical and Autopsy ProfileJ Trauma 1990 30:203-07. [Google Scholar]
[3]. Desforges G, Ridder WP, Lenoci RJ, Successful suture of ruptured myocardium after nonpenetrating injuryN Engl J Med 1955 252:567-69. [Google Scholar]
[4]. Fulda G, Brathwaite CE, Rodriguez A, Turney SZ, Dunham CM, Cowley RA, Blunt traumatic rupture of the heart and pericardium: A ten-year experience (1979–1989)J Trauma 1991 31:167-73. [Google Scholar]
[5]. Chaer RA, Doherty JC, Merlotti G, Salzman SL, Fishman D, A case of blunt injury to the superior vena cava and right atrial appendage: Mechanisms of injury and review of the literatureInjury extra 2005 36:341-45. [Google Scholar]
[6]. May AK, Patterson MA, Rue LW III, Schiller HJ, Rotondo MF, Schwab CW, Combined blunt cardiac and pericardial rupture: Review of the literature and report of a new diagnostic algorithmAm Surg 1999 65:568-74. [Google Scholar]
[7]. Hirai S, Hamanaka Y, Mitsui N, Isaka M, Kobayashi T, Successful emergency repair of blunt right atrial rupture after a traffic accidentAnn Thorac Cardiovasc Surg 2002 8:228-30. [Google Scholar]
[8]. Figueiredo AM, Poggetti RS, Quintavalle FG, Fontes B, Dalva M, Younes RN, Isolated right atrial appendage (RAA) rupture in blunt trauma – a case report and an anatomic study comparing RAA and right atrium (RA) wall thicknessWorld J Emerg Surg 2007 2:5 [Google Scholar]
[9]. Jose ETT, Javier EAA, Michael JR, Surgical repair of right atrial wall rupture after blunt chest traumaTex Heart Inst J 2012 39:579-81. [Google Scholar]
[10]. Sybrandy KC, Cramer MJ, Burgersdijk C, Diagnosing cardiac contusion: old wisdom and new insightsHeart 2003 89:485-89. [Google Scholar]
[11]. Parr MJ, Blunt cardiac injuryMinerva Anestesiol 2004 70:201-05. [Google Scholar]
[12]. Jackson L, Stewart A, Best evidence topic report. Use of troponin for the diagnosis of myocardial contusion after blunt chest traumaEmerg Med J 2005 22:193-95. [Google Scholar]
[13]. Brathwaite CE, Rodriguez A, Turney SZ, Dunham CM, Cowley RA, Blunt Traumatic Cardiac Rupture A 5-Year ExperienceAnn Surg 1990 212:701-04. [Google Scholar]
[14]. Symbas NP, Bongiorno PF, Symbas PN, Blunt Cardiac Rupture: The utility of emergency department ultrasoundAnn Thorac Surg 1999 67:1274-76. [Google Scholar]
[15]. Salooja MS, Singla M, Srivastava A, Mukherjee KC, Isolated tear in left atrial appendage due to blunt trauma chest: A rare case reportJ Saudi Heart Assoc 2013 25:95-97. [Google Scholar]