Periodontitis is a chronic, progressively worsening disease affecting the periodontal ligament, the gingiva and the dentoalveolar bone [1]. It is characterised by a migration of the boundary epithelial cells (keratinocytes), breakdown of the connective tissue and Sharpey’s fibres and a depletion of the alveolar bone due to immunological hyperactivity of the local cells [2]. The tissue destruction leads to the formation of a pocket and hence, to sub-gingival plaque, which cannot be reached by mechanical plaque control. A characteristic feature of the periodonto-pathogenic pocket is that it provides ample space for a large number of micro-organisms, inflammation cells, exudates and concretion [1,3].
Diagnosis of periodontal diseases requires recording of clinical, periodontal variables: Probing Depth (PD), Attachment Loss (AL) and Bleeding on Probing (BOP). PD, AL and BOP are the most frequent methods used to diagnose a destructive periodontal disease. Possible measurement errors in recording the periodontal findings are dependent on the measurement method, precision of reading, angulations of the probing tip, fluctuation of inflamed gingiva, and inflammatory status of the tissue and documentation errors in the transfer of data [4–7]. Further imprecision is introduced when findings are taken by two different users [8].
A variety of measurement methods are available in the market to take findings. Conventional probes have a production linked inaccuracy of ±1mm [9]. Regarding this aspect and the varying penetration pressure new probes were developed in recent years. First generation probe were focussing on pressure audit [10–12] and resolution [13]. Further stage of probes such as Florida- [14] or Toronto-Probe [15] were computer-linked and provided a more comfortable use. However, they are not in common dental use. The probes exhibit one main drawback: the missing tactile sensation. The large number of variables such as probe pressure, design of the probe tip and reading options and therefore reading precision means that there are substantial differences in the measurement results and hence, also in diagnosis and even the course of therapy [16,17].
The patient’s perception of pain while using the probe is a preventative factor in terms of compliance and hence, the willingness to submit to recurring diagnosis and subsequent therapy by means of Scaling and Root Planing (SRP). The perception of pain associated with the use of the probe varies depending on the group of teeth. The upper jaw incisors are most sensitive to pain, while sensitivity around the molars is substantially lower [18,19].
The costs of long-term periodontitis therapy and dental preservation are substantially lower compared to the costs of follow-up treatment after the loss of teeth among patients with periodontal damage, where treatment may involve implants or dental bridges [20]. This would suggest that regular diagnosis and suitable therapy are sensible measures. It is reasonable to assume that findings can be taken with sufficiently exact measurement values, and that reproducible findings can also be obtained over a longer period, even if more than one user is involved. Moreover, it can be presumed that management of treatment requiring less time and fewer personnel would enable a lower exposure of pain, and would hence, encourage a long term treatment that can be applied more consistently by the user, with greater cost effectiveness, and with greater acceptance by the patient.
This clinical trial investigated the differences between two measurement methods (automated controlled force probe - PA-ON, manual probe using millimetre scale) used to determine periodontal parameters. Its purpose was to determine whether there are differences with respect to measurement precision, time needed for measurement and the subjective perception of pain by the patient.
Materials and Methods
Study Design: This clinical investigation was approved by the Ethics Commission at the Medical Faculty in Leipzig (288-14-14072014). Before commencing the study, all study participants were informed of its content and the use of personal data and confirmed in writing their voluntary willingness to take part. A manual measurement with a standard probe using a millimetre scale (PCPUNC15 [HuFriedy, Tuttlingen, Germany]) and an electronic, pressure-calibrated probe (PA-ON probe [Orange Dental, Biberach, Germany]) were compared.
Study Subjects: Two male users examined 25 patients of either sex in a dental practice.
The inclusion criteria for the study participants were: Age ≥18 years, periodontal screening index codes degrees 3 and 4, at least 4 teeth per quadrant, required or active periodontitis treatment, voluntary consent to participate in the trial.
The patient were informed in writing and verbally about the objectives of, and reasons for the trial. The patients understood the objectives of, and reasons for the trial. The patients who gave informed consent were included in the study.
The exclusion criteria for the study were: Patients with legal guardians/disabled patients, patients declared legally incompetent to provide consent, blood clotting disorders, immunodeficiency and pregnancy/lactation.
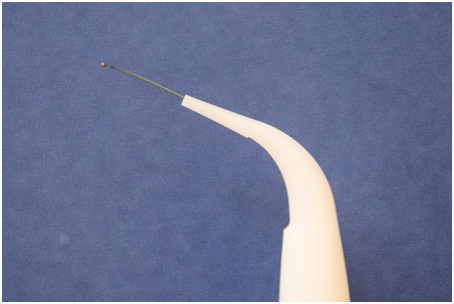
Data Collection: Each study participant was examined using both measurement methods in an interval of 24 hours (±1h). The following will refer to the electronically pressure-calibrated method (PA-ON probe [Orangedental, Biberach, Germany]) [Table/Fig-1,2] as EM, and to the standard manual method (PCPUNC15 [HuFriedy, Tuttlingen, Germany]) [Table/Fig-3] as MM. The PA-ON probe possesses a graphic display, and was capable of emitting sound. The display showed the current measurement point by means of a tooth symbol and lettering. Speech output could also be activated to indicate the measurement points. The tip of the probe was flexible and fitted with a ball (diameter 0.5mm).
Electronic, periodontal probe with graphic display (PA-ON, Orange Dental Germany).

Disposable electronic probe tip (in detail).
Standard manual probe (PCPUNC15, HuFriedy Germany).
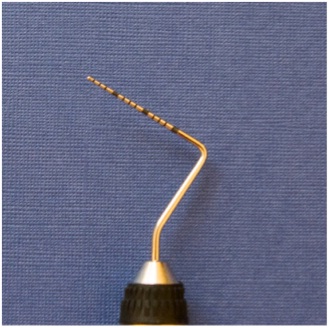
The standard probe had a laser-engraved millimetre scale, and was rigid. The tip of the probe was rounded (diameter 0.5mm).
The users then performed calibration with micro scales (measurement accuracy 1/100g) immediately before taking the findings. Here, the probe force was adjusted gradually to 20Ncm by means of 10 pressure tests on micro scales. Repeated calibration measurements were conducted for intra- and inter- examination on one quadrant in eight patients, and resulted in k=0.87. This calibration was not necessary for the EM, as the tip of the probe yields at a pressure of 20Ncm (manufacturer’s information). For a better handling, examiners had already used the electronic probe for a minimum of 10 times on other patients before.
The findings were taken by two male users (user 1 and user 2). The sequence of the measurement methods (1. MM and EM; 2. EM and MM) and the users (1. user 1 and 2; 2. user 2 and 1) and also how they were applied to the study participants, were randomized.
A computer generated randomization table was used to recruit and blindly randomize 25 participants for the initial electronic or manual measurements. The randomization was executed by a dental assistant not participating in the study.
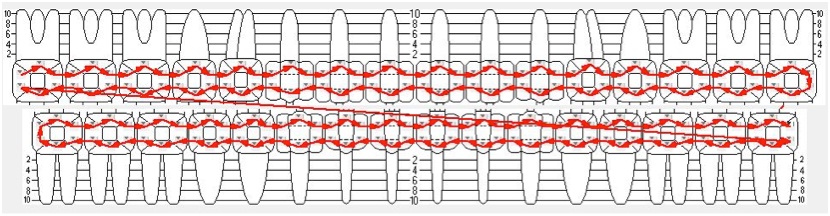
For each finding, the PD and AL were recorded in millimetres, along with the BOP and the time required for taking findings. PD, AL and BOP were measured at 6 points on each tooth (3606 measuring points, 601 teeth). Findings were taken in the identical way as shown in the diagram [Table/Fig-4].
Procedure of systematology measurement.
The documentation of findings for the MM took place simultaneously; the user stated the values and a chair assistant recorded them. The documentation of findings for the EM took place by saving the measurement values in the probe, which were then transferred digitally in a docking station once all of the findings had been taken. A stopwatch with a round dial divided into quadrants was used to measure the time for MM and EM (Schütt PC-71, Marburg, Germany). The time data was divided into a total time (Time_total), a time to take findings for PD and AL (Time_PD/AL) and a time to take findings for BOP (Time_BOP).
Perception of Pain: Following the examination, each study participant used a Visual Analogue Scale (VAS) to assess and document the subjective perception of pain experienced during the procedure of taking findings [Table/Fig-5]. This documentation was accomplished separately for MM and EM. The VAS was subdivided from 0 – 100 in steps of 1mm, whereby 0 = no pain and 100 = maximum pain [21].
Visual analogue scale for pain assessment.

Statistical Analysis
SPSS for Windows, Version 19.0 (SPSS Inc., U.S.A.), was used to conduct the statistical analyses.
The measurement data was reviewed in terms of normal distribution by application of the Kolmogorov-Smirnov test (significance correction according to Lilliefors) and the Shapiro-Wilk test. The data were analyzed using the paired t test. Significance was reviewed for all tests performed, whereby a p-value of <0.05 was assumed to be statistically significant for all tests. The Chi-square-test for independence was performed to review the significance of the grouped pocket depths (classification into groups of 1-3mm, 4-6mm and ≥7mm).
The required sample number was calculated assuming a very small effect due to the lack of preliminary examinations. G-Power calculated a required case number of 23 persons.
Results
A total of 25 study participants (13 women and 12 men) with an average age of 53 years (25-76 years) were examined [Table/Fig-6a,b]. A total of 24 sets of valid participant data were analyzed. A partial error in transferring of clinical data precipitated the dropout.
Clinical results for manual (MM) and electronic probing (EM).
| PD_EM,[mm] | PD_MM[mm] | AL_EM[mm] | AL_MM[mm] | BOP_EM[%] | BOP_MM[%] | VAS_EM[mm] | VAS_MM[mm] | Age[year] |
|---|
| N | 24 | 24 | 24 | 24 | 24 | 24 | 24 | 24 | 24 |
| Mean | 2.8 | 2.93 | 0.44 | 0.55 | 44 | 53 | 29.1 | 37.2 | 52.96 |
| SD | 1.38 | 1.5 | 1.01 | 1.09 | 5 | 5 | 15.6 | 23.3 | 13 |
PD- probing depth; AL- attachment loss; BOP - bleeding on probing; VAS- visual analogue scale for pain
Time taken results for manual (MM) and electronic probing (EM).
| Time_total [sec] | Time_PD/AL [sec] | Time_BOP [sec] |
|---|
| EM | MM | EM | MM | EM | MM |
|---|
| N | 24 | 24 | 24 | 24 | 24 | 24 |
| Mean | 799 | 814 | 654 | 646 | 149 | 168 |
| SD | 165 | 195 | 119 | 168 | 50 | 38.7 |
PD- probing depth; AL- attachment level; BOP-bleeding on probing; sec-seconds
A comparison between EM and MM [Table/Fig-7] determined a mean value of -0.14 (SD=0.297) with a significant difference (p=0.03) for PD, a mean value of -0.10 (SD=0.327) with no significant difference (p=0.064) for AL, and a mean value of -0.09 (SD=0.147) with a significant difference (p=0.010) for BOP.
Statistical significances (paired t test) between electronic (EM) and manual (MM) technique for PD, AL and BOP.
| Variable | mean | SD | p-value | d | power |
|---|
| PD_diff | -0.14 | 0.297 | 0.03* | -0.24 | - |
| AL_diff | -0.10 | 0.327 | 0.064 | -0.13 | 0.42 |
| BOP_diff | -0.09 | 0.147 | 0.01 | -0.47 | - |
*p<0.05 – significant. PD- probing depth; AL- attachment loss; BOP-bleeding on probing.
There is no significant difference between the measurement values recorded by the measurement methods EM and MM in respect to the total time [Table/Fig-8] required to take findings (p=0.331/d=0.08) and the measurement of time required to ascertain pocket depth and attachment level (p=0.909/d=0.058). The time required to take findings of bleeding on probing indicates a significantly smaller value for EM (p=0.004) [Table/Fig-8]. The VAS values show a significantly smaller value for EM (p=0.048).
Statistical significances (paired wilcoxon-test) between electronic (EM) and manual (MM) technique for time taking and VAS (visual analogue scale for pain).
| Variable | Time_total_difference | Time_PD/AL_difference | Time_BOP_difference | VAS_difference |
|---|
| Z | -0.971 | -0.114 | -2.915 | -1.895 |
| p-value | p = 0.331 | p = 0.909 | p = 0.004* | p = 0.048* |
| effect | d = 0.08 | d = 0.058 | d = 0.419 | d = 0.408 |
*p<0.05 – significant. PD- probing depth; AL- attachment loss; BOP-bleeding on probing, VAS- visual analogue scale for pain
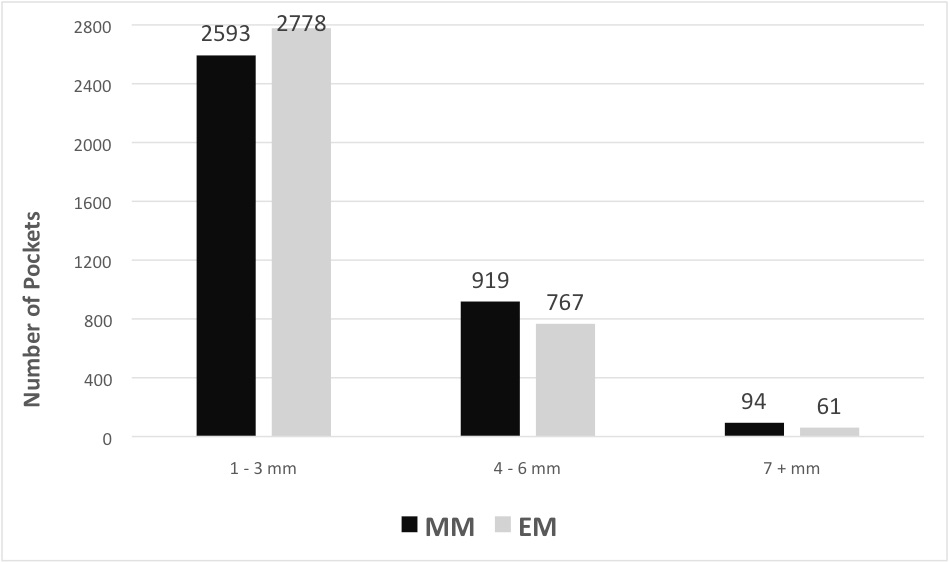
The distribution of measured PD [Table/Fig-9] shows a significantly greater number of pockets recorded by the EM in a depth of 1-3mm, and a larger number of pockets measured by the MM in a depth of 4-6mm and ≥7mm. This was statistically significant (p<0.001).
Numbers of different probing depths measured in the electronic probing (EM) and manual MM) groups (chi-square-test).
Discussion
It is assumed that the pressure-calibrated method delivers reproducible results, even with different users [22]. Other studies obtained more reproducible measurements for manual probing [23,24]. We observed a difference in VAS score for the experience of pain compared to the standard manual probe. It is reasonable to conclude that the study electronic probe is able to reduce patient’s perception of pain. Further, one can assume that working with an electronic probe is just as much a question of practice and a learning curve, and that different skill levels in its handling may also return different values.
It is accepted that there is no difference between the pressure-calibrated methods in terms of time needed to take findings [25]. We determined that in general, the electronic probe needed less time recording the BOP. This time advantage is due to the more efficient, display-assisted data recording and data transmission that the electronic probe offers. In contrast to the manual probe measurement where a chair assistant transfers the data the docking station for the electronic probe takes this transmission process. Hence, study electronic probe present a commercial benefit for independent practices, as they permit a single user concept, which in itself may put the high investment costs needed to purchase the probe into perspective. This, combined with the apparently lower perception of pain by the patients, could foster more continuous supportive periodontics therapy acceptance among patients and hence, a more continuous use by the practitioner; thus, contributing to more differentiated monitoring of periodontal health. Possible transmission errors compared with the manual method that are based on inadequate data communication between the user and the documentation assistant can be excluded owing to the automatic saving of measurement values in the electronic probe itself. This increases documentation certainty in ongoing practice routines.
It is reasonable to assume that the flexibility and slender design of the study electronic probe tip, compared with the rigid tip of the standard hand-held probe, is better suited to reach the base of a periodontal pocket, as it is more equipped to follow the curvature of the root. Furthermore, one can presume that the study electronic probe is better suited to probing tight vertical defects. This might permit more realistic measurement values and hence, a more precise representation of the severity of the disease. Broadly speaking, measurements conducted with an electronic pressure-calibrated probe are considered equivalent to the standard method in terms of measurement accuracy for pocket depths [26–28]. This has already been demonstrated in earlier investigations conducted using comparable product/probes such as the Florida probe and the Florida disk in comparison to standard manual measurement methods [29]. The substantial flexibility of the probe tip and the consequent severe reduction in orientation and tactile sensation in the pocket of the gum must be considered a disadvantage. Furthermore, the introduction of flexible probe tip to the sulcus region of healthy periodontal pockets within the vestibular area of the tooth is made more difficult as the tip is susceptible to bending. The design of the device means that the maximum probe depth is limited to 11mm. Therefore, it is not possible to take findings when facing severe manifestations of periodontitis with deep vertical defects. Secure introduction of the probe tip into the pocket in the distal molar region is made difficult due to limited space in the oral cavity and the size of the probe itself.
The PA-ON probe delivers comparable measurement results for PD and VAS values compared with a manually pressure-calibrated probe, as shown in a previous paper [25]. The measurement values relating to PD in our trial, as recorded by the electronically pressure-calibrated and the standard method, exhibit a statistical difference. We observed higher values for PD and AL by manual probing versus electronic measurements as also discussed by former investigations [23]. These distinctions may impact the course of therapy in terms of excessive or insufficient treatment. It is reasonable to assume that the user applies greater pressure to investigate the base of deeper pockets using the manual method. It can be presumed that an excessive use of the manual instruments may lead to traumatization of the periodontal region. The simultaneously elevated BOP values and higher VAS values lend further credence to this assumption. It appears likely that the pressure-calibrated electronic probe permits a gentler probing to prevent any traumatization of the periodontal region. On the other hand the specific design of the electronic probing tip led to small impressions on the marginal gingiva while measuring the PD. According to that the distance from the marginal gingiva to the bottom of the pocket will be reduced. Further lower PD measured by electronic probing may result in the under diagnosis of periodontal disease.
We should also mention the aspect of a differing inflammation situation in periodontal pockets depending on varying forms of periodontitis. Increase of tissue inflammation led to a reduction of resistance against the probing pressure. As a result probing tip penetration had deeper values for inflamed periodontal ligament than at healthy sites [7,30]. Accordingly prior studies [23] obtained higher values for manual probing in groups with severe periodontitis whereas, in groups with mild or moderate forms of periodontitis the electronic probe (Florida probe) showed higher AL values. It is assumed that the electronic probe, which operates with constant force, is able to indicate an AL earlier than this would be possible using standard measurement probes [24]. Also untreated patients had a less resistant gingival tissue where higher probing forces by manual probing in comparison with a controlled electronic probing could lead to distorted measurements. Further studies taking periodontal variables before and after active therapy would be necessary and proposed.
The electronic pressure-calibrated measurement has certain restrictions when detecting pocket depths higher than 7mm. Furthermore the length of the electronic probe tip, which is due to its design, means that additional application of the manual method for PD and AL greater than 11mm and for relatively inaccessible measurement points is necessary. It would be desirable that further studies will be performed to investigate user-dependent influences. Different periodontal inflammation status could also influence the probing value. More investigations regarding the severity of the periodontal disease and the phase of periodontal treatment are necessary.
Conclusion
The limitations caused by the design of the electronic probe do not permit a complete replacement of standard manual probes at the present time. The recording of the measurement by one single user can be seen as an economic benefit in practice routines. It is reasonable to assume that patients will exhibit greater acceptance of regularly taken periodontal findings due to the lower perception of pain especially in cases of highly inflammed tissue.
Conflict of Interest: The authors declare that they have no conflict of interest with any part of this study.
Contribution: The First and the Second (AR & LT) author contri-buted in preparation of the manuscript, literature research, translation, internal communication, proof reading and publication process. Third author (AS) contributed in statistical analysis and creation of tables. Fourth author (FS) was the head for statistical analysis and correction. Fifth Author (HJ) was the head for clinical research and allocation of the subjects.
PD- probing depth; AL- attachment loss; BOP - bleeding on probing; VAS- visual analogue scale for pain
PD- probing depth; AL- attachment level; BOP-bleeding on probing; sec-seconds
*p<0.05 – significant. PD- probing depth; AL- attachment loss; BOP-bleeding on probing.
*p<0.05 – significant. PD- probing depth; AL- attachment loss; BOP-bleeding on probing, VAS- visual analogue scale for pain