Many patients present to general surgeons with scalp lesions which require wide local excision with margin, following which the defect is too large to be closed primarily. These lesions can be benign or malignant. Skin grafting of these defects gives poor cosmetic outcome. Knowledge of basic flaps will enable the general surgeon to close these defects to heal by primary intention. Also, the margin of excision will not be compromised because of anticipated difficulty in closing the wound. We present a series of three cases who underwent excision of scalp lesions resulting in moderate size scalp defects. These defects were closed with rotation flap with good cosmetic outcome.
Cosmetic Outcome, Dermatofibroma protuberans, Histopathology
Introduction
General surgeons very often see patients with large swellings in the scalp which require some sort of flap cover for primary wound closure. Many a times, anticipating difficulty in closure, the surgical resection margins are compromised. This results in positive margins of resection, requiring adjuvant therapy in some cases and also having higher chances of local recurrence. A repeat excision will have further difficulties in achieving wound closure.
We present a series of three cases of lesions on the scalp which underwent wide local excision followed by rotation flap closure with good outcomes. Rotation transposition flaps can be done by general surgeons with basic knowledge of flap construction and does not require formal plastic surgery training. The cases are described below.
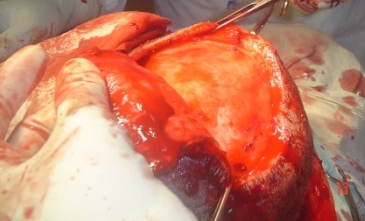
Case 1
A 63-year-old male reported with a swelling over the left fronto-parietal scalp. The swelling was 5cm in diameter with mobility over the underlying bony skull. Contrast enhanced computed tomography scan suggested the possibility of a pilomatrixoma. He underwent wide local excision with a 0.5cm margin. The wound was closed with a rotation flap. The histopathology was reported as dermatofibroma protuberans [Table/Fig-1,2 and 3].

Six months after surgery.

Case 2
A 43-year-old male patient presented with a swelling over the right fronto-temporal scalp. The swelling was 6cm in diameter and CT head suggested a pilar cyst. There was no intracranial extension. The final diagnosis was trichilemmal (pilar) cyst. A 6cm defect was obtained after excision of the swelling with a 0.5cm margin. This was closed with a rotation flap [Table/Fig-4,5].


Case 3
A 56-year-old lady on a permanent pacemaker presented with a swelling in the left fronto parietal scalp. The histopathology was reported as trichilemmal (pilar) cyst. This patient also underwent an excision followed by a rotation flap closure of the defect [Table/Fig-6,7 and 8].


Hair growth at four months after surgery.

All patients underwent thorough preoperative workup. Under general anaesthesia, a wide local excision with a 0.5cm margin was carried out. The flap incision was marked out preoperatively with the diameter of the defect forming the base of a triangle. The length of the flap to be mobilized was around five times the diameter of the defect. If there was tension on the flap during rotation a back cut was made at the end opposite to the defect to enable primary closure without tension. Anteriorly, dissection was carried out into the forehead to mobilize for primary closure. All wounds were closed with suction drains. The average operative time was one hour and blood loss was insignificant. The blood loss occured mainly at the time of scalp incision and not during mobilization of the flaps. There was no postoperative haematoma and drains were removed on day two after surgery. The average postoperative stay was two days. There was no periorbital oedema, wound infection or flap necrosis. Despite the extensive nature of dissection for raising the flaps, the postoperative pain was not significant and patients were managed with oral analgesics from day 1. However, a visual analog scale for pain was not maintained.
Cases were followed for upto six months after surgery. There was good hair growth over the transposed flap. The sutures were removed by the seventh day. Except for minor flap edge necrosis in one case, there were no other major problems. The suture lines had healed and the overall cosmetic outcome was good. However, the female patient, though she had good hair growth over the transposed flap, had lower rate of growth, which at four months had not reached the length of the hair on the posterior aspect of the scalp.
Discussion
Scalp lesions form a common presentation to the general surgeon. Dermatofibrosarcoma protuberans is an uncommon tumour, making up less than 0.1% of all malignancies and less than 2% of soft tissue tumours. Wide local excision forms the mainstay of treatment with adjuvant radiotherapy occasionally [1]. Trichilemmal cysts are intradermal or subcutaneous cysts, a majority of which occur in the scalp, where they form the most common cutaneous cysts [2]. Although benign, they may be locally aggressive and malignant transformation and metastasis has been described [3].
One study of head and neck lesions found epidermoid cysts to be the most common swelling in the head and neck region. Of the lesions found in the scalp, pilar (trichilemmal) cysts were the more common swelling in the scalp. Majority of the lesions peaked in the third decade with almost equal male to female incidence [2]. Malignant lesions in the scalp are also seen. A study reviewing the incidence of different pathologies seen in scalp lesions found 7.8% incidence of malignancies or lesions needing follow up. The common histopathologies found were trichilemmal cyst, epidermal cyst, lipoma, nevus and sebaceous cyst in decreasing order of frequency [4]. Non-melanoma malignant skin tumours arise due to direct sun exposure. Complex defects are seen after surgery for advanced lesions where the bone and dura mater may be opened. Reconstruction with free flaps has been described in such cases. Multidisciplinary approach will be required in such cases [5].
A basic understanding of the scalp anatomy and its blood supply is essential for every general surgeon. The scalp is described as being of five layers – the skin with its characteristic thick dermis, the subcutaneous tissue, the relatively rigid galea aponeurotica, which is continuous with the superficial musculoaponeurotic system, frontalis, occipitalis, and superficial temporal fascia, underlying areolar tissue and then the periosteum. Both, the internal and the external carotid arteries, supply the scalp. The supratrochlear and supraorbital branches of the ophthalmic artery, a branch of the internal carotid supply mainly the forehead and anterior scalp. The superficial temporal, posterior auricular and occipital artery arise from the external carotid artery provides three branches to the scalp.
Scalp defects arising from excision of moderate sized lesions can be approached in various ways. While skin grafting is an easy option, the cosmetic outcome is not the best. Hair does not grow on the grafted skin. Patients with more hair, falling into Norwood class I-IV would have a higher cosmetic expectation with respect to scalp hair pattern as compared to those in the higher class V-VII [6]. Flap repairs may give better outcomes in selected patients. Many types of flaps are possible in the scalp. The most commonly used flaps include rotation flaps and bipedicle advancement flap [7].
A study has described an algorithm for the management of scalp defects taking into account the age, sex, scalp hair distribution, history of skin cancer, regression with radiotherapy and American Society of Anaesthesiology (ASA) score. Intraoperative measurement of the defect and the presence or the absence of pericranium layer will provide indications for other indicated reconstruction strategies [6]. The authors grouped patients into five reconstructive categories including primary closure, skin grafts, local scalp flaps, application of dermal regeneration template with splint-thickness skin graft and free flap reconstruction. They observed that defects that are less than 5cm2 in size or diameter of 2.5cm can be usually closed primarily. Frontal and parietal scalp is more rigid and less elastic and smooth and here it may be difficult to close these defects with primary closure. Local or regional flaps were used for reconstruction in patients with defects of moderate size (5 to 20cm2) and a score less than 5. With a score more than 5, split thickness or full thickness grafts were used. In larger defects with area more than 20cm2 and score less than 5, free tissue transfer was done. With higher scores, acellular dermal matrix was used for immediate cover followed by split skin graft [6].
Limited elasticity of the scalp due to the tight galea necessitates planning for a rotation flap for moderate sized defects. These flaps have hair-bearing skin and may aid in healing in patients with compromised wounds. The good vascularity of the scalp usually prevents flap necrosis. This study did not find residual pain or hypertrophic scar during follow up. The diameter of the rotation flap should be five times the defect diameter. The double hatchet flap is another flap that has been described. The rotation flap is a big scar in only one direction while in the double hatchet flap, the scar is in two opposite directions [6].
During the creation of the rotation flap, the dissection takes place deep to the galea in the loose areolar tissue. This tissue is avascular and hence, the surgeon will not encounter much bleeding even during extensive dissection for mobilization of the flap. However, haematomas can arise from bleeding into this space from the superficial layer and hence good haemostasis and wound drainage is required.
Reconstruction of the scalp may be challenging because of the special anatomic structure of the scalp and underlying skeleton. Anterior scalp defects especially deserve special care for pleasant hairline re-creation and redirection of hair follicles. Local transposition or rotation flaps are the most common reconstruction methods for moderate or large anterior scalp defects [8]. The lateral and posterior aspects are usually used as donor sites to avoid distortion of the forehead or frontal hairline. The flaps are designed to include axial vessels in their bases. Usually, the superficial temporal artery or the occipital artery provides the basic blood supply to these flaps. The flaps should be designed with respect to previous incisions, which may block vascular inflow to the flap [7].
The defects of scalp following the excision of benign or malignant tumours, burns or secondary to trauma should be ideally replaced with hair bearing scalp. It not only gives aesthetic results but also reconstructs the defect with a tissue of the same histology. Local flaps when transposed or rotated can lead to dog ear formation. If the defect is large the rotated flaps are inadequate. In the cases where donor site is not closed primarily the secondary defect is grafted with skin, resulting in bald patches. Unilateral rotation scalp flaps based on temporal vessels may also be a good choice, but they move the hairline downwards [9].
Conclusion
Defects arising from excision of some of these lesions cannot be closed primarily. A basic idea of simple flap closure like a rotation flap can enable proper excision of the lesion with negative margins and good cosmetic outcome. However, for recurrent lesions with previous scars or more extensive defects, plastic surgery help may be required.
[1]. Maguire R, Nikolorakos D, Lam A, Dermatofibrosarcoma protuberans: The role of tissue expansion in reconstructive surgery of the scalpInt J Surg Case Rep 2016 19:137-39. [Google Scholar]
[2]. Al-Khateeb TH, Al-Masri NM, Al-Zoubi F, Cutaneous cysts of the head and neckJ Oral Maxillofac Surg 2009 67(1):52-57. [Google Scholar]
[3]. Weiss J, Heine M, Grimmel M, Jung EG, Malignant proliferating trichilemmal cystJ Am Acad Dermatol 1995 32:870-73. [Google Scholar]
[4]. Türk CÇ, Bacanlı A, Kara NN, Incidence and clinical significance of lesions presenting as a scalp mass in adult patientsActa Neurochir (Wien) 2015 157(2):217-23. [Google Scholar]
[5]. Igde M, Yilanci S, Bali YY, Unlu RE, Duzgun S, Pekdemir I, Reconstruction of tissue defects developing after excision of non-melanoma malignant skin tumours in scalp and forehead regionsTurk Neurosurg 2015 25(6):888-94. [Google Scholar]
[6]. Cherubino M, Taibi D, Scamoni S, Maggiulli F, Di Giovanna D, Dibartolo R, A new algorithm for the surgical management of defects of the scalpISRN Plastic Surgery 2013 2013:1-5.n. [Google Scholar]
[7]. Papadopoulos O, Karypidis D, Moustaki M, Chrisostomidis C, Grigorios C, Epaminondas K, Double scalping flap: a versatile technique in scalp reconstructionJ Craniofac Surg 2009 20(5):1484-91. [Google Scholar]
[8]. Gundeslioglu AO, Selimoglu MN, Doldurucu T, Bekerecioglu M, Reconstruction of large anterior scalp defects using advancement flapsJ Craniofac Surg 2012 23(6):1766-69. [Google Scholar]
[9]. Sharma R, Sirohi D, Sinha R, Menon PS, Reconstruction of a large posterior scalp defect using occipital artery based pedicled island v–y advancement flap: A Case ReportJ Maxillofac Oral Surg 2011 10(3):262-65. [Google Scholar]