Accuracy of Pelvic Mass Score in Pre-operative Determination of Malignancy in Adnexal Masses
Lakshmi Mohan1, Arun Rao2, Sonali Ullal3, Gowtham Krishna4
1 Assistant Surgeon, Govt. Urban Health Training Centre (UHTC), Ambalappuzha, Kerala, India. [Formerly (During Study Period), Junior Resident, Department of Obstetrics and Gynecology, Kasturba Medical College, Mangalore, India].
2 Professor, Department of Obstetrics and Gynecology, Kasturba Medical College, Mangalore, Karnataka, India.
3 Professor, Department of Radiology, Kasturba Medical College, Mangalore, Karnataka, India.
4 Junior resident, Department of Radiology, Kasturba Medical College, Mangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Lakshmi Mohan, Anandasadanam, House No.29A, Plakkudy L ane, Ambalappuzha, Alappuzha-688561, Kerala, India.
E-mail: drlakshmimohan18@gmail.com
Introduction
Suspicious adnexal masses are common clinical problems in gynaecological practice. A reliable diagnostic tool for the early detection of the ovarian malignancy is essential.
Aim
To validate a new scoring system –Pelvic Mass Score (PMS) in predicting the nature of the adnexal mass pre-operatively.
Materials and Methods
A prospective observational study was carried out in 100 consenting women with an undiagnosed adnexal mass requiring operative intervention. Among them 62 patients had mass with a feeding vessel in which the Doppler velocimetry study values were available. The PMS was determined in these 62 patients. A score of 29 or more was taken as suggestive of malignancy. The results were compared with the histopathological diagnosis to confirm malignancy. The chi-square test was applied to test the significance.
Results
Among the 62 patients with vascular mass, 31 had histopathological diagnosis of malignancy. The statistical analysis of the data with PMS with 29 as cut-off revealed 100% sensitivity and 100% Negative Predictive Value (NPV) as there was no false negative case detected. But the specificity and Positive Predictive Value (PPV) was poor; 45.2% and 64.6% respectively. Based on the Receiver Operating Characteristic (ROC) curve, if we redefine cut-off as 69, specificity increases to 80.6% with a sensitivity of 90.3%, the PPV and NPV being 82.35 and 89.29 respectively.
Conclusion
The present study concludes that, in suspicious vascular adnexal masses PMS can be used as a reliable diagnostic score to predict malignancy if we redefine the existing cut-off of 29 to 69.
Ovarian cancer, Tumour vascularity, Ultrasound scoring system
Introduction
Suspicious adnexal masses are common clinical problems in gynaecological practice. The average age adjusted incidence rate for ovarian cancer is around 6.0 per 100,000 population in Indian urban registries [1]. The age specific incidence rate for ovarian malignancy shows that the disease increases from 35 years and peaks by 55-64 years [2]. Lack of early warning symptoms and signs make ovarian cancer a silent killer. More than 70% of all patients with carcinoma ovary seek treatment after there has been regional or distant spread. Only less than 25% of the patients present with Stage I disease, the treatment of which is associated with a 5 year survival rate of 90% [3].
The differentiation of benign from malignant adnexal masses is of great therapeutic significance. Hence, the pre-operative detection of the nature of adnexal mass becomes extremely important for appropriate management. Ultrasonography is the primary imaging modality for confirmation of the ovarian origin of the mass and the characterization of the nature of the mass. Several scoring systems for classifying and scoring the abnormalities in the form of morphological index have been proposed in the past [4–7]. However, when the morphological features alone were applied to the prediction of ovarian mass, there was a tendency to overdiagnose malignant tumours.
The introduction of colour Doppler ultrasonography has allowed the evaluation of tumour vascularity. Several studies have assessed the value of this technique in the differentiation of benign from malignant adnexal masses with controversial results [8–10]. On the other hand, several tumour markers have been also used to differentiate benign from malignant adnexal tumours. The most used and studied is serum CA125 [10–12]. It is elevated in epithelial ovarian tumours, but is not tumour specific. It may be elevated in women with nonmalignant diseases such as leiomyomas, endometriosis and salphingitis which are more common in pre-menopausal women. Hence this marker has been found to be more useful in post-menopausal patients with suspicious adnexal masses.
Various scoring systems have been proposed in the past that associate a score with specific morphological, flowmetry and biochemical parameters (CA 125) and the menopausal status of the patient, such as the Risk Malignancy Index (RMI)-1, RMI-2, RMI-3 etc., [13,14].
Pelvic Mass Score (PMS) is a new scoring system proposed by Rossi et al., which incorporates the sonomorphological index - Sassone Score, the logarithmic value of CA125, the type of vascularity, menopausal status and the resistive index of the adnexal mass [15].
The formula proposed is-

where SASS is the numerical value of Sassone score, Log (CA-125) is the base 10 logarithm of the CA125 levels, VAS is the type of vascularisation (peripheral = 1; central/septal= 2), MS is the menopausal status (pre-menopausal=1; post-menopausal=2) and RI is the numerical value of the resistive index of the pelvic mass.
The present study aimed to evaluate the validity of this new scoring system- PMS, in accurate pre-operative prediction of malignancy in suspicious adnexal masses.
Materials and Methods
A prospective study was carried out in 100 consecutive consenting women attending the gynaecological services of a tertiary teaching hospital in southern India, during the study period between July 2012 to June 2013.
Inclusion criteria
A clinically palpable (per abdominally or vaginally) adnexal mass
An adnexal mass of more than 5 cm incidentally picked up by routine ultrasonogram.
Pregnant women with adnexal mass were excluded from the study. The study was approved by the Hospital Ethics committee. After noting the demographic details of the patient, ultrasonographic examination (transvaginal or transabdominal) was performed using General Electronics Voluson, 3-5 MHz Trans Vaginal Ultrasounds (TVS) probe with Pulsed Doppler System by a trained radiologist to assess the characteristics of the adnexal masses with respect to the wall structure, thickness, solid areas, presence of papillary projections, septations, the thickness of these and the echogenic pattern.
The Sassone score was calculated. The blood flow wave forms were assessed by insonating the beam at the growing area like the papillae, septa or solid areas to identify the feeding vessel. The location of feeding vessel- peripheral/central/septal and the Doppler parameters – the pulsatile index and the resistive index were measured. The blood samples were sent to estimate the serum CA 125 levels pre-operatively. Using these parameters, the Pelvic mass score was calculated using the above mentioned formula. A value more than 29 was considered indicative of malignancy, as suggested in the original study by Rossi et al., [15]. The results were compared with histopathological findings obtained from laparotomy, laparoscopy or Fine Needle Aspiration Cytology (FNAC).
Results
The mean age of the patients under the study was 42.48 ±15.38 years. The youngest patient was 13 years of age and the eldest 78 years. Among the total 100 cases, 61 were pre-menopausal and 39 attained menopause. From the histopathological data of the 100 operated masses, 28 cases were malignant ovarian tumours, 3 borderline tumours, and 69 cases were benign masses. The 3 borderline tumours were considered under malignant group for the purpose of analysis.
Malignancy rate in post-menopausal subjects were more than 3 times higher in comparison to the pre-menopausal age group; accounting to be 53.3% (21 patients among the 39 post-menopausal women had malignancy). The mean age of the patient with malignant masses was 50.48 years.
Among the 100 patients with suspicious adnexal masses, 62 patients had adnexal mass with feeding vessel, either central or peripheral. In these 62 patients, 69.4% (43 cases) had either central or septal vascularity and peripheral vascularity was noted in 30.6% (19 cases). Hence, the Doppler indices and the PMS could be assessed only in this subset of 62 patients.
The diagnostic performance of PMS (with the cut-off of 29) in premenopausal women and post-menopausal women are shown in [Table/Fig-1&2] respectively. The overall diagnostic value of PMS irrespective of the age was noted to be sensitivity-100%, specificity-45.2%, PPV-64.6% and NPV-100% [Table/Fig-3].
Diagnostic performance of PMS (cut-off-29) in pre-menopausal women.
| Prediction by PMS | HISTOPATHOLOGY | Total |
|---|
| Malignant | Benign |
|---|
| Malignant | 10 | 10 | 20 |
| Benign | 0 | 10 | 10 |
| 10 | 20 | 30 |
p<0.001
Diagnostic performance of PMS (cut-off-29) in post-menopausal women.
| Prediction by PMS | HISTOPATHOLOGY | Total |
|---|
| Malignant | Benign |
|---|
| Malignant | 21 | 7 | 28 |
| Benign | 0 | 4 | 4 |
| 21 | 11 | 32 |
p<0.001
Overall diagnostic performance of PMS (cut-off-29).
| SENSITIVITY | SPECIFICITY | PPV | NPV |
|---|
| Premenopausal | 100 | 50.0 | 50.0 | 100 |
| Postmenopausal | 100 | 36.4 | 75.0 | 100 |
| Overall | 100 | 45.2 | 64.6 | 100 |
p<0.001
PPV : Positive Predictive Value; NPV : Negative Predictive Value
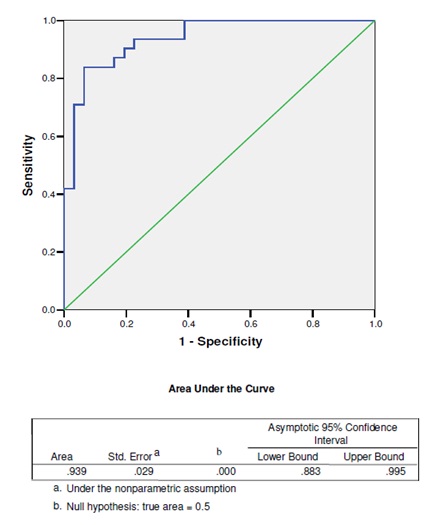
According to the Receiver Operating Characteristic (ROC) curve [Table/Fig-4] obtained, it was noted that if the existing cut-off of 29 is raised to 69, improves the sensitivity and specificity, as depicted in [Table/Fig-5,6 and 7].
Receiver Operating Characteristic (ROC) curve of PMS.
Diagnostic performance of PMS (cut-off-69) in pre-menopausal women.
| Prediction by PMS | HISTOPATHOLOGY | Total |
|---|
| Malignant | Benign |
|---|
| Malignant | 7 | 2 | 9 |
| Benign | 3 | 18 | 21 |
| 10 | 20 | 30 |
p<0.001
Diagnostic performance of PMS (cut-off-69) in post-menopausal women.
| Prediction by PMS | HISTOPATHOLOGY | Total |
|---|
| Malignant | Benign |
|---|
| Malignant | 21 | 4 | 25 |
| Benign | 0 | 7 | 7 |
| 21 | 11 | 32 |
p<0.001
Overall diagnostic performance of PMS (cut-off-69).
| SENSITIVITY | SPECIFICITY | PPV | NPV |
|---|
| Premenopausal | 70.0 | 90.0 | 77.78 | 85.71 |
| Postmenopausal | 100 | 63.64 | 84.0 | 100 |
| Overall | 90.3 | 80.64 | 82.35 | 89.29 |
p<0.001
PPV : Positive Predictive Value; NPV : Negative Predictive Value
Discussion
The sensitivity of morphologic analysis with USG in predicting malignancy in ovarian tumours has been shown to be 85%–97%, whereas its specificity ranges from 56% to 95% [7,8,10]. Doppler flowmetry has yielded variable results in distinguishing benign from malignant masses, with a sensitivity of 50%–100% and a specificity of 46%–100% [9,11]. Differing results are partly due to varying threshold values and corresponding trade-offs between sensitivity and specificity.
With regard to CA125, Michalak M et al., in a recent study reported a sensitivity and specificity of 85.2% and 63.6%, respectively [16]. Importance of CA125 in diagnosis of suspicious adnexal masses is that it is a non-observer dependant, self evident blood test. But due to its non specific nature, more so in pre-menopausal women, its diagnostic accuracy cannot be relied on completely.
The recent scoring system PMS proposed by Rossi et al., takes into account all these parameters- Sassone score, vascular distribution, resistance index and menopausal status all of which have been proven by various studies to have statistically significant association with the risk of malignancy [15]. Hence, the diagnostic performance was expected to be excellent. According to the present study when the cut-off score is taken as 29, PMS has a high sensitivity and NPV, however, the false positives detected were high, yielding a very poor specificity. But the existing cut-off when raised to 69, improves the specificity to 80.6% with a high sensitivity of 90.3%.
Conclusion
The PMS is a composite of multiple parameters having statistically significant association with the risk of ovarian malignancy. The present study, indicates that, PMS can be used as reliable diagnostic tool to predict the nature of a suspicious adnexal mass when its cut-off score is changed from 29 to a value of 69. However, a larger prospective study is required to confirm the validity of PMS with the present suggested cut-off.
p<0.001
p<0.001
p<0.001
PPV : Positive Predictive Value; NPV : Negative Predictive Value
p<0.001
p<0.001
p<0.001
PPV : Positive Predictive Value; NPV : Negative Predictive Value
[1]. Yeole BB, Trends in cancer incidence in female breast, cervix uteri, corpusuteri, and ovary in IndiaAsian Pac J Cancer Prev 2008 9(1):119-22. [Google Scholar]
[2]. Murthy NS, Shalini S, Suman G, Pruthvish S, Mathew A, Changing trends in incidence of ovarian cancer - the Indian scenarioAsian Pac J Cancer Prev 2009 10(6):1025-30. [Google Scholar]
[3]. Hennessy BT, Coleman RL, Markman M, Ovarian cancerLancet 2009 374(9698):1371-82. [Google Scholar]
[4]. Sassone AM, Timor-Tritsch IE, Artner A, Westhoff C, Warren WB, Transvaginal sonographic characterization of ovarian disease: evaluation of a new scoring system to predict ovarian malignancyObstet Gynaecol 1991 78:70-76. [Google Scholar]
[5]. Lerner JP, Timor-Tritsch IE, Federman A, Abramovich G, Transvaginal ultrasonographic characterization of ovarian masses with an improved, weighted scoring systemAm J Obstet Gynaecol 1994 170:81-85. [Google Scholar]
[6]. DePriest PD, Gallion HH, Pavlik EJ, Kryscio RJ, van Nagell JR, Transvaginal sonography as a screening method for the detection of early ovarian cancerGynaecol Oncol 1997 65(3):408-14. [Google Scholar]
[7]. Ferrazzi E, Zanetta G, Dordoni D, Berlanda N, Mezzopane R, Lissoni AA, Transvaginal ultrasonographic characterization of ovarian masses: comparison of five scoring systems in a multicenter studyUltrasound Obstet Gynaecol 1997 10(3):192-97. [Google Scholar]
[8]. Barroilhet L, Vitonis A, Shipp T, Muto M, Benacerraf B, Sonographic predictors of ovarian malignancyJ Clin Ultrasound 2013 41(5):269-74. [Google Scholar]
[9]. Shah D, Shah S, Parikh J, Bhatt CJ, Vaishnav K, Bala DV, Doppler ultrasound: a good and reliable predictor of ovarian malignancyJ Obstet Gynaecol India 2013 63(3):186-89. [Google Scholar]
[10]. Hartman CA, Juliato CR, Sarian LO, Toledo MC, Jales RM, Morais SS, Ultrasound criteria and CA 125 as predictive variables of ovarian cancer in women with adnexal tumoursUltrasound Obstet Gynaecol 2012 40(3):360-66. [Google Scholar]
[11]. van Nagell JR, DePriest PD, Management of adnexal masses in postmenopausal womenAm J Obstet Gynaecol 2005 193:30-35. [Google Scholar]
[12]. Partheen K, Kristjansdottir B, Sundfeldt K, Evaluation of ovarian cancer biomarkers HE4 and CA-125 in women presenting with a suspicious cystic ovarian massJ Gynaecol Oncol 2011 22(4):244-52. [Google Scholar]
[13]. Håkansson F, Høgdall EV, Nedergaard L, Lundvall L, Engelholm SA, Pedersen AT, Danish ‘Pelvic Mass’ ovarian cancer ctudy. Risk of malignancy index used as a diagnostic tool in a tertiary centre for patients with a pelvic massActa Obstet Gynaecol Scand 2012 91(4):496-502. [Google Scholar]
[14]. Ong C, Biswas A, Choolani M, Low JJ, Comparison of risk of malignancy indices in evaluating ovarian masses in a Southeast Asian populationSingapore Med J 2013 54(3):136-39. [Google Scholar]
[15]. Rossi A, Braghin C, Soldano F, Isola M, Capodicasa V, Londero AP, A proposal for a new scoring system to evaluate pelvic masses: Pelvic Masses Score (PMS)Eur J Obstet Gynaecol Reprod Biol 2011 157(1):84-88. [Google Scholar]
[16]. Michalak M, Gąsiorowska E, Markwitz EN, Diagnostic value of CA125, HE4, ROMA and logistic regression model in pelvic mass diagnostics - our experienceGinekol Pol 2015 86(4):256-61. [Google Scholar]