Scrub typhus (ST) is an emerging infectious disease in India and is being reported from almost every state [1–6]. ST was originally thought to be a disease of war and confined to jungles is now prevalent in both rural and urban areas. This might be perhaps due to the migration of people and clearing of forests for building houses, factories etc. The ‘tsutsugamushi triangle’ [7] is now slowly expanding to other continents – Africa, Europe and South America [8–10]. ST research is facilitated by the availability of specific rapid Point-of-Care test (PoC) and other conventional serological tests like ELISA, Indirect Immunofluroescence Assay (IFA) and molecular diagnostic test targeting Orientia tsutsugamushi DNA. ELISA tests are accessible to most of the laboratories in the world including those in remote areas. Three serological kits for Scrub Typhus were used in this project: Two ELISA kits based on Immunochromatography (ICT), viz., InBios Scrub Typhus Detect IgM Rapid Test (USA) and ImmuneMed Scrub typhus Rapid kit (South Korea). These two were compared against the reference standard test InBios Scrub Typhus Detect IgM ELISA which is a conventional ELISA test that takes about three hours and the samples can be tested only in batches. Additionally, the Weil-Felix (WF) test which is commonly used in developing countries was also performed. Our objective of this study was to evaluate the performance of InBios Scrub Typhus Detect IgM Rapid Test against ImmuneMed Scrub typhus Rapid and the non-specific but routinely used WF test. The kit under evaluation detects specifically ST IgM antibody only, which reflects acute status of the disease, whereas, another rapid ST ICT kit available in India for the past six years (SD Bioline Tsutsugamushi, South Korea) detects total antibody of IgM/IgG/IgA.
Materials and Methods
This prospective research work was carried out during an eight month period (November 2015 to June 2016) in Mahatma Gandhi Medical College and Research Institute, a Tertiary Care Super Specialty Teaching Hospital, Puducherry, India. A total of 220 consecutive patients who came to this hospital during the above period from various places in Puducherry and Tamil Nadu, Southern India were included. This study was approved by our Institutional Human Ethical Committee (IHEC). Written informed consent was obtained from all patients prior to collection of blood samples. About 3ml blood was collected in Clot activator tube and the serum was separated and kept frozen at -20°C till the time of testing.
Inclusion criteria: High grade fever with or without chills and rigour; fever with rash/eschar/hepatosplenomegaly/jaundice/lymphadenopathy/thrombocytopenia; fever with constitutional symptoms like malaise, myalgia, nausea, vomiting; fever with capillary leak syndrome (Pleural effusion, ascitis, pedal oedema); and fever with bleeding diathesis (petechia, purpura)/fever with shock.
Exclusion criteria: Immunocompromised patients like AIDS/lymphomas; malignancy secondaries; bleeding disorders and fever of more than four weeks duration (pulmonary tuberculosis, etc.,).
In our hospital, ST is routinely screened by ST Rapid ICT test followed by other serological tests for Fever of Unknown Origin (FUO) patients. Whenever possible, following laboratory investigations were done: Total WBC count, platelet count, haemoglobin, serum bilirubin, Alkaline Phosphatase (ALP)/Serum Glutamate Oxaloacetate Aminotransferase / Alanine transferase (SGOT/ALT)/ Serum Glutamate Pyruvate Aminotransferase / Aspartate transferase (SGPT/AST), urea, serum creatinine and albumin. Additional tests included: Peripheral blood films for malarial parasite/malarial antigen detection (J. Mitra & Co. Pvt. Ltd.), Widal test (Span Diagnostics), Dengue NS1/IgM/IgG detection (SD Bioline Dengue Duo kit, Seoul, South Korea) and Leptospiral serology (IgM/IgG - SD Bioline Leptospira IgM/IgG, Seoul, Korea). In our present study, ST serology included the following tests:
ST Detect IgM ELISA (InBios International, Seattle, U.S.A) (Conventional ELISA);
ST Detect IgM Rapid Test (InBios International, Seattle, U.S.A);
ImmuneMed ST Rapid kit (ImmuneMed, Chuncheon, Gangwon-do, South Korea);
WF Test – Proteus OXK (Plasmatec, South El Monte, California, USA).
ST IgM InBios ELISA: These ELISA plates with 96 wells were coated with ten recombinant antigens of O. tsutsugamushi, targeting antibodies to the 56-kDa antigen. The test was performed in accordance with procedure outlined by the kit manufacturers. Briefly, after absorption with Rheumatoid Factor (RF) sorbent, serum samples and controls were diluted 1:100 with diluent. After incubation and washing of ELISA plates, OD (Optical Density) readings were taken at 450nm in iMark Microplate Reader (Bio-Rad, Japan). Cut-off values were calculated and interpretation of the test results was computed as reported earlier [6]. Briefly, 20 samples from healthy volunteers from ST endemic area were tested by IgM InBios ELISA and average OD value was taken as cut-off value. Cut-off values were calculated as follows:
Cut-off value = Average of the Normal Human Sera (NHS) + three times SD of NHS. The samples with OD values above the Cut-off (0.560) were considered positive and those below the Cut-off were taken as negative. Borderline samples were tested in triplicate.
InBios Scrub Typhus Detect IgM Rapid Test: The test was performed in accordance with the technical brochure provided in the kit. Briefly, 3μl of serum samples were added to the strip, followed by the addition of three drops of Chase buffer provided in the kit. Results were read within 15-20 minutes. A single red line appears on the control area and if the patient has ST antibody, a second red line appears on the test area [Table/Fig-1].
1, ST Result InBios IgM and ImmuneMed Rapid ICT Kits.
JA-46/16 - ST IgM Positive in both rapid kits.
AP-6/16 - ST IgM Negative in both rapid kits.
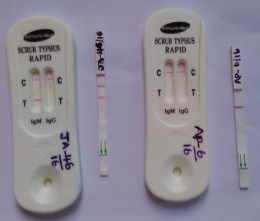
ST ImmuneMed kit: This Rapid ELISA cassette is coated with a mixture of recombinant antigen cr56, kr56 and r21 of Orientia tsutsugamushi. The test was carried out in accordance with the kit manufacturers’ instructions and as described earlier [11] [Table/Fig-1].
Weil-Felix test: Proteus OXK colored antigen (Plasmatec, South El Monte, Calif., USA) was used. Patients’ serum dilutions from 1:20 to 1:640 were used in the initial screen and those with more than 1:640 were titrated further. A single OXK titer of ≥ 1:320 was considered as suggestive of ST.
Statistical Analysis
Sensitivity, specificity, PPV and NPV were calculated considering ST IgM ELISA as gold standard.
For other parameters (Chi-square, Spearman’s correlation and Kappa) statistical analysis was performed using IBM SPSS Statistics 17 for Windows (SPSS Inc; Chicago, USA).
Results
Among 220 patients with acute febrile illness and clinical suspicion of ST, 140 were seropositive for O. tsutsugamushi IgM antibody in InBios Rapid ELISA and/or ImmuneMed Rapid/InBios ELISA. However, only 134 patients were positive in reference standard InBios IgM ELISA and among these patients, 127 were positive in all three kits, viz., both rapid kits and InBios ELISA. InBios Rapid kit has given highest positivity of 139. Regarding WF test, only 66 patients had single OXK titers of ≥ 1:320. OXK agglutinin titers ranged from ≤ 1:20 to 1:20,480. Against the reference standard IgM InBios ELISA test, the Immunochromatography tests InBios and ImmuneMed had shown commendable levels of sensitivity and specificity of 99.25%, 93.02% and 94.87%, 94.19% respectively. With a cut-off titre of OXK 1:320, WF test had a low sensitivity of 50.38%, but a high specificity of 95.51%.
Statistical analysis of InBios, ImmuneMed and WF against the InBios IgM conventional ELISA as reference is presented in [Table/Fig-2]. Between the two groups of patients, statistically significant difference (p≤0.05) was observed in few parameters like malaise, chills and rigor, hepatomegaly and lymphadenopathy. The clinical and laboratory findings of two categories of patients namely, children (0-14 years) and adults (≥15 years) are presented in [Table/Fig-3].
Comparison between InBios Rapid, ImmuneMed Rapid IgM, WF (OX K) and IgM ELISA (n=220). WF=Weil-Felix test.
| % Overall accuracy (95%CI) |
|---|
| Test | Agreement(Kappa factor)(95%CI) | Sensitivity[95%CI] | Specificity[95%CI] | Positive PredictiveValue (PPV)(95%CI) | Negative PredictiveValue (NPV)(95%CI) |
|---|
| InBios Rapid IgM | Vs IgM | 0.932(0.883- 0.982) | 99.25%(95.91-99.98) | 93.02% (85.43- 97.40) | 95.68% (90.84- 98.40) | 98.77%(93.31- 99.97) |
| Immune Med Rapid IgM | Vs IgM | 0.886(0.823 -0.949) | 94.87%(89.53-97.87) | 94.19% (86.95-98.09) | 96.21% (91.38-98.76) | 92.05%(84.30-96.74) |
| WFTitre ≥1:320 | VsIgM | 0.413(0.315- 0.512) | 50.38%(41.52- 59.23) | 95.51% (88.89- 98.76) | 94.29% (86.01- 98.42) | 56.67 % (48.34-64.73) |
Clinical and Laboratory parameters of ST (Scrub typhus) IgM Positive patients (n=140).
| Clinical/Laboratory findings | Children(0-14years)(n=61) | Adult(≥ 15 years)(n=79) | Total(n=140) | p- values* |
|---|
| Fever ≤ 7 days | 21 | 36 | 57 | 0.183285 |
| Fever ≥ 7 days | 40 | 43 | 83 | 0.183285 |
| Chills and Rigor | 32 | 56 | 88 | 0.025256 |
| Myalgia | 21 | 36 | 57 | 0.183285 |
| Headache | 35 | 33 | 68 | 0.91948 |
| Cough and Expectoration | 33 | 49 | 82 | 0.345107 |
| Abdominal Pain | 18 | 26 | 44 | 0.621696 |
| Hepatomegaly | 15 | 9 | 24 | 0.04497 |
| Splenomegaly | 9 | 18 | 27 | 0.283016 |
| Malaise | 35 | 19 | 54 | 0.000059 |
| Nausea | 19 | 29 | 48 | 0.491834 |
| Vomiting | 26 | 40 | 66 | 0.346488 |
| Pneumonitis | 2 | 9 | 11 | 0.113192 |
| Eschar | 18 | 25 | 34 | 0.78575 |
| Rash | 5 | 4 | 9 | 0.502973 |
| Lymphadenopathy | 24 | 15 | 39 | 0.007718 |
| Pedal oedema | 0 | 5 | 5 | 0.068319 |
| Platelet Count (≤1.5 Lacs) | 12 | 24 | 36 | 0.150614 |
| Increased Liver Enzymes (AST/ALT/ALP)£ | 6 | 17 | 23 | 0.070588 |
| Creatinine (>1.0) | 8 | 14 | 22 | 0.492578 |
| Leucocytosis (>11,000Cu mm) | 13 | 21 | 34 | 0.470816 |
| Leucopenia (<4,000Cu mm) | 7 | 15 | 22 | 0 .251102 |
*p-values <0.05 were considered significant
£ AST – Aspartate Transaminase/ALT – Alanine Transaminase/ALP – Alkaline Phosphatase
Discussion
IFA, the gold standard test for serological diagnosis of ST has been performed by researchers from overseas and a few from India [11–15]. According to a latest Indian report, sensitivity and specificity of ST IFA was 100% and 93.5%, respectively [12]. ST IFA kit needs to be presently imported. In addition, circulation of a large number of O. tsutsugamushi genotypes in different geographical locations in India makes it difficult to incorporate all the commonly prevalent genotypes in IFA kits. Only a few recent Indian reports [16] identified Kato, Karp, Gilliam, Ikeda and Neimeng-65 genotype strains, the first two (Kato and Karp) being the most prevalent genotypes. Thus, the knowledge of genotypes circulating in different parts of our country is still incomplete. Due to the highly specific, but subjective nature of IFA test demanding high interpretational skills, ELISA has been recommended by different researchers [12–15].
ST IgM InBios ELISA (conventional ELISA) has been validated by us and several researchers in India and abroad with satisfactory performance, qualifying as an alternate reference test to IFA [4–6,12–15,17].
ST InBios Rapid kit (ICT), although available in Indian market for the past one year, has not been validated so far. Hence, we present our findings validating this kit for ST serodiagnosis with sensitivity and specificity of 99.25%, 93.02% respectively. Kingston et al., from Thailand, validated this kit against the gold standard IFA and reported a satisfactory performance of 92% sensitivity and 95% specificity [15].
ImmuneMed rapid kit is not yet available in India. The kit has been validated by Korean researchers and found to have 98.6% sensitivity and 98.2% specificity [11]. In our present study, ImmuneMed rapid kit performed equally well with 94.87%, sensitivity and 94.19% specificity.
WF test, although a non-specific test is still routinely used in third world countries. We have got WF positivity of 66 with the cut-off titre of ≥1:320. There is difference of opinion regarding the single significant titre of Proteus OXK agglutinin in WF as suggestive of acute ST by researchers from India and other countries. The recommended titres varied from 1:80 [1,2,12,18], 1:160 [13,19] and 1:320 [3,7,20]. The sensitivity, specificity, PPV and NPV values were calculated for these three cut-off titres for OXK agglutinins. There was a proportional decrease in sensitivity like 81.34%, 65.67%, and 50.38%, when the cut-off titres considered were 80, 160 and 320 respectively. However, there was an increase in specificity of 70.93%, 94.19%, 95.51% when higher titres were considered namely 80, 160 and 320 respectively. A positive WF test per-se is not a conclusive proof for ST infection and has to be correlated with clinical findings.
Clinical features, laboratory results and demographic details of the patients between the two groups of patients (children and adults), could identify that more number of children had malaise, hepatomegaly and lymphadenopathy (p≤0.05), whereas chills & rigor was observed in more adults (p≤0.05).
In our experience, InBios Scrub typhus IgM Detect Rapid kit (USA) is both sensitive and specific. SD Bioline Tsutsugamushi kit is already available in India for the past six years, but this kit detects total antibody of IgM/IgG/IgA and does not discriminate between acute disease and immune status of ST. Contrast to this kit, InBios kit targets only the IgM antibody, and hence, acute cases of ST could be detected, thus, facilitating earlier intervention and prevention of complications. This kit is cost-effective and as a PoC test would benefit resource poor remote and rural laboratories in India.
Limitation
IFA test is the ‘gold standard’ for diagnosing rickettsial infections. We could not carry out IFA and molecular diagnostic test like PCR since, kits are to be imported and technically demanding.
Conclusion
InBios Scrub typhus IgM Detect Rapid kit (USA) is affordable and reliable for use in resource poor laboratories. Until ST IFA and molecular diagnostic tests are standardized and readily available in India, this rapid ICT kit could serve the purpose of early diagnosis of acute scrub typhus. Results of WF test need to be interpreted with caution.
*p-values <0.05 were considered significant
£ AST – Aspartate Transaminase/ALT – Alanine Transaminase/ALP – Alkaline Phosphatase