Intestinal Type Adenocarcinoma from Inverted Papilloma: A Rare Recurrence
Garima Singh1, Meeta Singh2, Mansi Chandana3, Sompal Singh4, Namrata Nargotra5
1 Senior Resident, Department of Pathology, NDMC Medical College and Hindu Rao Hospital, Malka Ganj, Delhi, India.
2 Assistant Professor, NDMC Medical College and Hindu Rao Hospital, Malka Ganj, Delhi, India.
3 Senior Resident, NDMC Medical College and Hindu Rao Hospital, Malka Ganj, Delhi, India.
4 Specialist, NDMC Medical College and Hindu Rao Hospital, Malka Ganj, Delhi, India.
5 Head of Department, NDMC Medical College and Hindu Rao Hospital, Malka Ganj, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sompal Singh, Room no. 202, 2nd Floor, G-Block, Hindu Rao Hospital, Malka Ganj, Delhi-110007, India.
E-mail: sompal151074@gmail.com
Inverted Papilloma (IP) is an uncommon and locally aggressive benign tumour of sinonasal region, which tends to recur after surgical resection. Most tumours are confined to the lateral nasal wall and sinuses, with maxillary sinus being most commonly affected and a male preponderance. It has a known association with in situ and invasive carcinomas with a <10% rate of malignant transformation. Most common association has been seen with squamous cell carcinoma and extremely rare association with adenocarcinoma and small cell carcinoma. A 36-year-old male presented with a left sided polypoidal nasal mass and underwent a polypectomy. Pathology results showed IP with mild dysplasia. The polypoidal growth reappeared on the same side after a period of 10 months and on histopathological examination, the growth revealed features of intestinal type adenocarcinoma. IP recurring as adenocarcinoma is rare and even after exhaustive literature search only few cases could be found. Two studies have described recurrence of adenocarcinoma in existing IP previously. We report an unusual case of inverted papilloma showing malignant transformation into an intestinal type adenocarcinoma in a 36-year-old male patient within 10 months of previous surgery.
Nasal blockage, Polypoidal, Sinonasal
Case Report
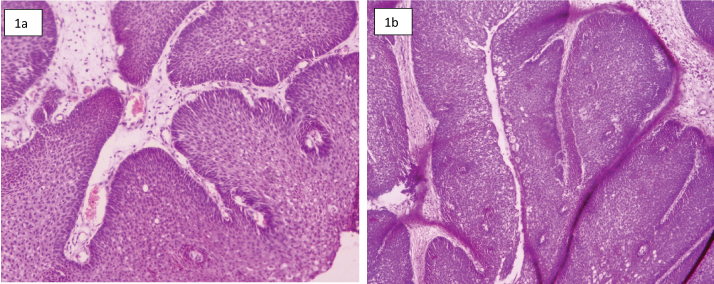
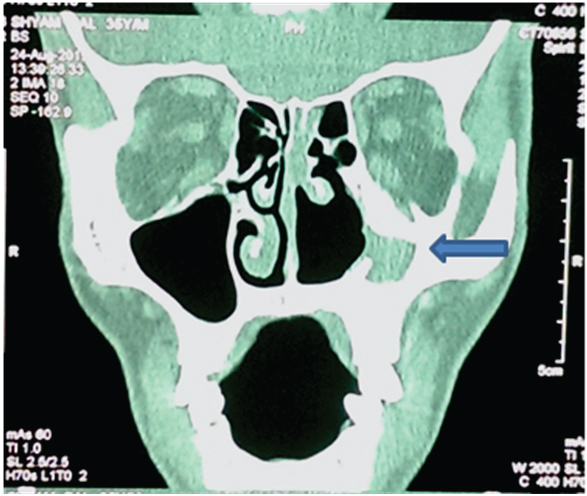
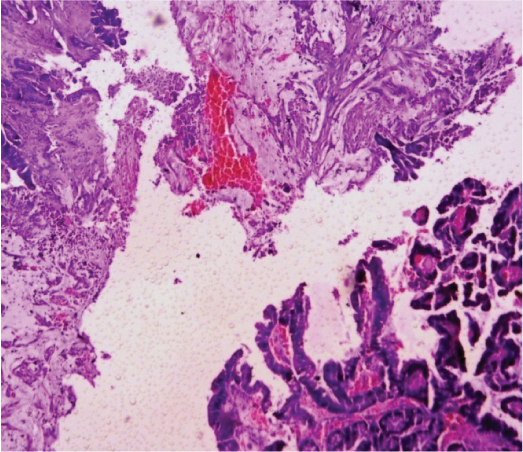
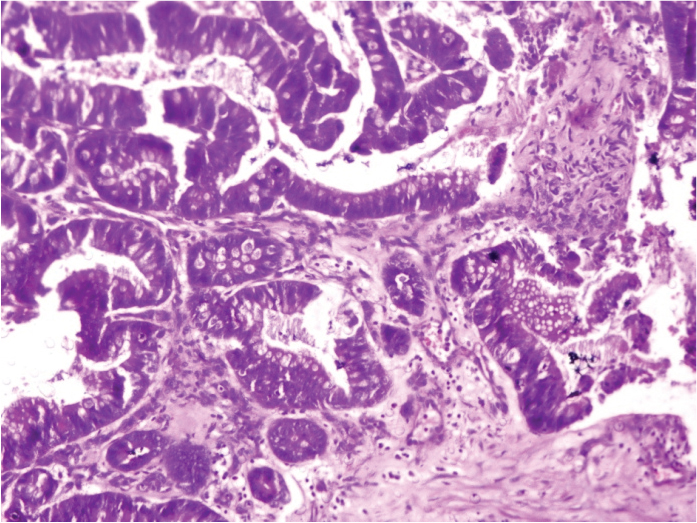
A 36-year-old male presented to Eye, Nose & Throat (ENT) clinic with a history of nasal blockage. The patient was noted to have left sided nasal polypoidal mass. Patient underwent polypectomy, followed by histopathological examination showing features of Inverted Papilloma (IP) with mild dysplasia [Table/Fig-1]. Margins were positive and incomplete excision was suspected. Clinician was informed about the margins and patient was kept under close follow-up. He presented with nasal blockage and nasal bleeding after 10 months. Physical examination and complete neurological evaluation were unremarkable. Computerized Tomography (CT) of head and neck showed collapsed maxillary sinus filled with soft tissue mass, destruction of osteomeatal complex and irregular, sclerosed margins of maxillary sinus [Table/Fig-2]. Polypectomy with wider resection margins was performed. Histopathology of the multiple tiny greyish white polypoidal soft tissue pieces showed predominant papillary architecture and invasive back to back glands with presence of goblet cells, columnar cells and mucinous cells [Table/Fig-3,4]. Columnar cells lining the papillae and glands showed vesicular to hyperchromatic nuclei (Grade I). Variable number of goblet cells was seen without any squamoid differentiation. Margins were positive and background showed mucin pools. To rule out any gastrointestinal metastasis patient was sent for CT abdomen, which revealed no abnormality. A diagnosis of intestinal type adenocarcinoma was given. Following the report patient underwent radiation therapy and was kept under close follow-up for any recurrence till the time of submission of article.
(a,b) Microphotographs showing Inverted papilloma (H&E, 40X and 10X).
Computerized Tomography (CT) head and neck showing soft tissue mass (arrow) in maxillary sinus along with local bony destruction.
Microphotograph showing branched papillae in the background of mucin pool (H&E, 4X).
Microphotograph showing branched papillae lined by columnar cells with vesicular to hyperchromatic nuclei admixed with variable number of goblet cells (H&E, 10X).
Discussion
IP are benign neoplastic proliferation of multilayered non- keratinizing squamous epithelium. IP is the most common type of benign Schneiderian papilloma. It most commonly involves lateral nasal wall and sinuses. The lesion predominates in elderly males (6th-7th decade) [1,2]. Numerous risk factors proposed in literature are allergy, environmental carcinogens, sinusitis, polyposis and Human Papilloma Virus (HPV) [1]. Clinically IP presents with unilateral nasal obstruction along with other symptoms like epistaxis, anosmia, nasal discharge, facial pain and epiphora [2].
IP is an inverted or endophytic proliferation of non-keratinizing squamous epithelium into the underlying stroma and it originates from ectoderm of the olfactory plate. Along with non-keratinized squamous cells, admixed ciliated respiratory epithelium, transitional cells, mucous and goblet cells are also seen. Mitotic activity is variable ranging from rare to frequent mitosis [3–5]. The present case showed no mitotic activity, necrosis or any other cell differentiation. Intra-epithelial microcysts containing macrophages, neutrophils, mucin and cell debris is a distinctive finding seen in IP [3,4]. Usually atypia is not seen in IP; however, its presence is not accompanied by increased mitotic activity or dyskeratosis as is seen in malignant transformation. Stroma of IP shows mixed inflammatory infiltrate along with odematous, myxomatous or fibrous change with no seromucus glands [3,4].
IP has a well known association with in situ and invasive carcinoma, predominantly with squamous cell carcinoma. Most of the series report 5 to 32% rate of malignant transformation [4]. In literature HPV 6, 11 and 16 are mentioned to play a significant yet not well understood role in pathogenesis of IP [6,7]. HPV is considered to be a risk factor for recurrence [6].
Association of IP with squamous cell carcinoma has been well documented in literature, but rarely adenocarcinoma or small cell carcinoma has been reported [2]. Incidence of squamous cell carcinoma associated with IP is 5 to 15% in most large series, however, only two studies have described occurrence of adenocarcinoma in existing IP cases [2,3,6,8]. Kerschner JE et al., reported a rare case of IP associated with squamous cell carcinoma and adenocarcinoma [8].
Adenocarcinoma of sinonasal tract are a diverse group of neoplasms which are classified by WHO-2005 into salivary and non salivary type which is then further divided into intestinal and non intestinal type [9]. Overall, incidence of sinonasal adenocarcinoma is 12.6%, out of which Intestinal Type Adenocarcinoma (ITAC) have an incidence of only 1.4% of tumours in the sinonasal region [10,11]. Only few cases of IP transforming into adenocarcinoma are found in literature after an exhaustive search. Most common age of presentation is 55-60 years [12]. Exposure to wood dust and breathe dust increases the risk of adenocarcinoma to 900 times [12]. Tumours arising in individuals with occupational exposure affect men in 85-95% cases whereas sporadic cases frequently arise in women [12]. Sites of origin reported in literature for ITAC are ethmoid sinus, 40%; nasal cavity, 28%; maxillary antrum, 23% and indeterminate, 9% [12].
Most commonly patient presents with nasal obstruction, epistaxis, rhinorrhea, mass in cheek and exophthalmos. Grossly the tumour is similar to colonic adenocarcinoma. ITAC commonly shows microscopic features like colonic adenocarcinoma. On immunohistochemistry ITACs are positive for pancytokeratin, epithelial membrane antigen and B72.3. Carcinoembryonic antigen positivity can be seen occasionally which is also expressed virtually by all colonic adenocarcinoma. But in a study, only two out of 12 ITAC’s showed strong staining for this antigen. However, chromogranin shows more strong positivity in ITAC and rarely in colonic adenocarcinoma [13].
CT plays an important role in work-up of IP as it provides a good estimation of extent of disease; hence, helpful in complete resection of tumour. Patients with ITAC should be fully examined to rule out any metastasis from GIT or breast. In our patient barium enema study and CT abdomen showed no abnormality. Sinonasal ITAC shows local recurrence, regional lymph nodes and distant metastasis in 50%, 8% and 13% of patients, respectively [14]. Complete surgical resection with adjuvant radiation therapy to the region of the tumour is the optimal treatment plan for sinonasal ITAC. These lesions are known to be locally destructive and ultimately lethal neoplasm with only papillary type having a slightly better prognosis [12,15].
Conclusion
IP can present as a destructive lesion with high rate of recurrence on incomplete resection and significant incidence of malignancy. Most common association is with squamous cell carcinoma but very rarely with adenocarcinoma. Sinonasal adenocarcinoma is rare aggressive neoplasms with high mortality reported. Long term follow up is recommended because IP are known to have recurrence as malignancy and not every time the transformation is into squamous cell carcinoma, but rarely into adenocarcinomas also.
[1]. Weissler MC, Montgomery WW, Turner PA, Montgomery SK, Joseph MP, Inverted papillomaAnn Otol Rhinol Laryngol 1986 95:215-21. [Google Scholar]
[2]. Phillips P, Gustafson RO, Facer GW, The clinical behavior of inverting papilloma of the nose and paranasal sinuses: Report of 112 cases and review of the literatureLaryngoscope 1990 100:463-69. [Google Scholar]
[3]. Hyams VJ, Papillomas of the nasal cavity and paranasal sinuses. A clinicopathological study of 315 casesAnn Otol Rhino1 Laryngol 1971 80:192-206. [Google Scholar]
[4]. Michaels L, Young M, Histogenesis of papillomas of the nose and paranasal sinusesArch Pathol Lab Med 1995 119:821-26. [Google Scholar]
[5]. Nielsen PL, Buchwald C, Nielsen LH, Tos M, Inverted papilloma of the nasal cavity: pathological aspects in a follow-up studyLaryngoscope 1991 101:1094-101. [Google Scholar]
[6]. Lawson W, Schlecht NF, Brandwein-Gensler M, The role of the human papillomavirus in the pathogenesis of schneiderian inverted papilloma: an analytical overview of the evidenceHead Neck Pathol 2008 2:49-59. [Google Scholar]
[7]. Gaffey MJ, Frierson HF, Weiss LM, Barber CM, Baber GB, Stoler MH, Human papillomavirus and Epstein-Barr virus in sinonasal schneiderian papillomas. An in situ hybridization and polymerase chain reaction studyAm J Clin Pathol 1996 106:475-82. [Google Scholar]
[8]. Kerschner JE, Futran ND, Chaney V, Inverted Papilloma Associated With Squamous Cell Carcinoma and Adenocarcinoma: Case Report and Review of the LiteratureAm J Otolaryngol 1996 17:257-59. [Google Scholar]
[9]. Franchi A, Santucci M, Wenig BM, Adenocarcinoma. In: Barnes L, Eveson JW, Reichart P, Sidransky D, edsPathology and genetics head and neck tumours. World Health Organization classification of tumours 2005 LyonIARC Press:20-3. [Google Scholar]
[10]. Turner JH, Reh DD, Incidence and survival in patients with sinonasal cancer: A historical analysis of population-based dataHead Neck 2012 34:877-85. [Google Scholar]
[11]. Boor A, Jurkovic I, Durdrikova K, Kavecansky V, Friedmann I, Intestinal-type sinonasal adenocarcinoma: a sporadic caseJ Laryngol Otol 1996 110:805-10. [Google Scholar]
[12]. Barnes L, Intestinal-type adenocarcinoma of the nasal cavity and paranasal sinusesAm J Surg Pathol 1986 10:192-202. [Google Scholar]
[13]. McKinney CD, Mills SE, Franquemont DW, Sinonasal intestinal type adenocarcinoma: immunohistochemical profile and comparison with colonic adenocarcinomaMod Pathol 1995 8:421-26. [Google Scholar]
[14]. Imbus HR, Dyson WL, A review of nasal cancer in furniture manufacturing and woodworking in North Carolina, the United States, and other countriesJ Occup Med 1987 29:734-40. [Google Scholar]
[15]. Mills SE, Fechner RE, Cantrell RW, Aggressive sinonasal lesion resembling normal intestinal mucosaAnn J Surg Pathol 1982 6:803-09. [Google Scholar]