Peritoneal Recesses of Human Duodenum
P.A. Nandagopalan1, Cessy Job2, M.B. Prasanna3
1 Professor, Department of Anatomy, P.K. Das Institute of Medical Sciences, Ottapalam, Palakkad, Kerala, India.
2 Additional Professor, Department of Anatomy, Govt. Medical College, Kottayam, Kerala, India.
3 Additional Professor, Department of Anatomy, Govt. Medical College, Kottayam, Kerala, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Cessy Job, Additional Professor, Department of Anatomy, Govt. Medical College, Kottayam-686008, Kerala, India.
E-mail: drcessy@gmail.com
Duodenum, Duodenal recesses, Internal hernia, Strangulation
There are small pockets or fossae in the peritoneal cavity, which are bounded by folds of peritoneum called peritoneal recesses. Duodenal recesses are peritoneal recesses surrounding duodenum. Sometimes coils of small intestine may enter these recesses, known as internal hernia and may get strangulated.
This study was conducted to find out the incidence of duodenal recesses, which can lead to internal herniation. Eighty specimens of human duodenum were observed for this study. These were obtained from Department of Anatomy and Forensic Medicine of Govt. Medical College, Kottayam, Kerala. The age group ranged from still born to 80 years. The recess was identified using naked eye examination as well as using magnifying lens and a gloved finger was introduced to detect, the direction of its opening into the peritoneal cavity.
The following are the results of our observation
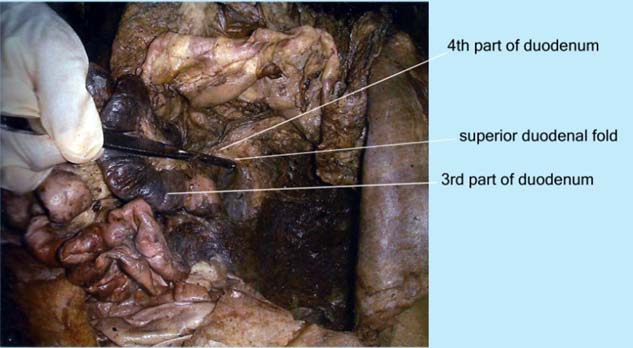
Superior Duodenal Recess (SDR) was seen in 34 cases. It appeared as a small peritoneal recess situated towards the upper left side of the 4th part of duodenum and opened downwards. On the anterior aspect, it was bounded by a cresenteric superior duodenal fold, which had a free margin. On the posterior aspect, the other margins of the fold fused with parietal peritoneum [Table/Fig-1,2].
Superior duodenal recess. Intestines are retracted and a forceps is introduced into the recess. the incidence is 42.3%.
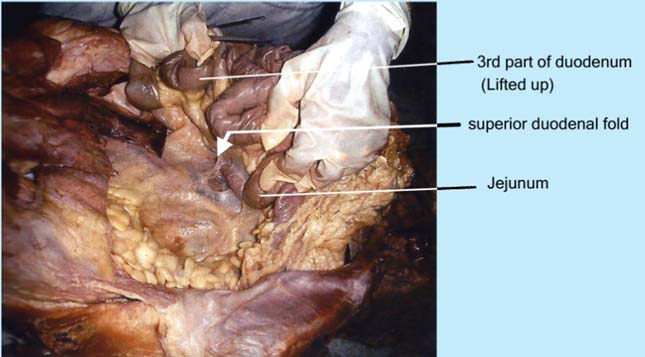
Superior duodenal recess. The recess is guarded by superior dodenal fold (arrow).
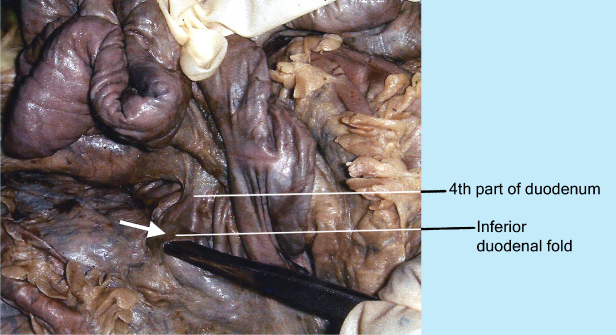
Inferior Duodenal Recess (IDR) was noted in 50 cases and was situated on the left of the 4th part of duodenum below duodenojejunal flexure. It was bounded by inferior duodenal fold in front, which was cresenteric. The fold had a free upper margin. The recess communicated with rest of peritoneal cavity by an opening which was directed upwards [Table/Fig-3,4].
Photograph showing inferior duodenal recess. Probe is introduced into the recess. the incidence. is 62%.
Inferior duodenal recess. It is guarded by inferior duodenal fold (arrow).
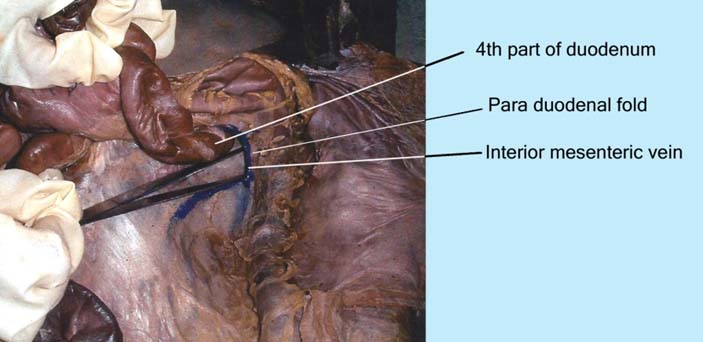
Para Duodenal Recess (PDR) was present in 3 cases out of 80. It was seen on the left side of the 4th part of duodenum. It was bounded in front by the vascular paraduodenal fold which had a right free margin. The opening of the recess was to the right [Table/Fig-5,6].
Para dodenal recess - a view from above. It is guarded by the praduodenal fold which contains the inferior mesenteric vein (blue).
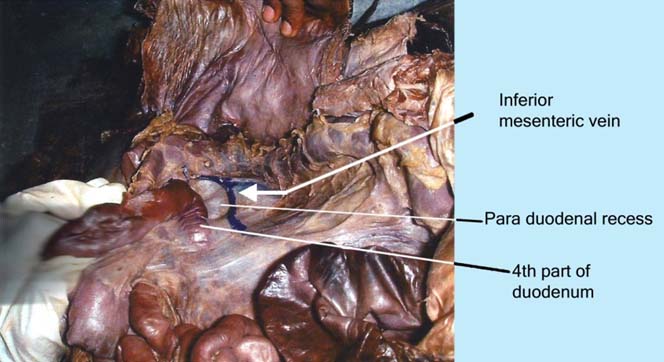
Photograph showing para duodenal recess. A probe is introduced into the depth of the recess. Incidence is 3%.
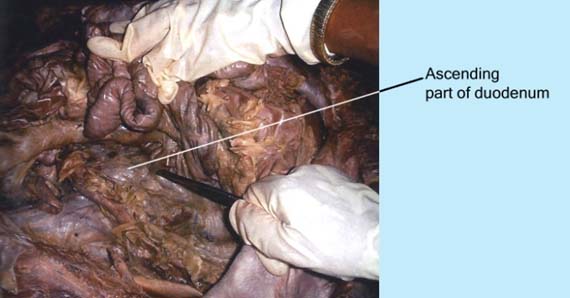
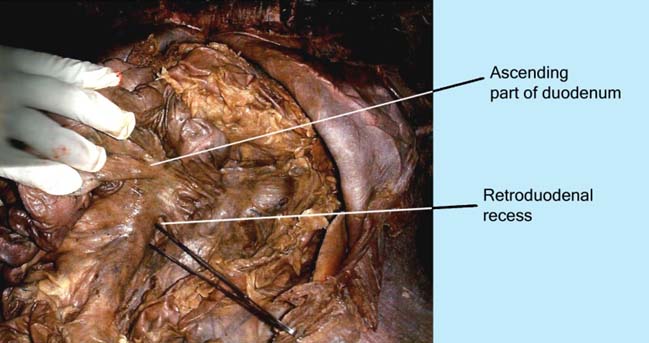
Retro Duodenal Recess (RDR) was observed in 2 cases, was situated behind the 3rd & 4th parts of duodenum. On its sides it was bounded by duodenoparietal folds. The recess was closed above and opened by an orifice which was directed downwards and to the left. Behind this recess lied the abdominal aorta [Table/Fig-7,8].
Retroduodenal recess. A probe is introduced into the depth of recess. the nicidence is 3%.

Retroduodenal recess. Jejunum and duodenojejunal flexure is lifted upwards.
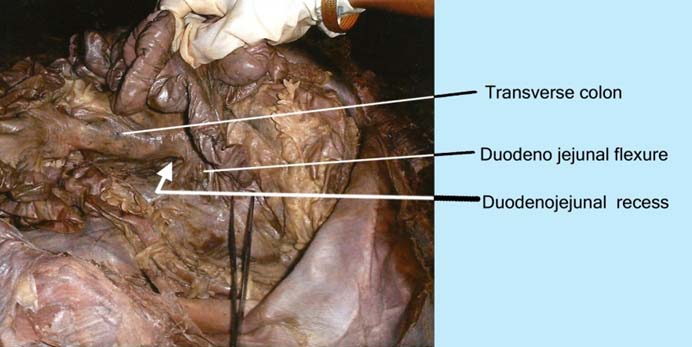
Duodeno Jejunal Recess (DJR) was seen in 15 cases. It was situated between the duodenojejunal flexure and root of transverse mesocolon, hence also known as mesocolic recess. It was bounded above by the pancreas, to the left side – by left kidney and below by renal vein. Its opening was directed downwards and to the right [Table/Fig-9,10].
Demonstration of duodenoejunal recess. A probe is introduced into the recess. Incidence is 19%.
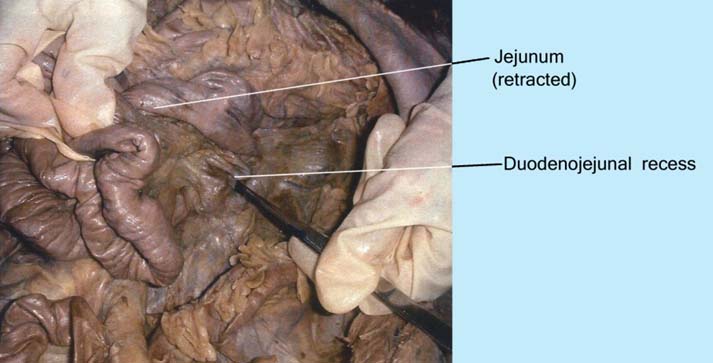
Photograph showing duodeno-jejunal flexure.
Mesentrico- Parietal Recess (MPR)- No mesentrico parietal recesses were seen in the cases studied.
Discussion
The inferior duodenal recesses were the commonly seen recess in the specimens [1]. Trieves also found the presence of inferior duodenal recess in 70-75% of individuals [2]. In the present study, the incidence of presence of inferior duodenal recesses is 62.5%. This finding almost coincides with his findings.
Superior duodenal recess is situated on the left side of the fourth part of duodenum bounded in front by superior duodenal fold. There is a presence of superior duodenal recess in 40-50% of individuals [3,4]. In the study, the presence of superior duodenal recess was 42.5%.
Para-duodenal recess is situated on the left side of the fourth part of duodenum and is bounded in front by the para duodenal fold with a right free margin which contains the inferior mesenteric vein and an ascending branch of the left colic artery. Occurrence of para duodenal recess is around is 2% [5]. In the present study, the occurrence of para-duodenal recess was 3.8%, which partly coincides with the above findings.
Retro duodenal recess is situated behind the third and fourth part of duodenum. It is bound at the side by the duodenoparietal folds. Occurrence of retro duodenal recess is rare [6]. In the present study, 2.5% of retro duodenal recesses were found.
Duodenojejunal recess is situated between the duodenojejunal flexure and root of transverse mesocolon. Occurrence of duodenojejunal recess is 20% [6]. In the present study the incidence of duodenojejunal recess was 18.8%.
Mesenterico parietal recess is situated below the third part of the duodenum and behind the upper part of the mesentery and is guarded by a fold of the mesentery raised by superior mesenteric artery. The occurrence of mesenterico parietal recess is 1% [5]. In the present study, no mesenterico-parietal recess was observed [Table/Fig-11].
Percentage of various duodenal recesses.
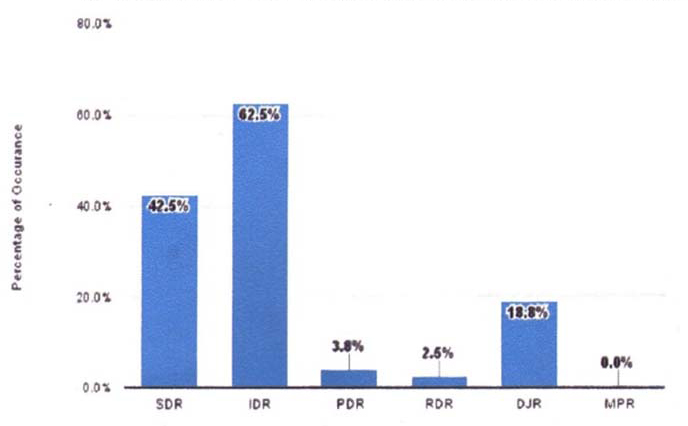
In the present study, the incidence of inferior duodenal recess was the highest (62.5%) followed by superior duodenal recess (42.5%). Duodenojejunal recess was observed in 18.8% of specimens, para duodenal recess in 3.8% and retro duodenal recess in 2.5% of cases.
Conclusion
The present study was conducted to find out the occurance of peritoneal recesses in human duodenum in different age groups. According to this most frequently occurring recess was inferior duodenal followed by superior. Paraduodenal and retroduodenal recesses were less frequent and mesenterico-parietal was not found. The present study gives adequate knowledge for surgeons to deal with internal herniation of intestinal loops.
[1]. Treitz W, About a new muscle on duodenum of people, about elastic tendon, and some other anatomical structuresVrtljschr. f. d. prakt. Heilk 1857 37:113 [Google Scholar]
[2]. Trieves F, Lectures on the anatomy of the intestinal canal and peritoneum in man: Lecture 1Brit M J 1885 (1):415 [Google Scholar]
[3]. Moynihan BGA, Retro peritoneal Hernia 1906 2nd EditionLondonBailliere, Tinclall and Cox [Google Scholar]
[4]. Chakraborty VC, Chakraborty D, Fundamentals of human anatomy New Central Book Agency (P) Limited 2001 [Google Scholar]
[5]. Ranganathan S, Text book of human anatomy 2000 1st editionS Chand [Google Scholar]
[6]. Williams PL, Bannister LH, Berry MM, Collins P, Dyson M, Dussek JE, Gray’s Anatomy 1995 38th. EdEdinburghChurchill Livingstone:1266-1274. [Google Scholar]