Endodontic Management of a Mandibular First Molar with Radix Entomolaris and Conservative Post-endodontic Restoration with CAD/CAM Onlay: A Novel Clinical Technique
Kanika Yadav1, Ida De Noronha De Ataide2, Marina Fernandes3, Rajan Lambor4, Dalip Alreja5
1 Postgraduate Student, Department of Conservative Dentistry and Endodontics, Goa Dental College and Hospital, Goa, India.
2 Professor and Head, Department of Conservative Dentistry and Endodontics, Goa Dental College and Hospital, Goa, India.
3 Assistant Professor, Department of Conservative Dentistry and Endodontics, Goa Dental College and Hospital, Goa, India.
4 Assistant Professor, Department of Conservative Dentistry and Endodontics, Goa Dental College and Hospital, Goa, India.
5 Consulting Periodontist, Department of Periodontics, Goa Dental College and Hospital, Goa, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Kanika Yadav, RZF/68-A, Street No. 3, Mahavir Enclave, New Delhi-110045, India.
E-mail: kanikay771@gmail.com
This case report describes a novel technique of restoring endodontically treated teeth. Hidden caries causing irreversible pulpitis in a mandibular molar with Radix Entomolaris (RE) was evident. The intact occlusal surface anatomy was duplicated before preparing an access cavity to replicate the original occlusal surface in the post endodontic restoration using (Computer-Aided Design and Computer-Aided Manufacturing) CAD/CAM technique. This report highlights uniquely designed onlay utilizing the benefits of contemporary materials and advanced technology.
Fiber reinforced composite, Hidden caries, Occlusal template
Case Report
A 35-year-old male patient reported to the Department of Conservative Dentistry and Endodontics with spontaneous pain in the region of mandibular right first molar. Patient’s medical history was non-contributory. Clinical examination revealed discolored disto-occlusal surface of tooth #46 with intact occlusal anatomy [Table/Fig-1a]. Tooth was tender to percussion and gave lingering response to thermal tests and electric pulp test. Pre-operative radiograph showed disto-proximal radiolucency involving the pulp and an additional disto-lingual root, Radix Entomolaris (RE) [Table/Fig-1b]. Based on clinical and radiographic findings, a diagnosis of symptomatic irreversible pulpitis and apical periodontitis was made. Treatment plan comprised of duplicating the intact occlusal surface before preparing an access cavity to replicate the natural tooth anatomy in the final restoration. It was decided to reinforce the remaining tooth structure and to form a flat base in the prepared access cavity with fiber reinforced composite, followed by CAD-CAM metal onlay restoration. Various steps in the treatment proc-edure were as follows:
(a) Pre-operative photograph showing intact occlusal surface of tooth #46; (b) Pre-operative radiograph; (c) Pre-operative cast with duplicated intact occlusal surface of tooth #46.
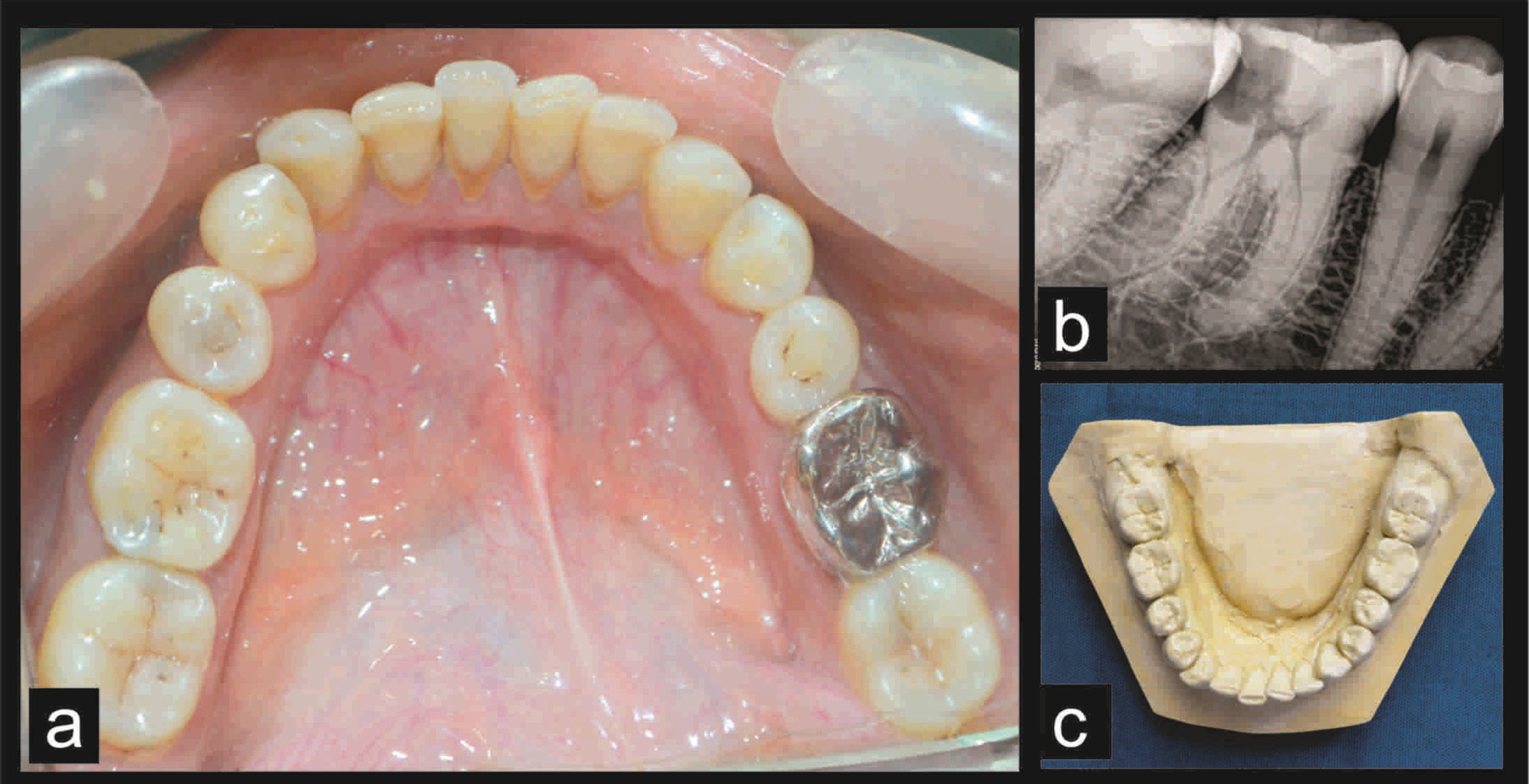
Duplicating the intact occlusal surface: Polyvinyl siloxane elastomeric impression (Aquasil soft putty/regular set and light body Dentsply, Mannheim Germany) of the lower arch was made to record the occlusal anatomy of tooth #46. Impression was made by double step putty wash technique to incorporate occlusal surface details in light body. Impression was poured in dental stone to obtain a cast with the duplicated occlusal surface of the tooth [Table/Fig-1c].
Management of radix entomolaris: Endodontic access cavity in tooth #46 was prepared under rubber dam isolation and profound anesthesia. The access cavity was modified from a triangular outline form to a trapezoidal form to locate the disto-lingual canal [Table/Fig-2a]. Working length of all four canals viz. mesio-buccal, mesio-lingual, disto-buccal and disto-lingual canal was determined using an apex locator (Propex II, Dentsply Maillefer) and confirmed radiographically [Table/Fig-2b]. The curved and narrow disto-lingual canal was first negotiated with small and flexible hand K-files and gradually enlarged to ISO size 15. Further cleaning and shaping was performed with ProTaper nickel-titanium rotary file system (Dentsply, Maillefer) in a crown-down fashion up to F1 in mesial canals and F2 in distal canals. Copious irrigation was performed with 5% sodium hypochlorite solution (Asian Acrylates, Mumbai), 17% EDTA (Glyde, Dentsply Maillefer) and final flush with sterile saline solution. Canals were dried with sterile paper points and fit of the master cone was verified radiographically. Obturation was done with ProTaper gutta percha cones (Dentsply, Maillefer) and AH Plus resin sealer (Dentsply DeTrey, Konstanz, Germany) [Table/Fig-2c].
(a) Access opening showing four root canal orifices; (b) Working length radiograph; (c) Post-obturation photograph; (d) Fiber reinforced composite placement in the access cavity; (e) Flat floor and axial wall of fiber reinforced composite; (f) Crown lengthening; (g) Onlay preparation.
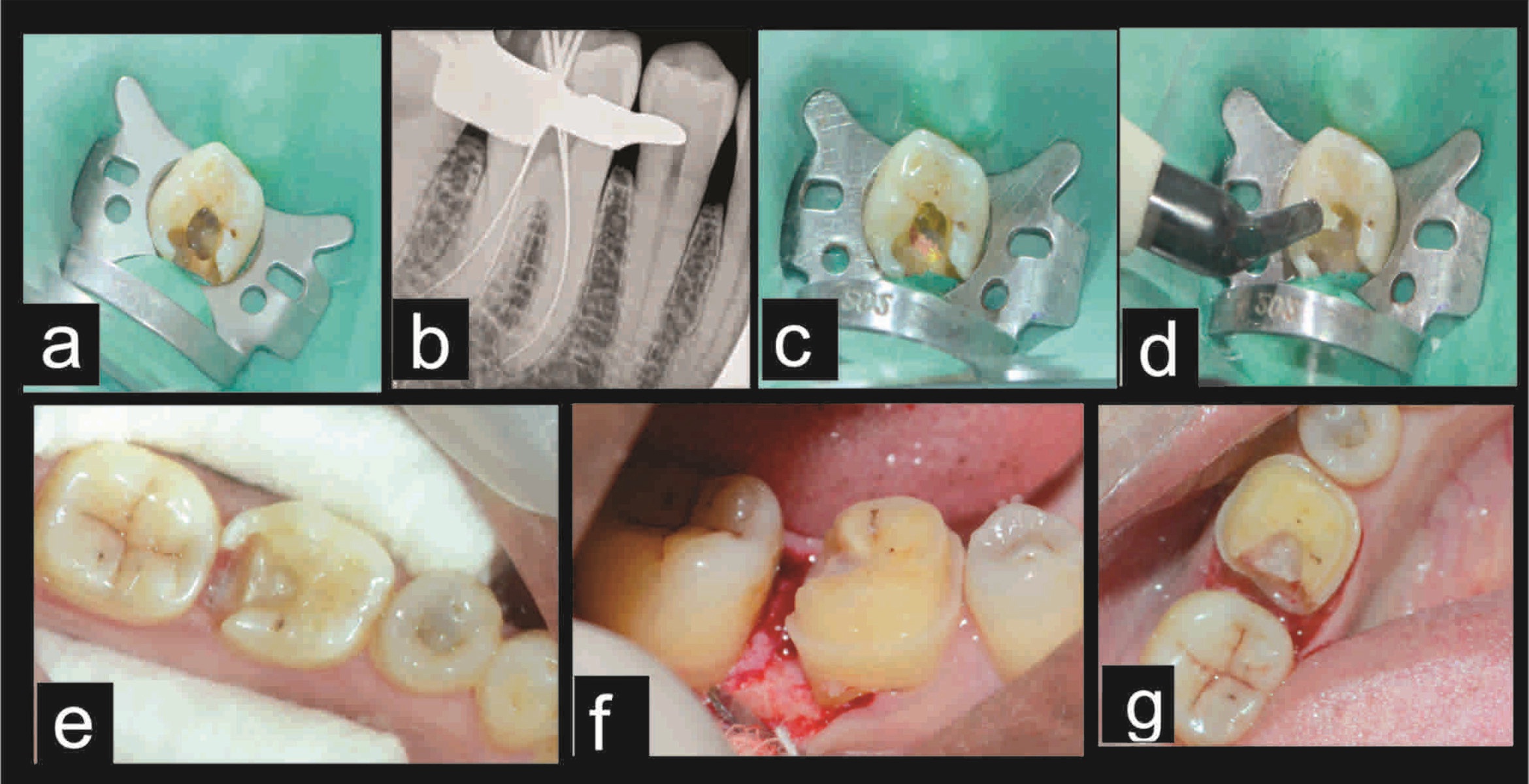
Fiber reinforced composite restoration: Following obturation, access cavity was cleaned to remove residual sealer and debris from the walls. Access cavity was etched with 37% phosphoric acid (Conditioner 36, Dentsply DeTrey) for 15 seconds and rinsed with distilled water. Cavity was blot dried and total etch adhesive (Prime and Bond NT, Dentsply Caulk, Milford, DE, USA) was applied with an applicator tip. Excess primer was removed with a gentle air stream and light cured for 20 seconds with a halogen curing light (Woodpecker LED Curing Light; Gulin Woodpecker Medical Instrument Co., Ltd., Guangxi, China). Access cavity was filled up to 4mm with fiber reinforced composite (Ever X Posterior, GC Dental Products Corp., Aichi, Japan), leaving the proximal part of the cavity and light cured for 40 seconds [Table/Fig-2d]. Therefore, endodontic access cavity was transformed to a Class II cavity with pulpal floor and axial wall in fiber reinforced composite [Table/Fig-2e].
Tooth preparation for metal onlay and impression making: Gingivectomy and crown lengthening was done on the distal surface of the tooth to get preparation margin on the sound tooth structure without compromising the biological width [Table/Fig-2f]. Tooth was prepared for a Class II metal onlay and tooth collar was prepared with no. 271 carbide bur (SS white, Fleet Street, London) for auxiliary retention [Table/Fig-2g]. Tooth was temporized and patient was recalled after 3 weeks. On recall visit, soft tissue and hard tissue healing was within normal limits. Impressions of both the arches were made and sent to the laboratory along with the cast with duplicated occlusal anatomy for the fabrication of CAD/CAM based metal onlay (Ceramill Sintron).
CAD/CAM metal onlay fabrication and cementation: In laboratory, patient’s cast with intact occlusal anatomy and onlay preparation was scanned with a 3-dimensional scanner (Amann Girrbach GMBH, Pforzheim, Germany) and the processed data was superimposed on the preparation [Table/Fig-3a,b]. A digital 3-D model of onlay was designed and input was send to the milling machine [Table/Fig-3c]. A Co-Cr metal alloy (Sintron, Amann Girrbach GMBH, Pforzheim, Germany) was milled to fabricate the onlay. The Ceramill Sintron onlay was dense-sintered with the Ceramill Therm to obtain the final density and excellent material properties [Table/Fig-3d].
(a) Digital scanning of the tooth preparation; (b) Superimposition of the processed data on the tooth preparation; (c) Digital 3D model of onlay; (d) Post-operative occlusal view; (e) Post-operative radiograph; (f) Follow-up occlusal view; (g) Follow-up radiograph.
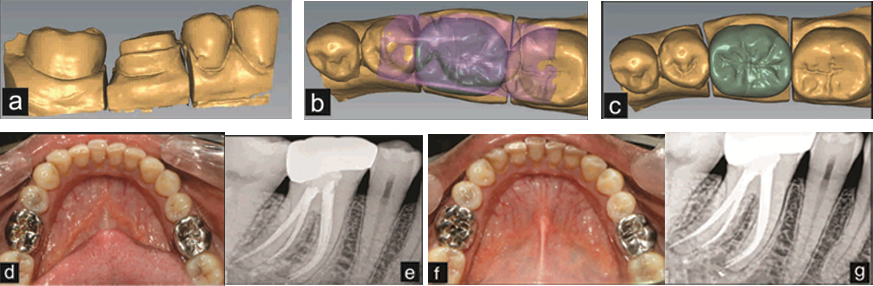
In the next treatment visit, metal onlay was cemented using glass ionomer cement (GC Luting and Lining Cement, GC America Inc.) according to manufacturer’s recommendations [Table/Fig-3e]. A 15 months follow-up showed hard tissue and soft tissues within normal limit with no clinical sign and symptom [Table/Fig-3f,g].
Discussion
Hidden caries are also one of the various aetiologies causing pulpal involvement and tooth structure loss. ‘Hidden caries’ is a term used to describe carious lesion seen in dentine on a radiograph, where clinically the occlusal enamel appears sound or only minimally demineralized [1]. These lesions present challenges in diagnosis and treatment planning, but have an advantage of intact occlusal surface which can be duplicated pre-operatively to replicate it in the final restoration [2].
Successful root canal treatment is dependent on thorough clean-sing, shaping and obturation of the entire root canal system including anatomical variations. RE is the anatomical variant found most commonly in a permanent mandibular molar and characterized by the presence of an additional third root, disto-lingually. The prevalence of RE ranges from 0-33.1% [3]. Management of such cases are challenging as majority of RE are curved and have variable furcation level which may lead to iatrogenic errors in the form of furcal or strip perforation, canal transportation, vertical root fracture, ledge formation, and instrument separation [4]. Conventional triangular access opening in such cases is modified to a trapezoidal or rectangular form to locate disto-lingual canal orifice of the additional root which may additionally weaken the tooth structure [5]. Therefore, restorative needs of such cases should be given special attention to preserve the remaining tooth structure.
The restorative needs of the posterior teeth are different from that of anteriors because of variability in the magnitude and direction of forces acting on the molars. Long-term retention of the endodontically treated teeth and resistance to fracturing are directly related to the amount of residual tooth structure [6]. Preservation of Pericervical Dentine (PCD) is of utmost importance in endodontically treated teeth. PCD is a critical zone, 4mm above the crestal bone and extending 4mm apical to the crest. Preservation of pericervical dentine provides optimum strength and fracture resistance to endodontically treated teeth [7]. Although bonded restoration is the most conservative treatment option, it is unacceptable for endodontically treated teeth with lost marginal ridge [8]. If the cuspal width to length ratio of the tooth is more than 1:2, an onlay can be placed as the partial coverage restorations preserves more tooth structure than full coverage crowns and provides sufficient fracture to resistance as compared to direct bonded restorations [9]. In this case report, post-endodontic restoration was done with metal onlay instead of full coverage crown to preserve the sound tooth structure.
Ever-X posterior (GC Dental Products Corp.) is a Fiber Reinforced Composite (FRC) in which silanated short E-glass fibers are incorporated to improve the flexural strength and fracture toughness of the restoration. Fiber reinforcement reduces polymerization shrinkage and improves the mechanical properties of composites [10]. In this case, FRC was used not only to reinforce weakened tooth structure but also to block out undercuts in the access cavity by forming a base of FRC. It transformed an access cavity to a Class II cavity which was prepared for an onlay conventionally. It enhanced the ease of impression making and onlay cementation by forming a flat base in FRC and blocking out the undercuts.
CAD/CAM based restoration was selected for this case to replicate patient’s original tooth anatomy in the final restoration by scanning the pre-operative cast of the patient. Moreover, digital scanning and designing results in more accurate marginal adaptation than conventional casting procedure [11]. Thus, patient’s original tooth form, contact and contour are restored in the milled restoration without much need of adjusting the restoration in patient’s mouth. This reduces the chair side time, restores the natural tooth anatomy and provides a restoration with better marginal fit and accuracy. Metal restoration was chosen over the ceramic restoration due to low cost, aesthetically non-critical area and presence of metal restoration on contralateral tooth. To the best of our knowledge, this is the first case report of CAD/CAM based non-precious metal restoration.
This technique combined the benefits of contemporary materials (FRC) and recent technology (CAD/CAM) to replicate original tooth form and anatomy. This technique offers various advantages such as less chair side time in adjusting the restoration, no occlusal interference, better fit of the restoration, reinforcement of the tooth structure and supragingival margin preserving the periodontal health. Also, the restoration is more conservative and less expensive than full coverage restorations.
Conclusion
Therefore, endodontic cases of hidden caries spreading beneath an intact enamel surface can be managed conservatively using the occlusal template, fiber reinforced composite and CAD/CAM technology.
[1]. Weerheijm KL, Occlusal ‘hidden caries’Dent Update 1997 24:182-84. [Google Scholar]
[2]. Martos J, Silveira LFM, Ferrer-Luque CM, González-López S, Restoration of posterior teeth using occlusal matrix techniqueIndian J Dent Res 2010 21:596-99. [Google Scholar]
[3]. Abella F, Patel S, Duran-Sindreu F, Mercade M, Roig M, Mandibular first molars with disto-lingual roots: Review and clinical managementInt Endod J 2012 45:963-78. [Google Scholar]
[4]. Calberson FL, de Moor RJ, Deroose CA, The radix entomolaris and paramolaris: Clinical approach in endodonticsJ Endod 2007 33:58-63. [Google Scholar]
[5]. Gu Y, Lu Q, Wang H, Ding Y, Wang P, Ni L, Root canal morphology of permanent three-rooted mandibular first molars-part I: Pulp floor and root canal systemJ Endod 2010 36:990-94. [Google Scholar]
[6]. Kutesa Mutebi A, Osman YI, Effect of the ferrule on fracture resistance of teeth restored with prefabricated posts and composite coresAfr Health Sci 2004 4:131-35. [Google Scholar]
[7]. Clark D, Khademi J, Modern molar endodontic access and directed dentine conservationDent Clin North Am 2010 54:249-73. [Google Scholar]
[8]. Tikku AP, Chandra A, Bharti R, Are full cast crowns mandatory after endodontic treatment in posterior teeth?J Conserv Dent 2010 13(4):246-48. [Google Scholar]
[9]. Marzouk MA, Simonton AL, Gross RD, Designs of cavity and tooth preparations for cast restorationsOperative Dentistry, Modern Theory and Practice 1997 1st Indian edChennaiAll India Publishers and Distributors:326 [Google Scholar]
[10]. Rocca GT, Rizcalla N, Krejci I, Fibre-reinforced resin coating for endocrown preparations: A technical reportOper Dent 2013 38:242-48. [Google Scholar]
[11]. Yildiz C, Vanlioglu B, Evren B, Uludamar A, Ozkan YK, Marginal-internal adaptation and fracture resistance of CAD/CAM crown restorationsDent Mater J 2013 32:42-47. [Google Scholar]