Anaerobic Bacteriological Microbiota in Surface and Core of Tonsils in Chronic Tonsillitis
Meera Niranjan Khadilkar1, Nitin R. Ankle2
1 Resident, Department of Ear, Nose and Throat, Jawaharlal Nehru Medical College, KLE University, Belgaum, Karnataka, India.
2 Professor, Department of Ear, Nose and Throat, Jawaharlal Nehru Medical College, KLE University, Belgaum, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Meera Niranjan Khadilkar, Department of ENT, Jawaharlal Nehru Medical College, KLE University, Belgaum – 590010, Karnataka, India.
E-mail: musicnmee@gmail.com
Introduction
Tonsillar infection may stem from bacteria within tonsillar crypts or parenchyma rather than from those on the surface. Pathogens isolated from surface culture may be colonizing the tonsil, but not essentially infecting it. Anaerobes though not often studied, are known to cause chronic tonsillitis.
Aim
To study the correlation of anaerobic bacterial isolates in surface and core cultures from recurrently infected and inflamed tonsils.
Materials and Methods
A cross-sectional study was conducted in Charitable Hospital and Medical Research Centre, Belagavi from January 2014 to December 2014 on 100 patients of chronic tonsillitis who underwent tonsillectomy. Swabs were obtained from tonsil surface and core and analysed for anaerobes as per standard protocol. Chi-square test and Fischer-Exact test were used for statistical analysis.
Results
Twenty eight out of 63 (44.4%) patients had anaerobic growth on tonsil surface and 30 out of 62 (48.4%) patients had anaerobic growth in tonsil core. Porphyromonas sp. was the most common anaerobe isolated from the surface as well as from the core. There was no statistical significance between anaerobes isolated in the tonsil surface and core.
Conclusion
Anaerobic organisms obtained from tonsil surface and core cultures were similar. A throat swab satisfactorily depicts the core organism and is reliable in recognizing the bacteriology of chronic tonsillitis. Anaerobic organisms known to inhabit the surface as well as the core of tonsils may be treated with suitable antibiotic therapy.
Bacteria, Porphyromonas, Tonsillectomy
Introduction
The tonsils are situated in areas where microorganisms are teeming, enabling the passage of organisms through areas of deficient epithelium, bearing the effect of individual attacks of tonsillitis. Thus it is very important to identify the individual pathogens causing tonsillitis, and also affecting joints, heart and kidneys, resulting in dreadful consequences [1].
Tonsillar infection may arise from bacteria within the tonsillar parenchyma or crypts rather than those on the surface, which may be colonizing the tonsil, without essentially infecting it. A possible explanation for not acquiring an accurate culture of pathogenic microorganisms is that the sole aerobic techniques are unsatisfactory. Anaerobic technique would increase the isolation of organisms, so that the most sensitive antibiotic can be administered and the cause of the recurrence identified. Moreover, the cost and procedure of tonsillectomy, the agonising post-operative pain and complications can be minimised [2].
In tonsillitis, bacteria colonise the surface as well as the core. Hence, antibiotic treatment based only on tonsil surface culture report may sometimes fail [3].
Anaerobes though not studied on a regular basis in cases of chronic tonsillitis, are recognized causative organisms in infection and recurrence of the disease.
Materials and Methods
A cross-sectional study was conducted on 100 patients of chronic tonsillitis between 5 and 52 years of age, who underwent tonsillectomy in Department of ENT, KLES Dr. Prabhakar Kore Charitable Hospital and Medical Research Centre, Belagavi, from January to December 2014, after obtaining written informed consent. There were 47 male and 53 female patients. Those with tonsillar malignancy and who failed to give consent were excluded. There was no control group.
One swab was procured from the tonsillar surface intraoperatively by rotating sterile cotton wool swabs over the surface of the tonsil, avoiding any other part of the oropharynx, before tonsillectomy. The tonsillar specimen obtained after surgery was immediately dipped into povidone iodine solution for half a minute and then rinsed in sterile saline solution. It was sectioned into two parts following thorough asepsis. Another sterile swab was applied to the inner surface of the sectioned tonsil, without touching the outer surface. The two samples were transported to the Microbiology lab in thioglycollate medium for anaerobic culture. The samples were processed as per the standard protocol [4,5]. Statistical analysis was done to determine percentage and the significance between the anaerobic isolates from surface and core of infected tonsils by application of Chi-square test and Fischer-Exact test. Institutional Ethics Committee approval was obtained.
Results
Chronic tonsillitis was most predominant (44%) in the adolescent age group (11-20 years) with a slight female predilection (53%). Indications for surgery were chronic tonsillitis in 63%, chronic adenotonsillitis in 36% and chronic adenotonsillitis with bilateral chronic otitis media in 1%. Tonsillitis was parenchymatous type in 83 (83%) and follicular type in 17 (17%) patients, with nil cases of membranous tonsillitis.
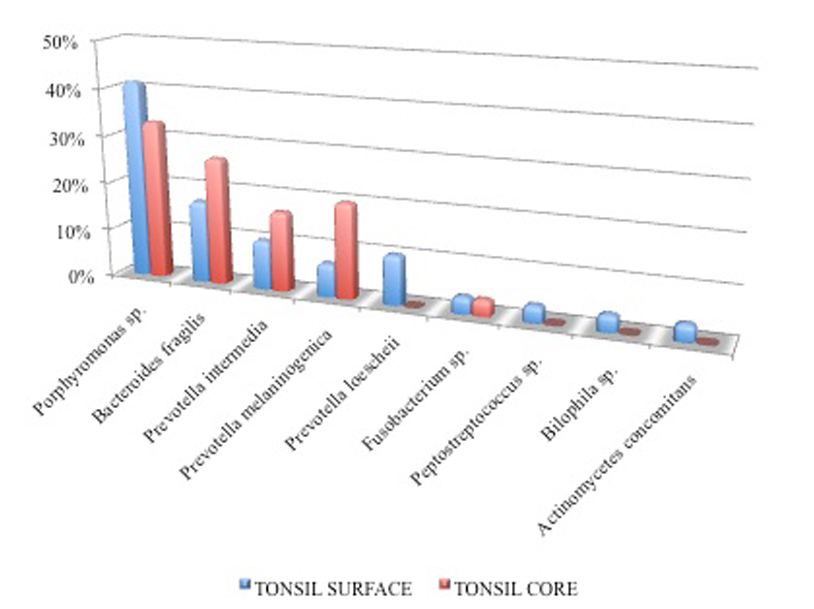
The number of patients with bacterial growth on tonsil surface and core were 63 (63%) and 62 (62%). Twenty-eight out of 63 (44.4%) and 30 out of 62 (48.4%) patients had anaerobic growth on tonsil surface and core respectively. The remaining 35 out of 63 (55.6%) and 32 out of 62 (51.6%) did not have any anaerobic growth on tonsil surface and core respectively. Twenty-two out of 36 (61.1%) patients had anaerobic growth on tonsil surface as well as in tonsil core, of which 13 patients had the same growth on tonsil surface as well as core. The remaining 14 patients (38.9%) patients had anaerobic growth in either tonsil surface or in core. One out of 28 (3.6%) patients had polymicrobial anaerobic growth on tonsil surface. No patients had polymicrobial anaerobic growth in tonsil core. The most common anaerobic bacterium isolated from tonsil surface and core was Porphyromonas sp. in 41.4% and 33.3% respectively. There was no statistically significant difference between the anaerobic bacteria in tonsil surface and core [Table/Fig-1].
Statistical analysis of anaerobes isolated on tonsil surface and tonsil core.
| Anaerobic Growth | Tonsil SurfaceNumber (%) | Tonsil CoreNumber (%) | p-value |
|---|
| Porphyromonas sp. | 12 (41.4%) | 10 (33.3%) | 0.522 |
| Bacteroides fragilis | 5 (17.2%) | 8 (26.7%) | 0.382 |
| Prevotella intermedia | 3 (10.3%) | 5 (16.7%) | 0.742 |
| Prevotella melaninogenica | 2 (6.9%) | 6 (20.0%) | 0.276 |
| Prevotella loescheii | 3 (10.3%) | 0 (0.0%) | 0.112 |
| Fusobacterium sp. | 1 (3.4%) | 1 (3.3%) | 1.00 |
| Peptostreptococcus sp. | 1 (3.4%) | 0 (0.0%) | 0.491 |
| Bilophila sp. | 1 (3.4%) | 0 (0.0%) | 0.491 |
| Actinomycetes concomitans | 1 (3.4%) | 0 (0.0%) | 0.491 |
| Total | 29 (100%) | 30 (100%) | |
Discussion
Tonsillitis most often presents in the first ten years of life and antibiotic therapy is many a time inadequate or inappropriate, leading to persistent, resistant, recurrent infection and chronicity. In our study, chronic tonsillitis was primarily seen in adolescents (44%) of 11-20 years, followed by children (41%). Age incidence was comparable to some of the previous studies [1,2,6–8]. Females (53%) were in majority in the present study, while males were 47%, male:female ratio being 1:1.12. This could be attributed to the increased health awareness in women in the last decade. On the contrary, gender incidence was higher in men as per many of the previous studies [1,6,8]. In a study by Jayasimha et al., which included 50 patients with recurrent tonsillitis, the most common age group was 11-20 years. Male: female ratio was 1:1.5 [9]. Surgical indications included chronic tonsillitis in 63%, followed by chronic adenotonsillitis in 36% and chronic adenotonsillitis with bilateral chronic otitis media in 1%. Tonsillitis was parenchymatous in nature in 83%, follicular in 23% and not a single case of membranous tonsillitis. In the current study, growth of bacteria on the surface and core of tonsils was almost equal (63% and 62% respectively). An identical incidence of surface and core isolates was observed in three studies [2,5]. A study conducted by Rekabi et al., revealed pathogenic organisms in 65% (78 of 120) patients, with 43 surface isolates and 35 core isolates [10]. Another study showed microorganisms on tonsil surface in 76.1% and in core in 79.6% patients [11]. However, three other studies observed core isolates to be nearly twice that of surface isolates [12–14]. The absence of growth in tonsil surface and core in the other patients could be justified by a probable viral etiology in causing chronic tonsillitis, which has not been analysed in our study.
Anaerobic isolates in the surface and core cultures in the present study were almost equal (44.4% & 48.4% respectively). Another study revealed anaerobic growth in 20% surface isolates and 62.5% core isolates [15]. In our study, anaerobes were isolated in 61.1% patients, in both surface and core cultures. Same isolates were seen in 59.1% in cultures from surface and core. Porphyromonas sp. was the most common anaerobe isolated in both surface and core cultures (41.4% and 33.3% respectively) in the present study. Klug et al., found Prevotella sp. and Fusobacterium sp. as the predominant anaerobes [15]. Bacteroides fragilis (17.2%), Prevotella intermedia, Prevotella loescheii (10.3% each), Prevotella melaninogenica (6.9%) were the other anaerobic isolates from surface cultures in the present study. Fusobacterium sp., Peptostreptococcus sp., Bilophila sp., Actinomycetes concomitans (3.4%) were the uncommon anaerobic bacteria isolated exclusively in surface cultures. Previous studies have almost never isolated Bilophila sp. and Actinomycetes concomitans. Taylan et al., noted that Peptostreptococcus sp. was the most common organism in tonsil core (37%) [16]. However, in our study, Peptostreptococcussp. was isolated only from the surface. [Table/Fig-2].
Comparison of findings of present study and previous studies.
| Study | Present study | Klug et al., [15] | Taylan et al., [16] |
|---|
| Anaerobic growthon tonsil surface | 44.4% | 30.4% | - |
| Anaerobic growthon tonsil core | 48.4% | 36.5% | 30.7% |
| Most commonanaerobe on tonsil surface | Porphyromonassp. | Prevotella sp. | - |
| Most commonanaerobe on tonsil core | Porphyromonassp. | Prevotella sp. | Peptostrepto-coccus sp. |
The core cultures also isolated Bacteroides fragilis (26.7%), Prevotella melaninogenica (20.0%) [Table/Fig-3], Prevotella intermedia (16.7%) and Fusobacterium sp. (3.3%) [Table/Fig-4]. There was no statistically significant difference (p-value > 0.05) between the anaerobic bacteria found in tonsil surface and core. Polymicrobial anaerobic isolates were cultured in 3.65% surface cultures, whereas there was no polymicrobial anaerobic flora isolated from core culture.
Growth of Prevotella melaninogenica and Bacteroides fragilis.
Comparison of anaerobes isolated on tonsil surface and tonsil core.
Limitation
The authors recommend additional studies to assess the likely role of viral organisms and host factors like socio-economic status, malnutrition and poor oral hygiene in a larger population and over wider geographical areas.
Conclusion
Surface and core anaerobic cultures of tonsils are equally comparable. This could possibly be due to the fact that the swabs were obtained under ideal conditions that included transporting swabs with sterile precautions within one hour of tonsillectomy. Hence, a throat swab adequately represents the core pathogen, and is dependable in detecting the anaerobic bacteriology of chronic tonsillitis and specific antibiotic treatment can be administered based on surface anaerobe culture report.
[1]. Agrawal A, Kumar D, Goyal A, Gupta R, Bhooshan S, Bacteriological evaluation and their antibiotic sensitivity pattern in tonsillitisIOSR J Dental Med Sc 2014 13(3):51-55. [Google Scholar]
[2]. Bista M, Sinha BK, Amatya RCM, Tuladhar NR, Pokharel BM, Comparison of core and surface cultures in recurrent tonsillitisJ Institute Med 2005 27:60-65. [Google Scholar]
[3]. Panga A, Rani GU, Kumar MV, Chronic Tonsillitis: A comparative study of the causative organism cultured through throat swab vs. core culture and biopsy of the tonsillectomy specimenInt J Sc Research 2013 5(4):1390-95. [Google Scholar]
[4]. Collee JG, Fraser AG, Marmion BP, Simmons A, Mackie & McCartney Practical Medical Microbiology 1996 14th edNew YorkChurchill Livingstone [Google Scholar]
[5]. Sutter VL, Citron DM, Edelstein M, Finegold SM, Wadsworth anaerobic bacteriology manual 1985 4th edCaliforniaStar Publishing Company [Google Scholar]
[6]. Babu B, Reynolds AM, A study to find out the bacteriology of tonsillar surface and core, among Patients undergoing tonsillectomy at a tertiary care hospital in south IndiaJ Evid Based Med Healthc 2016 3(43):2131-34. [Google Scholar]
[7]. Samaddar S, Mukherjee D, Nandi A, Mandal SS, Roy N, Sanyal S, Recurrent Acute Tonsillitis - The ‘Core’ IssueBengal J Otolaryngol Head Neck Surg 2016 24(1):1-6. [Google Scholar]
[8]. Gul M, Okur E, Ciragil P, Yildirim E, Aral M, Kilic MA, The comparison of tonsillar surface and core cultures in recurrent tonsillitisAmerican J Otol 2007 28(3):173-76. [Google Scholar]
[9]. Jayasimha VL, Vinodkumar CS, Raghukumar KG, Basavarajappa KG, Surface Tonsillar bacteria versus deep tonsillar bacteria in tonsillitisJ Pub Health Med Res 2013 1(2):92-94. [Google Scholar]
[10]. Rekabi H, Khosravi AD, Ahmadi K, Kardouni M, The microbiologic comparison of the surface and deep tissue tonsillar cultures in patients underwent tonsillectomyJ Med Sciences 2008 8:325-28. [Google Scholar]
[11]. Shishegar M, Ashraf MJ, Post-tonsillectomy bacteremia and comparison of tonsillar surface and deep cultureAdv in Prev Med 2014 :1-5. [Google Scholar]
[12]. Pereira LMP, Juman S, Bekele I, Seepersadsingh N, Adesiyun AA, Selected bacterial recovery in Trinidadian children with chronic tonsillar diseaseRev Bras Otorrinolaringol 2008 74(6):903-11. [Google Scholar]
[13]. Al-Roosan M, Al-Khtoum N, Al-Said H, Correlation between surface swab culture and tonsillar core culture in patients with recurrent tonsillitisKhartoum Medi J 2008 1(3):129-32. [Google Scholar]
[14]. Yousef RY, Faza’a SA, Yousef RY, Comparison of the bacteriology of tonsil surface and core in bacterial profile isolated from children with chronic tonsillitisMed J Babylon 2014 7(1):52-57. [Google Scholar]
[15]. Klug TE, Henriksen JJ, Fuursted K, Ovesen T, Similar recovery rates of Fusobacterium necrophorum from recurrently infected and non-infected tonsilsDan Med Bul 2011 58(7):1-5. [Google Scholar]
[16]. Taylan I, Ozcan I, Mumcuoglu I, Baran I, Ozcan KM, Akdogan O, Comparison of the surface and core bacteria in tonsillar and adenoid tissue with beta-lactamase productionInd J Otolaryngol Head Neck Surg 2011 63(3):223-28. [Google Scholar]