An Atypical Presentation of Multiple Central Osteomas Mimicking Craniofacial Fibrous Dysplasia – A Pictorial Essay
Rashmi Kewal Agarwal1, Amit A Mhapuskar2, Manjula Hebbale3, Meenal Tepan4, Ayushee5
1 Ex-Postgraduate Student, Department of Oral Medicine and Radiology, Bharati Vidyapeeth Deemed University Dental College and Hospital, Pune, Maharashtra, India.
2 Professor and Head, Department of Oral Medicine and Radiology, Bharati Vidyapeeth Deemed University Dental College and Hospital, Pune, Maharashtra, India.
3 Reader, Department of Oral Medicine and Radiology, Bharati Vidyapeeth Deemed University Dental College and Hospital, Pune, Maharashtra, India.
4 Assistant Professor, Department of Oral Medicine and Radiology, Bharati Vidyapeeth Deemed University Dental College and Hospital, Pune, Maharashtra, India.
5 Postgraduate Student, Department of Oral Medicine and Radiology, Bharati Vidyapeeth Deemed University Dental College and Hospital, Pune, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rashmi Kewal Agarwal, A 104, Shree Shanta Durga Complex, Ramkrishna Nagar, Palghar– 401404, Maharashtra, India.
E-mail: dr.agarwal.rashmi@gmail.com
Osteoma is benign neoplasm with slow growth characterized by deposition of compact lamellar cortical or cancellous bone creating a tumour mass. It is still unclear whether osteomas are benign neoplasms or hamartomas. They have typical clinical presentations and are easily diagnosed with the help of radiographs. We present a rare case of non-syndromic multiple osteomas in the craniofacial region which are typically restricted to the midline and presents radiographically as craniofacial fibrous dysplasia causing a diagnostic dilemma.
Clinico-radio-pathologic correlation, Multiple radiopacities, Multicentric, Unilateral
Case Report
A 32-year-old female patient visited the department of Oral Medicine and Radiology, with a chief complaint of multiple hard growths on the right side of the face and in the oral cavity from past 18 years. The growths had started appearing when she was 14 years of age and gradually increased in size to the present size when she was 20 years old. After that the growths remained unchanged. Since that time her hearing ability from the right ear had gradually diminished. She also complained of mild pain in the head, the ear and the jaw when she performed movements such as yawning, eating etc., since then. Extraoral examination showed marked asymmetry of the face with multiple bony hard nodules in the temporal and parietal region of the cranium, malar process, temporomadibular joint region and the mandible [Table/Fig-1]. She had a reduced mouth opening and right side temporomandibular joint was not palpable on functional movements. Intraoral examination showed tori like growths on the right maxillary alveolus, hard palate and buccal and lingual mandibular alveolus and also fusiform enlargement of the right maxilla and mandible [Table/Fig-2]. All the features were strictly restricted to the midline. A provisional diagnoses of multiple osteomas and a differential diagnoses of craniofacial fibrous dysplasia and Gardner’s syndrome were made. The radiographic investigations advised were Orthopantomograph, Posterior to anterior skull, P.A. Waters, lateral cephalogram and Reverse Towne’s projections [Table/Fig-3]. All the radiographs showed multiple well defined ovoid radiopacities in the right cranium, orbit, malar region, maxilla, mandible, nasal bone and temporomandibular joint giving a cotton wool appearance. As these radiographs could not delineate the complete extent of the involvement; so, Computed Tomography (CT) was advised. The CT showed large expansile predominantly sclerotic lesion exhibiting ground glass to dense matrix involving the right half of skull base, temporoparietal bones, maxilla, zygomatic bone, and arch, mandible, pterygoid plate, right sphenoid and clivus and right temporomandibular joint. Significant encroachment was seen on the right maxillary sinus, sphenoid sinus, right external auditory canal, middle ear cavity, mastoid air cells and orbital apex. Near complete obliteration of foramen ovale, rotundum and spinosum and narrowing of the right superior orbital fissure was also seen [Table/Fig-4]. No neurologic signs and symptoms were associated with this. Soft tissue window showed mild proptosis of the right eye. Additional radiographs of the long bones of the body were made which appeared normal. A radiographic diagnosis of a fibroosseous lesion most likely to be fibrous dysplasia was made. The 3D reconstructed images showed the massiveness of the lesion [Table/Fig-5]. Ultrasonography of the intestine and colonoscopy was performed which appeared normal. Serum calcium and alkaline phosphatase levels were also in the normal ranges. An excisional biopsy of the torus present in the mandible and maxilla was performed under general anesthesia with the patient’s consent and sent for histopathological evaluation. The histopathology showed lamellar bone without any fibrous component; thus, giving the diagnosis of multiple osteomas [Table/Fig-6]. The patient is now being managed under a multidisciplinary approach including various specialists.
Profile pictures (frontal and lateral) show the facial asymmetry and lobulated overgrowths in the malar region, temporal region and the mandibular region.

Intraoral pictures showing maxillary fusiform enlargement and mandibular torus.

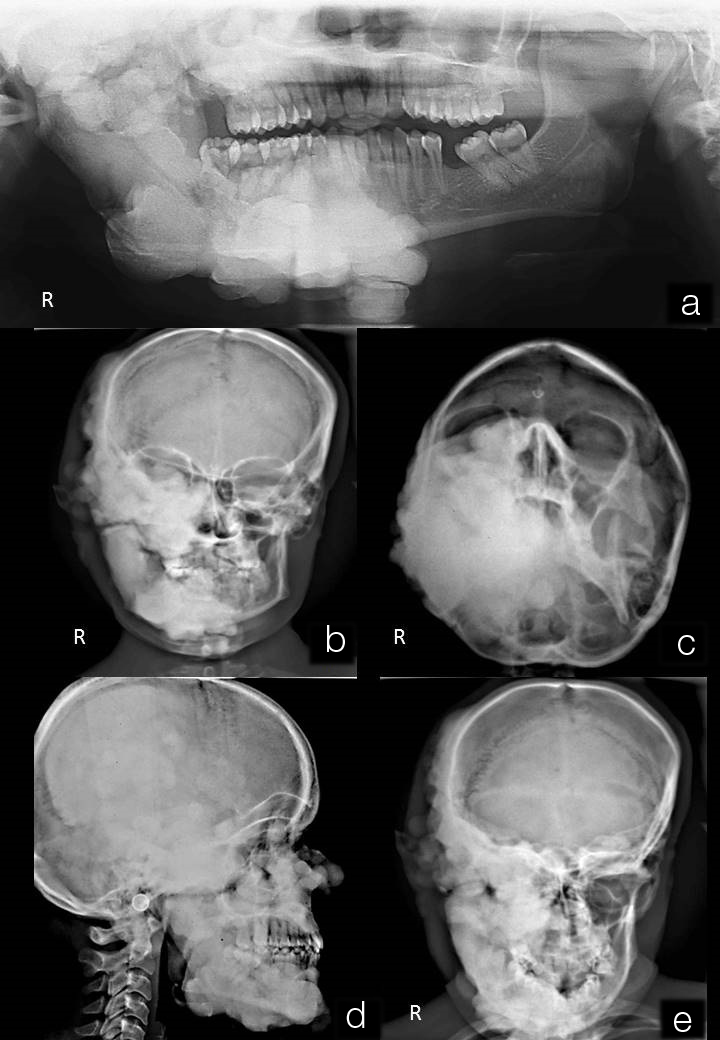
a) Orthopantomograph showing well defined multiple radiopacities giving a cotton wool appearance involving the right maxilla, maxillary sinus, temporomandibular joint and mandible; b) P.A cephalogram shows similar radiopacities in the right temporal region, parietal region, floor of the orbit, lateral nasal wall, zygomatic bone, maxilla and the condyle, ramus and body of the mandible; c) P.A Water’s projection shows the complete obliteration of the right maxillary sinus; d) Lateral cephalogram shows well defined multiple radiopacities in the temporal bone, parietal bone, nasal bone, zygomatic bone, maxilla and the mandible; e) Reverse Towne’s projection shows the involvement of the right glenoid fossa, condylar head, ramus and body of the mandible.
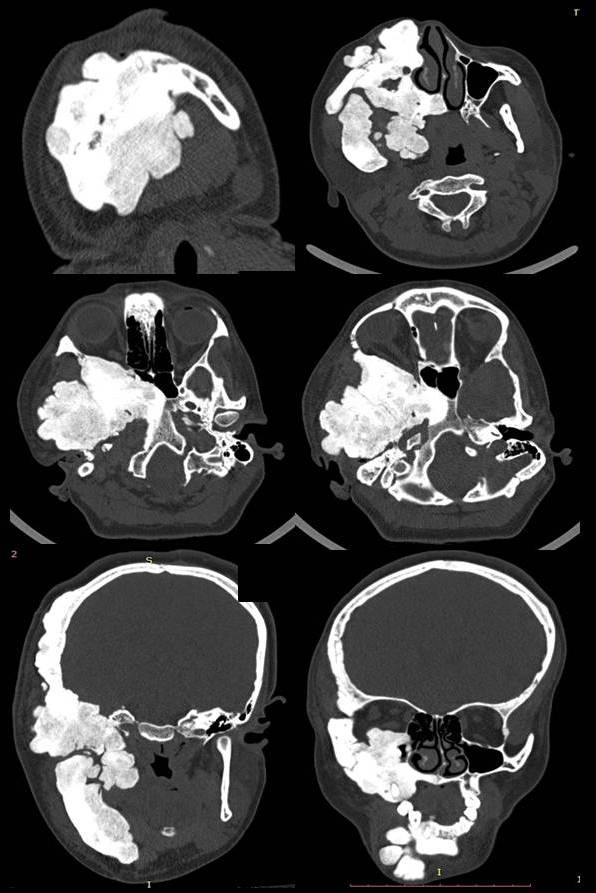
Axial and coronal sections of computed tomography show large expansile predominantly sclerotic lesion exhibiting ground glass to dense matrix involving the right half of skull base, temporoparietal bones, maxilla, zygomatic bone, and arch, mandible, pterygoid plate, right sphenoid and clivus, mastoid and right temporomandibular joint, significant encroachment is seen on the right maxillary sinus, sphenoid sinus, right external auditory canal, middle ear cavity, mastoid air cells and orbital apex and near complete obliteration of foramen ovale, rotundum and spinosum.
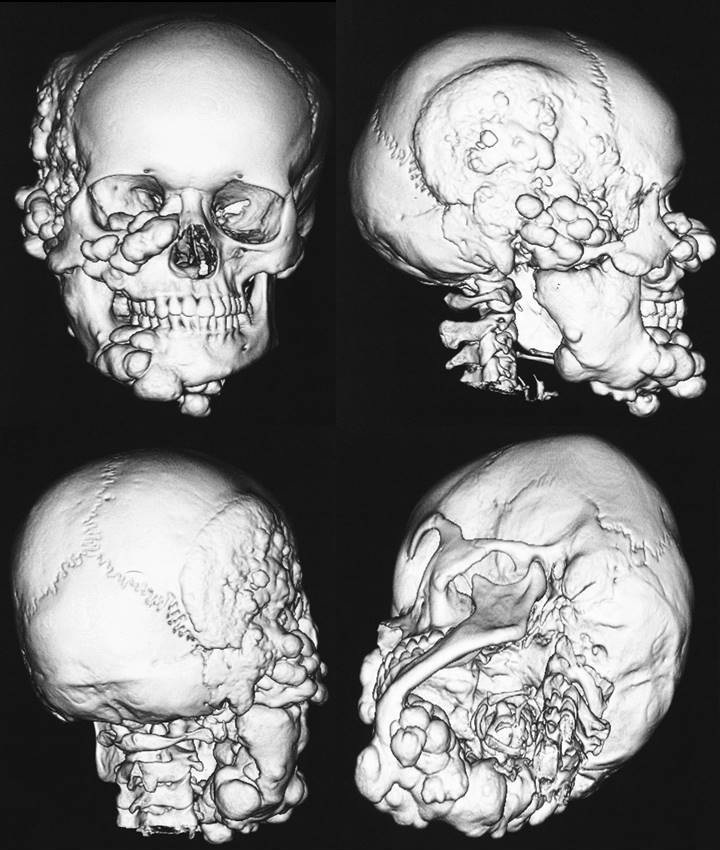
3D reonstructions of the CT images showing the massive involvement.
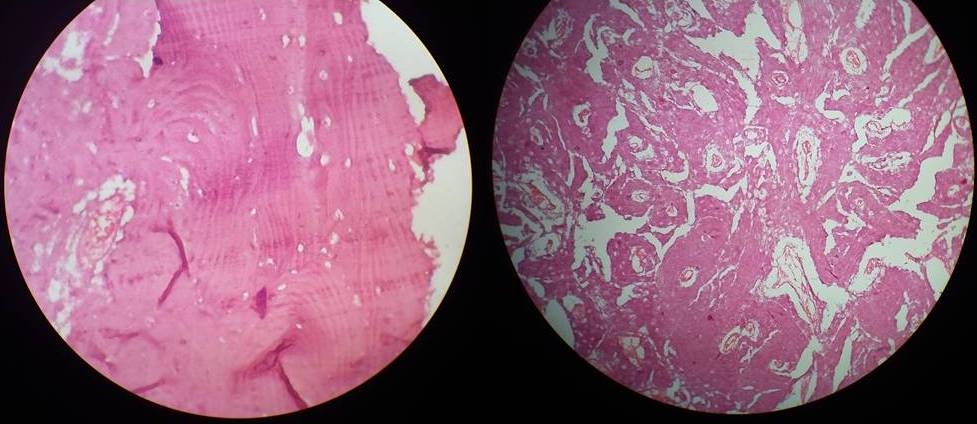
Histopathology showing lamellar bone.
Discussion
Osteoma is an osteogenic lesion characterized by slow growth and proliferation of compact or cancellous bone and is almost exclusively found in the head and neck area [1]. The majority of cases occur in the craniofacial skeleton, most frequently in the paranasal sinuses and the jawbones, and rarely in the cranial vault [2]. Temporal osteomas are more common in the females and rarely occur before puberty; whereas, the osteomas of the middle ear are more common in the males [3]. The case presented here showed the involvement of the temporal bone, mastoid, middle ear, zygomatic bone, sphenoid, maxilla and mandible. It can be of central, peripheral or extra-skeletal variety. The central form arises from the endosteum and the peripheral form arises from the periosteum; whereas, the extraskeletal forms of osteomas develop in the muscular tissue structures. The aetiology of osteomas is not clear and numerous theories have been implicated including trauma, infection and heredity [4].
Imaging plays a very important role in such cases of widespread involvement. The CT with 3D reconstruction enables better visualization and shows the exact extent of the lesion and the structures involved. The radiological features of having a ground glass appearance hinted to the diagnosis of a fibroosseous lesion. However, the histopathology confirmed the diagnosis of osteomas.
The presence of multiple osteomas gave rise to the suspicion of Gardner’s syndrome. The association between maxillofacial osteomas, cutaneous sebaceous cysts, desmoids, multiple supernumerary teeth and colorectal polyposis is known as Gardner’s syndrome [5]. As features other than osteomas were absent, the present case was considered to be of a non-syndromic variety of multiple central osteomas.
Osteomas although mostly asymptomatic, nevertheless occasionally patients can present symptoms like headache, invasion and deformity of the orbit, pneumocephalus with possible rhinorrhea and meningitis and infrequently, abscess formation [6]. Patients usually have aesthetic concerns which are met by surgical excision and contouring.
Conclusion
This case report is a very rare presentation of multiple unilateral central osteomas in a non-syndromic patient. It also emphasizes the importance of various investigations helping in the diagnosis of multiple radiopacities of the craniofacial bones.
[1]. Sayan NB, Ucok C, Karasu HA, Gunhan O, Peripheral osteoma of the oral and maxillofacial region: A study of 35 new casesJ Oral Maxillofac Surg 2002 60:1299-301. [Google Scholar]
[2]. Woldenberg Y, Nash M, Bodner L, Peripheral osteoma of the maxillofacial region. Diagnosis and management: A study of 14 casesMed Oral Patol Oral Cir Bucal 2005 10(Suppl 2):E139-42. [Google Scholar]
[3]. Hornigold R, Pearch BJ, Gleeson MJ, Anosteoma of the middle ear presenting with the Tullio phenomenonSkull Base 2003 13(2):113-17. [Google Scholar]
[4]. Schwartz LJ, Osteoma of the mastoidArch Otolaryngol 1961 74(3):350-53. [Google Scholar]
[5]. Lew D, DeWitt A, Hicks RJ, Cavalcanti MG, Osteomas of the condyle associated with Gardner’s syndrome causing limited mandibular movementJ Oral Maxillofac Surg 1999 57:1004-09. [Google Scholar]
[6]. Haddad FS, Haddad GF, Zaatari G, Cranialosteomas: their classification and management. Report on a giant osteoma and review of theliteratureSurg Neurol 1997 48(2):143-47. [Google Scholar]