Oral Pulse Granuloma: A Veiled Entity
Ashalata Gannepalli1, Venkat Baghirath Pacha2, Bhargavi Krishna Ayinampudi3, Anuradha Chandragiri4, Aditya Mohan Alwala5
1 Professor, Department of Oral Maxillofacial Pathology and Microbiology, Panineeya Mahavidyalaya Institute of Dental Sciences and Research Centre, Hyderabad, Telangana, India.
2 Professor and Head, Department of Oral Maxillofacial Pathology and Microbiology, Panineeya Mahavidyalaya Institute of Dental Sciences and Research Centre, Hyderabad, Telangana, India.
3 Professor, Department of Oral Maxillofacial Pathology and Microbiology, Panineeya Mahavidyalaya Institute of Dental Sciences and Research Centre, Hyderabad, Telangana, India.
4 Postgraduate Student, Department of Oral Maxillofacial Pathology and Microbiology, Panineeya Mahavidyalaya Institute of Dental Sciences and Research Centre, Hyderabad, Telangana, India.
5 Senior Lecturer, Department of Oral Maxillofacial Surgery, Panineeya Mahavidyalaya Institute of Dental Sciences and Research Centre, Hyderabad, Telangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ashalata Gannepalli, Professor, Department of Oral Maxillofacial Pathology and Microbiology, Panineeya Mahavidyalaya Institute of Dental Sciences and Research Centre, Hyderabad, Telangana, India.
E-mail: ashalatamds@gmail.com
Hyaline rings, Periapical, Granuloma, Cellulose, Legumes
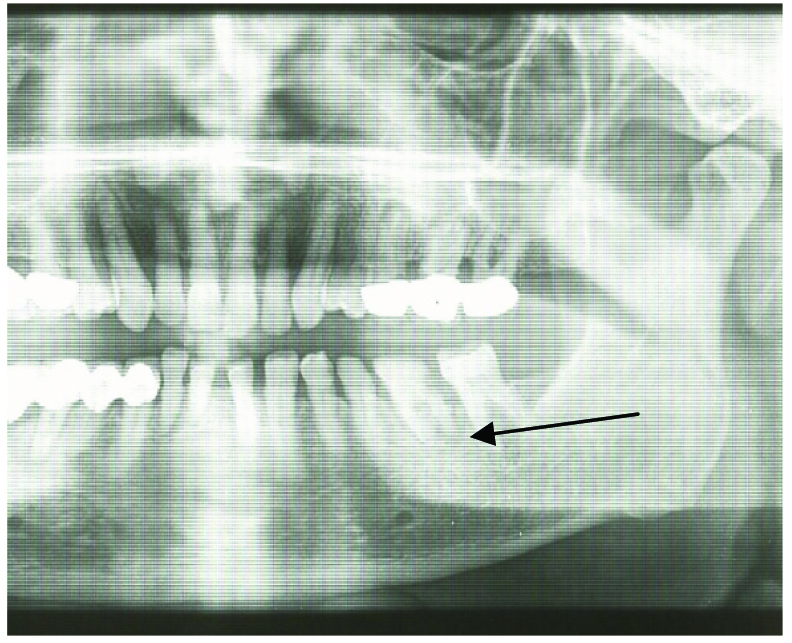
A 65-year-old man reported to Department of Oral and Maxillofacial Surgery with a painful swelling over the left mandibular molar region and inability to open the mouth since one month. The patient gave history of pain since one and half month and noticed the swelling since 15 days. His general health was non-contributory and clinical examination revealed poor oral hygiene with fixed partial dentures, periodontitis and gingivitis. Intra-oral examination revealed smooth localized swelling in relation to tooth #36, which was grossly decayed with deep periodontal pocket involving furcation area with food debris and calculus. There was pain on palpation and percussion. Oral hygiene was poor with fixed partial dentures, gingivitis and periodontitis. A provisional diagnosis of chronic periodontal abscess was given and differential diagnoses of chronic periapical abscess/granuloma were considered. On radiographic examination Orthopantomograph (OPG) revealed periapical radiolucency pertaining to tooth #36 [Table/Fig-1]. With a clinical diagnosis of a chronic periapical abscess due to combined periodontic-endodontic involvement was considered. As the tooth was grossly decayed with furcation involvement, the patient was referred to the Department of Oral and Maxillofacial Surgery for extraction of tooth #36.
OPG showing grossly decayed tooth #36 with periapical radiolucency and deep periodontal pocket on distal aspect.
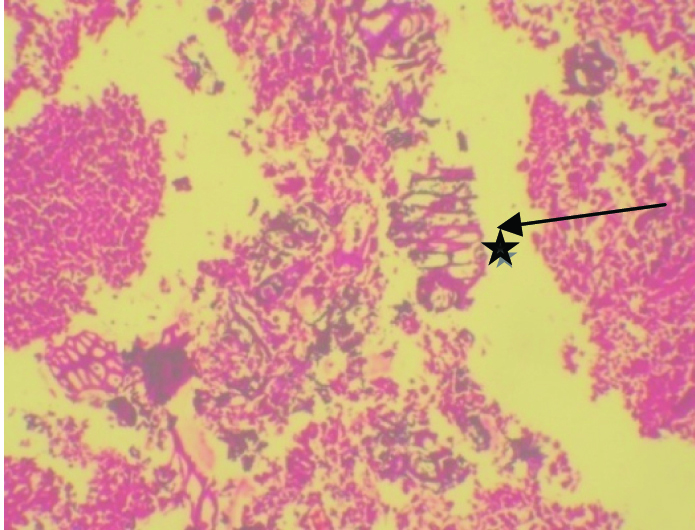
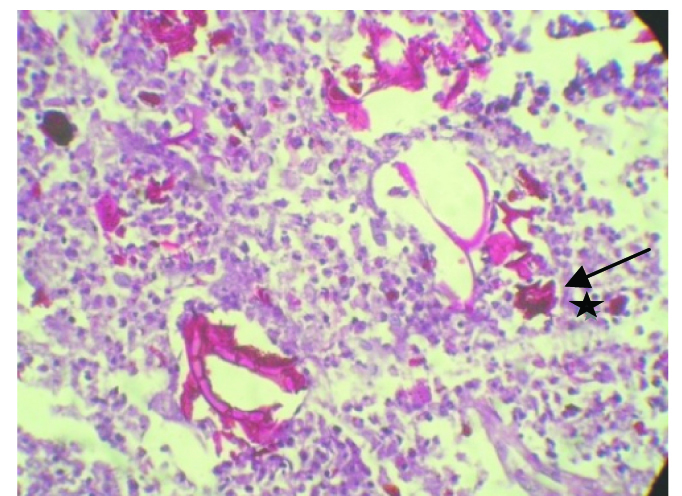
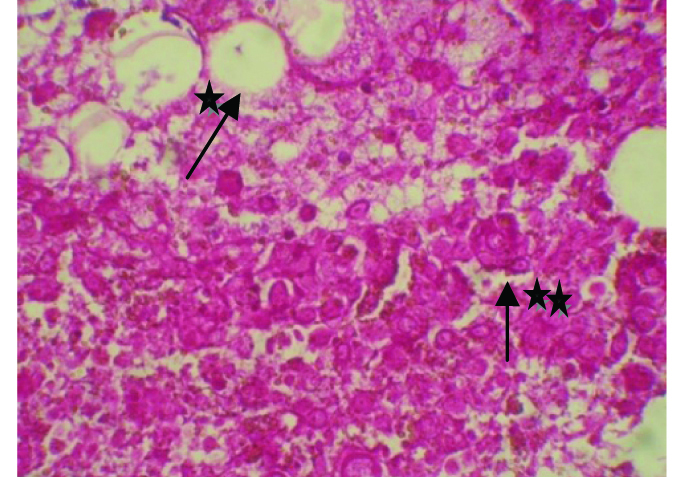
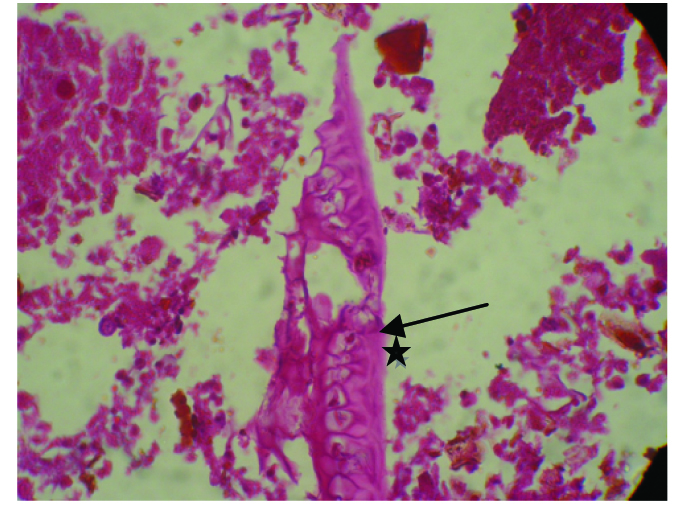
On extraction the surgeon noticed tooth specimen with attached soft tissue. The tooth socket was thoroughly curetted and specimen was sent for routine histopathological examination [Table/Fig-2]. Histopathological examination showed an interesting finding of multiple fragments of fibrous tissue, granulation tissue and area of eosinophilic spherical bodies, and refractile hyaline rings. There was a mixed inflammatory infiltrate consisting of predominantly lymphocytes, plasma cells, macrophages, foamy histiocytes and few giant cells [Table/Fig-3,4]. The hyaline rings were eosinophilic and Periodic Acid Schiff (PAS) positive, with few areas showing bacterial colonies [Table/Fig-5,6 and 7]. The hexagonal rings with spherical bodies, granular bodies, hyaline rings appeared to be derived from parenchymatous tissue of vegetable origin. Hence, the final diagnosis was given as chronic pulse granuloma. The patient was recalled after one month and showed a well healed tooth socket.
H&E section revealing inflammatory cells with eosinophilic hyaline rings (*).
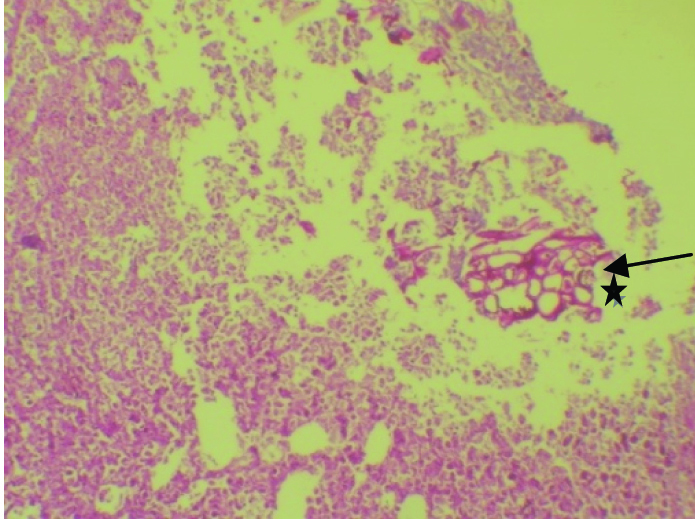
H&E (x4), Hyaline rings surrounded by chronic inflammatory cells forming a granuloma (*).
H&E section (x40), Giant cell (*), epitheloid macrophages (**), hyaline rings.
PAS stain(x10), Chronic inflammatory cells with PAS positive hyaline (*) rings.
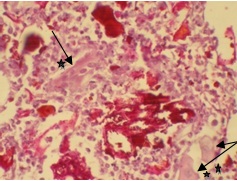
H&E, (x40), Foamy histiocytes (*), eosinophilic spherical granular material (**)
H&E (x40), eosinophilic hyaline material (*) resembling vegetable matter.
Discussion
Oral pulse granuloma is a rare lesion characterized by the presence of numerous multinucleated giant cells and hyaline rings. It was first described by Lewars in 1970, as an inflammatory lesion in the buccal sulcus of lower denture wearers. Various terminologies were used for this entity, Rannie (1975) described them as “Chronic Mandibular Periostitis Associated with Vasculitis”, Dunlap and Barker (1977) used the term ‘Giant Cell Angiopathy’. The term “Oral Pulse Granuloma” which is most preferred, was given by King in 1978, for the lesions occurring in the oral cavity [1,2]. Although most often associated with the oral cavity, pulse granuloma is also seen infrequently in the lungs, alimentary tract, fallopian tube, skin etc., [2].
Chou L et al., classified these lesions into central and peripheral according to the location and designated them as “Hyaline Ring Granuloma” [3]. Peripheral pulse granulomas have been described on lower lip, gingiva, dorsum of tongue, etc., [1,4,5].
In the oral cavity these are most often seen in edentulous jaws or in patients with a history of dental procedures [1]. They are reported in the walls of periapical/residual cysts, nasopalatine cysts, keratocysts, in granulomas involving carious teeth/tooth roots left open or teeth with failed endodontic therapy as seen in the present case [5–7]. The age range is from 6-71 years, with two thirds of the lesions in males. The lower jaw is commonly involved in the premolar-molar region. The signs and symptoms are of pain, swelling, discharge, chronic sinus, or may be found on routine clinical or radiologic examination [2,5]. Radiographic examination is not pathognomic of pulse granulomas, intra-osseous pulse granuloma manifests as an irregular radiolucent lesion and extra-osseous presents as poorly defined erosion of the crest of the alveolar ridge [5–7]. Similarly the presented case showed deep carious lesion and also deep periodontal pocket (a combination of possible periodontic-endodontic lesion), through which the foreign food material might have been introduced into periapical area. Radiographically, an intra-osseous irregular radiolucent lesion with respect to tooth #36 was observed, similar to other cases in literature [2,5].
Pulse granuloma is an exceptionally reported oral finding with indeterminate aetiology. The aetiopathogenesis of pulse granuloma is a complex one evolved from two concepts, i.e., exogenous and endogenous. Most authors favor the exogenous origin for these lesions, based on the suggestion of implantation of food particles of plant origin especially of leguminous (pulse) origin, through extraction sockets, deep periodontal pockets, unfilled root canals and grossly decayed teeth. Whereas, the endogenous origin is suggested to be localized degenerative changes in the walls of blood vessels, collagen degeneration, etc., [2,3].
The above concepts arose mainly due to the presence of hyaline rings in the histopathology. They appear as spherical, ovoid, or irregular bodies surrounded by fibroblasts and appear as homogeneous, eosinophilic material in hematoxylin and eosin stained section surrounded by acute and chronic inflammatory cells and foreign body giant cells [7].
The hyaline material characteristic of these lesions has been debated by many authors to be vegetable matter, lentils and pulses of leguminous origin [2]. The present case showed vegetable matter with refractile hyaline rings, honeycomb like structures, spherical to ovoid granular material, which might have incited a granulomatous response as suggested by Knoblich R in his experiments. He showed that the cellulose portion of the food particle is indigestible and persists as hyaline material whereas the starch form gets easily digested. This cellulose material invokes a chronic granulomatous response or allergic granulomas [8].
Conclusion
With regard to the histopathological features which was a chance finding in the present case, summing up to the diagnosis of a pulse granuloma, it can be inferred that it is a classical foreign body granuloma that occurs irrespective of the clinical manifestations present. Oral pulse granuloma is a rare entity in which no features considered clinically pathognomic of pulse granuloma can be seen and remains largely a microscopic diagnosis. A more widespread knowledge on the unusual sites of occurrence and clinical manifestations may aware the clinicians about the diagnostic hazard of mistaking pulse granulomas for other entities.
[1]. Saraswathi Vishnu Naik, Syed Ghousia, Kamalaksharappa Shashibhushan Deepa Benni, Pediatric oral pulse granuloma – A rare entityDent Res J 2012 9(6):812-15. [Google Scholar]
[2]. Philipsen HP, Reichart PA, Pulse or hyaline ring granulomas. Review of the literature on etiopathogenesis of oral and extra-oral lesionsClin Oral Invest 2010 14:121-28. [Google Scholar]
[3]. Chou L, Ficarra G, Hansen LS, Hyaline ring granuloma: A distinct oral entityOral Surg Oral Med Oral Pathol 1990 70:318-24. [Google Scholar]
[4]. Acharya S, Hallikeri K, Anehosur V, Okade A, Oral pulse or hyaline ring granuloma: A case report and a brief reviewJ Indian Soc Periodontol 2015 19(3):327-32. [Google Scholar]
[5]. Gueiros LA, Santos Silva AR, Lopes MA, Jorge J, Distinctive aspects of oral hyaline ring granulomasOral Surg Oral Med Oral Pathol Oral Radiol Endod 2008 106:e35-e39. [Google Scholar]
[6]. Kotrashetti VS, Angadi PV, Mane DR, Hallikerimath SR, Oral pulse granuloma associated with keratocystic odontogenic tumor: Report of a case and review on etiopathogenesisAnn Maxillofac Sur 2011 1(1):83-86. [Google Scholar]
[7]. Talacko AA, Radden BG, Oral pulse granuloma: Clinical and histopathological featuresInt J Oral Maxillofac Surg 1988 17:343-46. [Google Scholar]
[8]. Knoblich R, Pulmonary granulomatosis caused by vegetable particles. So called lentil pulse pneumoniaAm Rev Respir Dis 1969 99:380-89. [Google Scholar]