Introduction
Periodontal pain caused by elastomeric separators is a very common problem in the commencement of orthodontic treatment. Previous studies have shown good results in reducing this pain by Low Level Laser Therapy (LLLT) and different protocols of application have been suggested in the literature.
Aim
This trial aimed to evaluate LLLT on managing orthodontic pain caused by elastomeric separators and to compare single versus double irradiation in possible pain reduction.
Materials and Methods
A clinical randomized compound (parallel-group and split-mouth design) trial was conducted on 36 patients between 12 and 26 years of age. Elastomeric separators were placed at the mesial and distal surfaces of the first molars in one jaw (upper or lower) for each patient and in only one side of the mouth (the other side served as the placebo side). The trial had two groups: the first group received single irradiation of LLLT [Gallium Aluminum Arsenide (GaAlAs): 830 nm, 4J/cm2, 100mW] immediately after separators insertion, where as the second group received double irradiation immediately after separators insertion and after 24hours. All patients were instructed to rate the level of pain at 1, 6, 24, 48, 96 hours on a Visual Analog Scale (VAS). The student ‘t’ tests, repeated measures ANOVA and LSD post-hoc tests were employed.
Results
LLLT was successful in reducing post-separation pain when the experimental side was compared to the placebo side at all assessment times in each group (p<0.05). There were no statistically significant differences between single and double irradiation groups in terms of pain reduction (p>0.05).
Conclusion
GaAlAs LLLT application reduced early orthodontic pain caused by elastomeric separators by single or double irradiation.
Introduction
Orthodontic tooth movement causes injury in the periodontal structures including periodontal ligament which leads to pain and discomfort sensation [1]. This sensation appears because of pressure and tension in periodontal ligament that releases inflammatory mediators [2] such as histamine, serotonin, dopamine, glycine, prostaglandins, substance P, and cytokines [3]. Many surveys have shown that 70-95% of patients complain of pain caused by orthodontic appliances [4], and described orthodontic pain as a main reason to interrupt the treatment [5]. The percentage of adolescents reporting pain during fixed orthodontic treatment has been shown to be 90% [6]. Adolescents showed worse pain than adults [7], but some authors have reported that pain is more intense in adults [8]. Early orthodontic pain which is caused by elastomeric separators starts during the first 24 hours of insertion [6,9,10], reaches the worst pain after 24 or 48 hours [9,11]. The post-separation pain has been described as a continuous pain during the first two days of placement, and then it becomes intermittent [12].
An orthodontic tooth movement is associated with pain not related to infection but to inflammatory processes that are localized and last for a short period of time [13]. This pain can be controlled sometimes using Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) [14]. It has been shown that NSAIDs may decrease tooth movement velocity [15], and they have many contraindications such as allergic reaction (like aspirin), kidney or liver injury, hypertension, bone marrow disorder and pregnancy [16]. For these reasons, some authors have recommended the use of local analgesic therapy in order to avoid the side effects of these drugs [13]. Recent studies have reported the effectiveness of Low Level Laser Therapy (LLLT) to reduce pain in several dental fields like endodontic pain [17] and extraction [18]. LLLT has also been shown to reduce early orthodontic pain [9,10,13,19,20], and pain caused by orthodontic tooth movement [8,21].
Laser has been introduced in the field of dentistry in the last three decades [22]. There are two main types of laser: High Level Laser (HLL) which is used in soft and hard tissues surgeries and in some specific dental practices [22], and LLLT which increases healing, decrease pain and inflammatory reactions [23]. LLLT is called as cold, soft and therapeutic laser which exists in near infrared spectrum, 630-980nm, and its power 50-500mw [24]. It doesn’t make any absolute changes such as evaporation of water, increase heat, deform proteins, or abrasion of tissues [23] so, it is safe and globally accepted, and doesn’t cause mutations or cancers [15]. This laser has many hypothesis in reducing pain, it could modulate the inflammatory response to reduce pain, or by altering conduction and excitation of the peripheral nerves, or stimulating endorphins release [13]. LLLT has also a positive role in orthodontic treatment because it has been shown to enhance bone remodeling and increase tooth movement [25], as well as to relieve orthodontic pain [9]. Lim et al., in a clinical investigation found an efficacy of LLLT in pain relief caused by orthodontic separators [26], and this study was followed by several studies that have evaluated this technique [9,14,19,20]. Nobrega et al., and Marini et al., evaluated the single irradiation of LLLT, whereas, Eslamian et al., studied double irradiation and Kim et al., used multiple irradiation [9,14,27,28]. All these authors have found that LLLT has a significant effect in reducing pain following the use of elastomeric separators. These protocols (single, double or multiple irradiations) were effective, but there was no reason why previous studies preferred one protocol over another and no differentiation was made between the employed protocols.
The objectives of this Randomized Controlled Trial (RCT) were to evaluate the efficacy of LLLT on controlling pain caused by elastomeric separators, and to compare single irradiation versus double irradiation in terms of pain reduction.
Materials and Methods
Study Design: This was a randomized compound (parallel-group and split-mouth design) controlled clinical trial conducted at the Laser Department at University of Damascus Dental School, Syria, between November 2014 and June 2015. Ethical Approval was obtained from the Local Ethic Research Committee at the University of Damascus Dental School (Reference Number: UDDS-380-30032014/SRC-2209). This trial was registered at Clinical Trials.gov (Identifier: NCT02209818).
Patient Selection: A calculation of sample size was performed using Minitab® 17 (Minitab Inc., Pennsylvania, USA) with an alpha level of 0.05, a power of 90%, and assuming that the smallest difference requiring detection in pain level was 10mm on a visual analog scale with a variation of 8.1 from a previous study [29], a sample of 30 patients was required, i.e., 15 patients in each group.
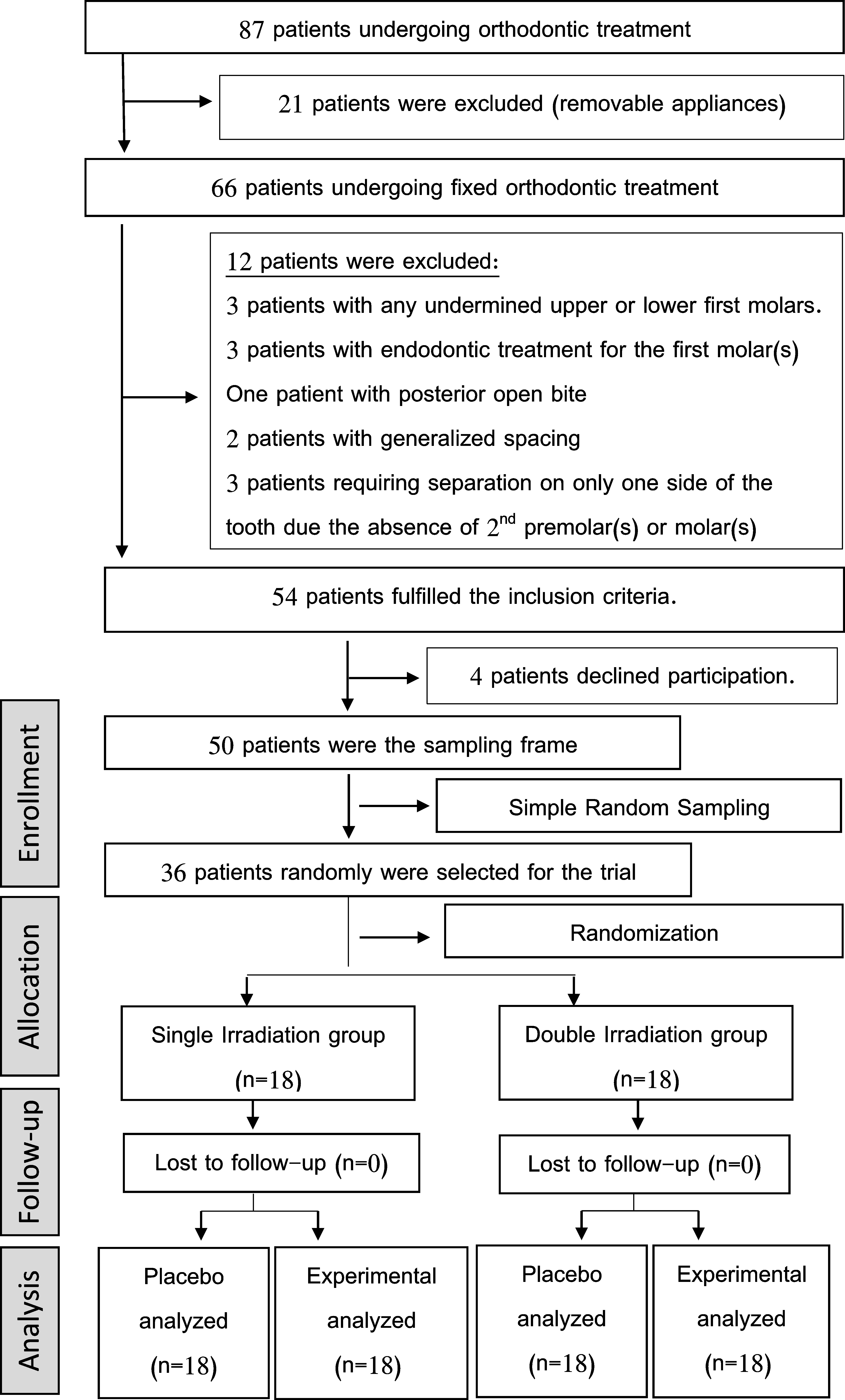
Patients of this study were selected from Department of Ortho-dontics at University of Damascus Dental School. The treatmemt plan of 87 patients was reviewed, but the number of patients who met the inclusion criteria and agreed to participate in this study was only 50. According to a priori sample size calculation which indicated the need for 30 patients, a simple random sampling was applied to select 36 patients from the sampling frame; this number was chosen for any potential drop-out after the commencement of the trial.
All patients read and signed the informed consent forms before the initiation of the study. The inclusion criteria were: (1) the absence of any systemic or periodontal disease; (2) the absence of any chronic or neural pain; (3) the avoidance of using analgesics or anti-inflammatory drugs; (4) loose contact points on the mesial or distal surface of the first molars; (5) pigmentation on the gingiva where the laser will be applied; (6) and the first molars must be fully erupted and without any treated or non-treated apical lesions. Elastomeric separators (Ortho Technology Company, Florida, USA) were inserted mesial and distal to the first molars on both sides of one jaw for every patient.
Study Groups: Using a software-generated list of random numbers the recruited patients were divided into two parallel groups with a 1:1 allocation ratio. First group received Single Irradiation (SI) of LLLT immediately after elastomeric separators insertion, whereas the second group received Double Irradiation (DI) at the following times: (1) immediately following elastomeric separators insertion; and (2) after 24 hours of elastomeric separators insertion. One side was chosen randomly to be the experimental side, and the other served as the placebo side employing a computer-generated list of random sides [Table/Fig-1].
CONSROT 2010 flow diagram of patients’ recruitment and follow-up.
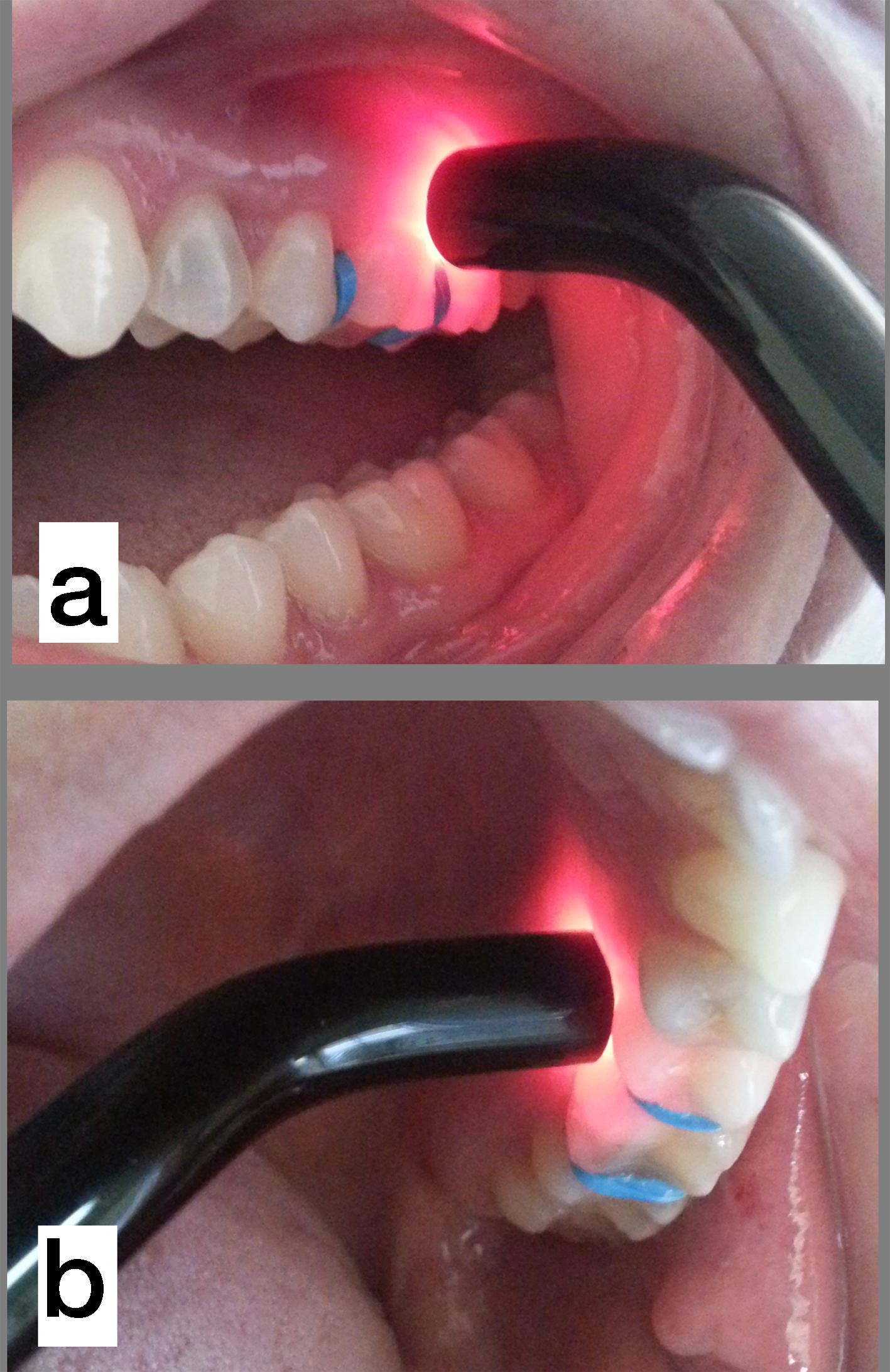
Laser Parameters and Procedure: A low level medical semicon-ductor laser with a Gallium Aluminum Arsenide (GaAlAs)diode [Table/Fig-2], wavelength 830 nm, energy density 4J/cm2, power 100 mW, laser spot diameter 7mm (Diobeam®, CMSDental, Copenhagen, Denmark). The irradiation time was automatically set according to the chosen dose (the irradiation time was 28 seconds per each 4J/cm2). Eight points were irradiated in every side, mesial and distal to the first molar, mesial to the second premolar, distal to the second molar (buccally and palatally/ lingually) [Table/Fig-3]. In the placebo side, the safety cover was removed to pretend in front of the patient as if his/her side of the jaw was being irradiated and the device was allowed to give sounds as if it was working. The same duration of application was followed (i.e., 28 seconds).

Laser application, A: from buccal side, B: from lingual side.
Pain Assessment: All patients instructed to rate their pain level on a Visual Analog Scale (VAS). A line of 100mm length was used with the left side representing no pain (i.e., score=0) and right side representing the worst pain (i.e., score=100). The assessment of pain was conducted at 1,6,24,48,96 hours after separation. Each patient was given a questionnaire and he/she was asked to put a vertical mark on the line at a point which best represented the perceived level of pain. The patients instructed to bring the questionnaires in the next appointment. The assessment of pain was done by measuring the distance from left side to the vertical mark and was converted in mm. Patients were instructed not to take any analgesic during pain assessment period. In case of severe pain, they were allowed to take one or two tablets of paracetamol 500mg (acetaminophen) but they were asked to fill in the questionnaire first before taking any tablet.
Statistical Analysis
For data collection, Microsoft Excel Software was used. Statistical analysis was performed using Minitab® V17 (Minitab Inc., Pennsylvania, USA) and SPSS®V17 (SPSS Inc., Chicago, IL, USA). The student t tests were employed to evaluate the efficacy of LLLT in management pain caused by orthodontic separators, and to compare between single and double irradiation. Repeated measures ANOVA was employed to evaluate change in pain perception over time and the Least Significant Difference (LSD) method was used for post-hoc tests.
Results
The mean age of patients was 18.4 years (range: 12-26 years; 10 males, 26 females) [Table/Fig-4]. Separation was applied in the maxillary arch for 21 patients and in the mandibular arch for 15 patients. Pain perception started between one and 24 hours following separators insertion (pain started after one hour for 23 patients, after six hours for six patients and after 24 hours for three patients) and there were four patients who never experienced pain during the whole period of assessment.
Basic sample characteristics.
| Group | Gendern (%) | Age Mean (SD) | Maxi-mum age | Mini-mum age | Maxillary separation: n(%) | Mandibular separation: n(%) |
|---|
| Single Irradiation | Male5 (13.89%) | 17.20 (5.07) | 24 | 12 | 3 (8.33%) | 2 (5.56%) |
| Female13 (36.11%) | 17.54 (4.91) | 26 | 12 | 6 (16.67%) | 7 (19.44%) |
| Double Irradiation | Male5 (13.89%) | 21.40 (2.074) | 25 | 20 | 2 (5.56%) | 3 (8.33%) |
| Female13 (36.11%) | 18.53 (3.50) | 23 | 13 | 10 (27.78%) | 3 (8.33%) |
| Total | 36 (100%) | 18.39 (4.20) | 26 | 12 | 21 (58.34%) | 15 (41.66%) |
Pain perception for the single irradiation group reached its maximum mean value at 24 hours following separation in both sides. Changes between assessment times were statistically significant (p=0.003 for the placebo side and p=0.043 for the experimental side) [Table/Fig-5,6 and 7] and there were statistically significant differences between the experimental and the placebo sides at all times except for the last assessment time (p=0.526) [Table/Fig-8].
Descriptive statistics of pain levels in the two groups of patients at the different assessment times.
| Group | Side | T1Mean (SD) | T2Mean (SD) | T3Mean (SD) | T4Mean (SD) | T5Mean (SD) | F value | p-value |
|---|
| Single Irradiation | Experimental | 12.00 (13.39) | 18.44 (19.32) | 27.22 (20.99) | 20.11 (21.85) | 11.50 (15.18) | 3.871 | 0.013* |
| Placebo | 25.28 (19.70) | 39.44 (28.01) | 41.78 (24.00) | 30.28 (23.89) | 12.78 (18.25) | 6.544 | 0.002** |
| Double Irradiation | Experimental | 6.28 (11.82) | 13.89 (20.70) | 18.00 (20.83) | 20.89 (24.74) | 18.67 (21.58) | 3.580 | 0.025* |
| Placebo | 11.56 (17.57) | 23.17 (25.49) | 30.06 (24.22) | 37.00 (33.45) | 24.78 (26.09) | 4.026 | 0.015* |
T1: one hour following separation; T2: six hours following separation; T3: 24 hours following separation; T4: 48 hours following separation; T5: 96 hours following separation. Employing Repeated Measure ANOVA. * significant difference at p<0.05, ** significant difference at p<0.01
Descriptive statistics of the observed changes between assessment times (pairwise comparisons) in the single irradiation group in the experimental side. Post-hoc tests were performed using Least Significant Difference (LSD) method and the p-values of significance tests are given.
| Time | Comparison | Mean(SD) | p-value | 95%CI |
|---|
| The lower bound | The upper bound |
|---|
| T1 | T1 vs T2 | -6.44 (3.17) | 0. 058 | -13.14 | 0.25 |
| T1 vs T3 | -15.22 (4.55) | 0.004** | -24.83 | -5.61 |
| T1 vs T4 | -8.11 (5.53) | 0.161 | -19.78 | 3.56 |
| T1 vs T5 | 0.50 (4.06) | 0.904 | -8.07 | 9.07 |
| T2 | T2 vs T3 | -8.77 (4.86) | 0.089 | -19.03 | 1.48 |
| T2 vs T4 | -1.66 (4.92) | 0.739 | -12.04 | 8.71 |
| T2 vs T5 | 6.94 (4.39) | 0.132 | -2.32 | 16.21 |
| T3 | T3 vs T4 | 7.11 (5.56) | 0.218 | -4.62 | 18.84 |
| T3 vs T5 | 15.72 (4.94) | 0.005** | 5.30 | 26.14 |
| T4 | T4 vs T5 | 8.61 (4.04) | 0.048* | 0.08 | 17.14 |
T1: one hour following separation; T2: six hours following separation; T3: 24 hours following separation; T4: 48 hours following separation; T5: 96 hours following separation.
* significant difference at p<0.05, ** significant difference at p<0.01
Descriptive statistics of the observed changes between assessment times (pairwise comparisons) in the single irradiation group in the placebo side. Post-hoc tests were performed using Least Significant Difference (LSD) method and the p-values of significance tests are given.
| Time | Comparison | T valueMean (SD) | p-value | 95%CI |
|---|
| The lower bound | The upper bound |
|---|
| T1 | T1 vs T2 | -14.16 (4.65) | 0.007** | -23.99 | -4.34 |
| T1 vs T3 | -16.50 (4.02) | 0.001** | -24.99 | -8.01 |
| T1 vs T4 | -5.00 (6.90) | 0.479 | -19.56 | 9.56 |
| T1 vs T5 | 12.50 (6.68) | 0.079 | -1.59 | 26.59 |
| T2 | T2 vs T3 | -2.33 (4.85) | 0.637 | -12.57 | 7.90 |
| T2 vs T4 | 9.17 (8.09) | 0.273 | -7.90 | 26.23 |
| T2 vs T5 | 26.67 (7.60) | 0.003** | 10.64 | 42.70 |
| T3 | T3 vs T4 | 11.50 (7.06) | 0.122 | -3.40 | 26.40 |
| T3 vs T5 | 29.00 (7.70) | 0.002** | 12.75 | 45.25 |
| T4 | T4 vs T5 | 17.50 (5.64) | 0.006** | 5.59 | 29.41 |
T1: one hour following separation; T2: six hours following separation; T3: 24 hours following separation; T4: 48 hours following separation; T5: 96 hours following separation.
* significant difference at p<0.05, ** significant difference at p<0.01
Descriptive statistics of the differences between the experimental and control sides in each group at each assessment time. The p-values of the significance test are also included.
| Group | Time | Mean difference between the exp. and cont. sides (SD) | T value | p-value | 95%CI |
|---|
| The lower bound | The upper bound |
|---|
| Single Irradiation | T1 | 13.28 (17.11) | 3.29 | 0.004** | 4.77 | 21.79 |
| T2 | 21.00(23.19) | 3.84 | 0.001** | 9.47 | 32.53 |
| T3 | 14.56(23.22) | 2.66 | 0.016* | 3.01 | 26.10 |
| T4 | 10.17(15.18) | 2.84 | 0.011* | 2.62 | 17.72 |
| T5 | 1.28(8.37) | 0.65 | 0.526 | -2.88 | 5.44 |
| Double Irradiation | T1 | 5.28(7.01) | 3.19 | 0.005** | 1.79 | 8.76 |
| T2 | 9.28(16.84) | 2.34 | 0.032* | 0.90 | 17.65 |
| T3 | 12.06(14.11) | 3.63 | 0.002** | 5.04 | 19.07 |
| T4 | 16.11(24.91) | 2.74 | 0.014* | 3.72 | 28.50 |
| T5 | 6.11 (9.21) | 2.82 | 0.012* | 1.53 | 10.69 |
T1: one hour following separation; T2: six hours following separation; T3: 24 hours following separation; T4: 48 hours following separation; T5: 96 hours following separation. Employing Paired T-Test
* significant difference at p<0.05, ** significant difference at p<0.01
Pain perception in the double irradiation group reached its maximum mean value at 48 hours following separation in both sides with significant differences being observed over time (p=0.016 for the placebo side and p=0.026 for the experimental side) [Table/Fig-5,9,10]. There were statistically significant differences between the experimental and the placebo sides at all assessment times [Table/Fig-8].
Descriptive statistics of the observed changes between assessment times (pairwise comparisons) in the double irradiation group in the experimental side. Post-hoc tests were performed using Least Significant Difference (LSD) method and the p-values of significance tests are given.
| Time | Comparison | Mean(SD) | p-value | 95%CI |
|---|
| The lower bound | The upper bound |
|---|
| T1 | T1 vs T2 | -7.61 (3.12) | 0.026* | -14.182 | -1.040 |
| T1 vs T3 | -11.72 (4.27) | 0.014* | -20.73 | -2.72 |
| T1 vs T4 | -14.61 (4.67) | 0.006** | -24.47 | -4.75 |
| T1 vs T5 | -12.39 (4.70) | 0.017* | -22.30 | -2.474 |
| T2 | T2 vs T3 | -4.11 (4.52) | 0.376 | -13.65 | 5.43 |
| T2 vs T4 | -7.00 (4.89) | 0.171 | -17.32 | 3.32 |
| T2 vs T5 | -4.78 (5.42) | 0.390 | -16.20 | 6.65 |
| T3 | T3 vs T4 | -2.89 (4.09) | 0.489 | -11.51 | 5.73 |
| T3 vs T5 | -0.67 (3.95) | 0.868 | -9.00 | 7.67 |
| T4 | T4 vs T5 | 2.22 (2.80) | 0.438 | -3.69 | 8.13 |
T1: one hour following separation; T2: six hours following separation; T3: 24 hours following separation; T4: 48 hours following separation; T5: 96 hours following separation.
* significant difference at p<0.05, ** significant difference at p<0.01
Descriptive statistics of the observed changes between assessment times (pairwise comparisons) in the double irradiation group in the placebo side. Post-hoc tests were performed using Least Significant Difference (LSD) method and the p-values of significance tests are given.
| Time | Comparison | Mean(SD) | T value | p-value | 95%CI |
|---|
| The lower bound | The upper bound |
|---|
| T1 | T1 vs T2 | -11.61 (4.61) | -2.52 | 0.022* | -21.35 | -1.88 |
| T1 vs T3 | -18.50 (5.95) | -3.11 | 0.006** | -31.04 | -5.96 |
| T1 vs T4 | -25.44 (7.44) | -3.42 | 0.003** | -41.14 | -9.75 |
| T1 vs T5 | -13.22 (5.79) | -2.76 | 0.035* | -25.43 | -1.02 |
| T2 | T2 vs T3 | -6.89 (6.78) | -1.02 | 0.324 | -21.18 | 7.41 |
| T2 vs T4 | -13.83 (8.99) | -1.54 | 0.142 | -32.81 | 5.14 |
| T2 vs T5 | -1.61 (7.12) | -0.67 | 0.82 | -16.63 | 13.41 |
| T3 | T3 vs T4 | -6.94 (7.31) | -0.95 | 0.355 | -22.36 | 8.47 |
| T3 vs T5 | 5.28 (4.43) | 0.33 | 0.249 | -4.06 | 14.61 |
| T4 | T4 vs T5 | 12.22 (6.55) | 1.13 | 0.079 | -1.59 | 26.03 |
T1: one hour following separation; T2: six hours following separation; T3: 24 hours following separation; T4: 48 hours following separation; T5: 96 hours following separation.
* significant difference at p<0.05, ** significant difference at p<0.01
When single irradiation was compared with double irradiation, no significant differences between the experimental sides were observed at all assessment times [Table/Fig-11].
Descriptive statistics of the differences between the single irradiation and double irradiation groups at the experimental side at each assessment time. The p-values of significance test are also given.
| Time | Single Irradiation mean(SD) | Double Irradiation mean (SD) | Mean Diffe-rence | T value* | p-value | 95%CI |
|---|
| The lower bound | The upper bound |
| T1 | 12.00 (13.39) | 6.28 (11.82) | 5.72 | 1.36 | 0.183 | -2.84 | 14.29 |
| T2 | 18.44 (19.32) | 13.89 (20.70) | 4.56 | 0.68 | 0.500 | -9.02 | 18.14 |
| T3 | 27.22 (20.99) | 18.00 (20.83) | 9.22 | 1.32 | 0.195 | -4.96 | 23.40 |
| T4 | 20.11 (21.85) | 20.89 (24.74) | -0.78 | -0.10 | 0.921 | -16.61 | 15.05 |
| T5 | 11.5 (15.18) | 18.67 (21.58) | -7.17 | -1.15 | 0.258 | -19.87 | 5.54 |
*Employing Tow-Sample T-Test
T1: one hour following separation; T2: six hours following separation; T3: 24 hours following separation; T4: 48 hours following separation; T5: 96 hours following separation.
Discussion
Periodontal pain caused by elastomeric separators is an inflam-matory pain and the employed laser technique should be effective and acts as an anti-inflammatory tool without increasing tissue heat. Lasers in 600-1000nm range works very fine for this purpose [19]. GaAlAs 830nm has superiority in tissue penetration than other lasers [27], and has an advanced analgesic effect that has been documented in clinical and laboratory studies [13].
Selection of the right dose is an important element that should be taken into account to reach an ideal result. High dosage should be avoided in inflammatory pain because it reduces the anti-inflammatory and analgesic effects [9]. Dosage makes the treatment more effective when it is lower than 20J/cm2 per area and 5J/cm2 per point [9,19]. In this study the dosage was 4 J/cm2 per point and 16 J/cm2 per tooth, so it was within the acceptable range.
Using different wavelengths could also affect the observed changes [23]. In the current study, GaAlAs laser was used with a wavelength of 830nm which showed significant difference between experimental and placebo groups. Kim et al., used AlGaInP laser with a wavelength of 635nm and found that there was a significant difference in reducing separation pain between the control and experimental groups [14]. Furquim RD et al., did not found any significant difference between the experimental and placebo sides in their trial but they applied a high dose of 80J/cm2 [29] violating the acceptable range which has been shown to be between 0.3 and 19 J/cm2 and less than 20J/cm2 according to several previous reports [9,30].
It is felt that conducting this study on split-mouth design would be better than the parallel-group design since having two groups of patients even though randomly allocated would not probably allow precise estimation of the effect of laser irradiation because of the expected variability when analyzing two groups of different subjects [31]. On the other hand, Lim HM et al., conducted a four-arm split-mouth randomized controlled trial to test laser effect in reducing separation pain [26]. One quadrant was chosen as a placebo and the rest quadrants were irradiated with different doses. They reported that there were no significant differences in pain reduction following separation between these quadrants. In this type of study, pain in one jaw could irradiate to the opposite jaw and patients may have been confused in assessing the actual pain they encountered at each quadrant [32]. Abtahi SM et al., found a significant difference in pain reduction in the experimental side compared to the control side on the 2nd day only and not in the following assessments. However, LLLT irradiation was performed at 3 locations and from the buccal side only [33]. This may explain the less paramount effect of pain reduction observed in their study.
The VAS was used as a tool to measure pain perception because of its superiority on other scales and has been used in previous studies [9,13,14]. VAS is clear to use for all ages including young children [34] also it has two clear reasons of its excel. It allows to choose the exact degree of pain and gives the maximum chance to express personal response pattern [35].
The present study showed that pain by elastomeric separators started between one and 24hours following their insertion. Eslamian L et al., and Marini I et al., reported that pain started after separators insertion immediately and lasted up to 24hours [9,28], whereas Fujiyama K et al., surprisingly reported pain appearance after 30 seconds [36]. Artes-Ribas M et al., and Farias RD et al., reported pain appearance after 5 minutes [13,20]. These figures of early pain emergence could be attributed to patients realization of pain induced by nuisance and cannot be considered a real inflammatory pain. Other studies reported that the emergence of initial pain occurred after 2 to 24 hours [6,13,27]. Therefore, the first assessment of pain was decided to be at one hour following the insertion of elastomeric separators to make sure that we included the first possible signs of inflammatory pain. Pain was found to reach its maximum mean values at 24 hours for both sides in SI group and at 48 hour for both sides in DI group; a finding similar to previous studies [9,19,36].
In the current study, LLLT reduced pain and promoted analgesic effect for pain due to separation whether the application was single or double. Previous studies that discussed reducing pain by LLLT have used single, double or multiple irradiation [9,13,14]. Single irradiation has been discussed in several trials and many of them reported a significant effect in reducing separation pain in the experimental groups compared to the control groups [13,20,27].
Furthermore, Eslamian L et al., studied double irradiation to assess LLLT effectiveness in controlling separation pain. The study was a split-mouth design and LLLT applied on the irradiation quadrant immediately following separators insertion and 24hours post-separation. The results showed a significant difference in reducing pain between double-irradiated quadrants and the placebo quadrants in the first 3 days of the separation but not thereafter [9]. Pain reduction by repeated LLLT application was not different from that achieved with single application in this trial. It seems that laser application did not have a cumulative effect on pain reduction and it seems to be that the mechanism is triggered by laser application regarding its repetition.
Limitation
The clinical application of LLLT in managing post-separation pain can be expanded to include different orthodontic procedures well-known to be associated with pain such as alignment of crowded teeth, canine retraction, upper incisors retraction, and closure of interdental spaces. LLLT application may become a regular procedure in the daily orthodontic practice once all the parameters of its use have been fine tuned. This trial compared single versus double irradiation, but there are several other protocols of application that can be suggested. More research is required with different designs to find out the best protocol of application and with the expected future advances in laser technology it is possible that encountering pain during orthodontic treatment would become an idea of the past.
Conclusion
Low level laser therapy showed a significant reduction in the perceived pain following orthodontic elastomeric separation. Double irradiation did not have any additional impact in pain reduction compared to the single irradiation protocol.
T1: one hour following separation; T2: six hours following separation; T3: 24 hours following separation; T4: 48 hours following separation; T5: 96 hours following separation. Employing Repeated Measure ANOVA. * significant difference at p<0.05, ** significant difference at p<0.01
T1: one hour following separation; T2: six hours following separation; T3: 24 hours following separation; T4: 48 hours following separation; T5: 96 hours following separation.
* significant difference at p<0.05, ** significant difference at p<0.01
T1: one hour following separation; T2: six hours following separation; T3: 24 hours following separation; T4: 48 hours following separation; T5: 96 hours following separation.
* significant difference at p<0.05, ** significant difference at p<0.01
T1: one hour following separation; T2: six hours following separation; T3: 24 hours following separation; T4: 48 hours following separation; T5: 96 hours following separation. Employing Paired T-Test
* significant difference at p<0.05, ** significant difference at p<0.01
T1: one hour following separation; T2: six hours following separation; T3: 24 hours following separation; T4: 48 hours following separation; T5: 96 hours following separation.
* significant difference at p<0.05, ** significant difference at p<0.01
T1: one hour following separation; T2: six hours following separation; T3: 24 hours following separation; T4: 48 hours following separation; T5: 96 hours following separation.
* significant difference at p<0.05, ** significant difference at p<0.01
*Employing Tow-Sample T-Test
T1: one hour following separation; T2: six hours following separation; T3: 24 hours following separation; T4: 48 hours following separation; T5: 96 hours following separation.
[1]. Bruno MB, Bruno MA, Krymchantowski AV, da Motta AF, Mucha JN, A double-blind, randomized clinical trial assessing the effects of a single dose of preemptive anti-inflammatory treatment in orthodontic painProg Orthod 2011 12(1):2-7. [Google Scholar]
[2]. Xiaoting L, Yin T, Yangxi C, Interventions for pain during fixed orthodontic appliance therapy: A systematic reviewAngle Orthod 2010 80(5):925-32. [Google Scholar]
[3]. Alhashimi N, Frithiof L, Brudvik P, Bakhiet M, Orthodontic tooth movement and de novo synthesis of proinflammatory cytokinesAm J Orthod Dentofacial Orthop 2001 119(3):307-12. [Google Scholar]
[4]. Scheurer PA, Firestone AR, Bürgin WB, Perception of pain as a result of orthodontic treatment with fixed appliancesEur J Orthod 1996 18(4):349-57. [Google Scholar]
[5]. Kluemper GT, Hiser DG, Rayens MK, Jay MJ, Efficacy of a wax containing benzocaine in the relief of oral mucosal pain caused by orthodontic appliancesAm J Orthod Dentofacial Orthop 2002 122(4):359-65. [Google Scholar]
[6]. Shetty N, Patil AK, Ganeshkar SV, Hegde S, Comparison of the effects of ibuprofen andacetaminophen on PGE 2 levels in the GCF during orthodontic tooth movement: a human studyProg Orthod 2013 14(1):1 [Google Scholar]
[7]. Brown DF, Moerenhout RG, The pain experience and psychological adjustment toorthodontic treatment of preadolescents, adolescents, and adultsAm JOrthod Dentofacial Orthop 1991 100(4):349-56. [Google Scholar]
[8]. Tortamano A, Lenzi DC, Haddad ACSS, Bottino MC, Dominguez GC, Vigorito JW, Low-level laser therapy for pain caused by placement of the first orthodontic archwire: a randomized clinical trialAm J Orthod Dentofacial Orthop 2009 136(5):662-67. [Google Scholar]
[9]. Eslamian L, Borzabadi-Farahani A, Hassanzadeh-Azhiri A, Badiee MR, Fekrazad R, The effect of 810-nm low-level laser therapy on pain caused by orthodontic elastomeric separatorsLasers Med Sci 2014 29(2):559-64. [Google Scholar]
[10]. Ngan P, Kess B, Wilson S, Perception of discomfort by patients undergoing orthodontic treatmentAm J Orthod Dentofacial Orthop 1989 96(1):47-53. [Google Scholar]
[11]. Bondemark L, Fredriksson K, Ilros S, Separation effect and perception of pain anddiscomfort from two types of orthodontic separatorsWorld J Orthod 2004 5(2) [Google Scholar]
[12]. Asiry MA, Albarakati SF, Al-Marwan MS, Al-Shammari RR, Perception of pain and discomfort from elastomeric separators in Saudi adolescentsSaudi Med J 2014 35(5):504-07. [Google Scholar]
[13]. Artes-Ribas M, Arnabat-Dominguez J, Puigdollers A, Analgesic effect of a low-level laser therapy (830 nm) in early orthodontic treatmentLasers Med Sci 2013 28(1):335-41. [Google Scholar]
[14]. Kim WT, Bayome M, Park JB, Park JH, Baek SH, Kook YA, Effect of frequent laser irradiation on orthodontic pain. A single-blind randomized clinical trialAngle Orthod 2013 83(4):611-16. [Google Scholar]
[15]. Barbosa KGN, Sampaio TPD, Rebouças PRM, Catão MHCdV, Pereira JV, Gomes DQdC, Analgesia during orthodontic treatment with low intensity laser: systematic reviewRev Dor 2013 14(2):137-41. [Google Scholar]
[16]. Bertolini A, Ferrari A, Ottani A, Guerzoni S, Tacchi R, Leone S, Paracetamol: new vistas of an old drugCNS Drug Rev 2006 12(3-4):250-75. [Google Scholar]
[17]. Asnaashari M, Mohebi S, Paymanpour P, Pain reduction using low level laser irradiation in single-visit endodontic treatmentJ Lasers Med Sci 2011 2(4):139 [Google Scholar]
[18]. Ferrante M, Petrini M, Trentini P, Perfetti G, Spoto G, Effect of low-level laser therapy after extraction of impacted lower third molarsJ Lasers Med Sci 2013 28(3):845-49. [Google Scholar]
[19]. Esper MA, Nicolau RA, Arisawa EA, The effect of two phototherapy protocols on pain control in orthodontic procedure—a preliminary clinical studyLasers Med Sci 2011 26(5):657-63. [Google Scholar]
[20]. Farias RD, Closs LQ, Miguens Jr SAQ, Evaluation of the use of low-level laser therapy in pain control in orthodontic patients: A randomized split-mouth clinical trialAngle Orthod 2016 86(2):193-98. [Google Scholar]
[21]. Turhani D, Scheriau M, Kapral D, Benesch T, Jonke E, Bantleon HP, Pain relief by single low-level laser irradiation in orthodontic patients undergoing fixed appliance therapyAm J Orthod Dentofacial Orthop 2006 130(3):371-77. [Google Scholar]
[22]. Walsh L, The current status of low level laser therapy in dentistry, Part 1. Soft tissue applicationsAust Dent J 1997 42(4):247-54. [Google Scholar]
[23]. Parker S, Verifiable CPD paper: laser-tissue interactionBr Dent J 2007 202(2):73-81. [Google Scholar]
[24]. Convissar RA, Principles and Practice in Laser Dentistry 2011 1st edSt. Louis, MoMosby Elsevier [Google Scholar]
[25]. Kawasaki K, Shimizu N, Effects of low-energy laser irradiation on bone remodeling during experimental tooth movement in ratsLasers Surg Med 2000 26(3):282-91. [Google Scholar]
[26]. Lim H-M, Lew KK, Tay DK, A clinical investigation of the efficacy of low level laser therapy in reducing orthodontic postadjustment painAm J Orthod Dentofacial Orthop 1995 108(6):614-22. [Google Scholar]
[27]. Nobrega C, da Silva EM, de Macedo CR, Low-level laser therapy for treatment of pain associated with orthodontic elastomeric separator placement: a placebo-controlled randomized double-blind clinical trialPhotomed Laser Surg 2013 31(1):10-16. [Google Scholar]
[28]. Marini I, Bartolucci ML, Bortolotti F, Innocenti G, Gatto MR, Alessandri Bonetti G, The effect of diode superpulsed low-level laser therapy on experimental orthodontic pain caused by elastomeric separators: a randomized controlled clinical trialLasers Med Sci 2015 30(1):35-41. [Google Scholar]
[29]. Furquim RD, Pascotto RC, Rino Neto J, Cardoso JR, Ramos AL, Low-level laser therapy effects on pain perception related to the use of orthodontic elastomeric separatorsDental Press J Orthod 2015 20(3):37-42. [Google Scholar]
[30]. Bjordal JM, Johnson MI, Iversen V, Aimbire F, Lopes-Martins RAB, Low-level laser therapy in acute pain: a systematic review of possible mechanisms of action and clinical effects in randomized placebo-controlled trialsPhotomed Laser Ther 2006 24(2):158-68. [Google Scholar]
[31]. Hujoel PP, DeRouen T, Validity issues in split-mouth trialsJ Clin Periodontol 1992 19(9):625-27. [Google Scholar]
[32]. Chetruș V, Roman I, Ciobanu S, Early diagnosis of acute diffuse pulpitis, treatment successRom J Oral Rehabil 2014 6(1) [Google Scholar]
[33]. Abtahi SM, Mousavi SA, Shafaee H, Tanbakuchi B, Effect of low-level laser therapy on dental pain induced by separator force in orthodontic treatmentDent Res J (Isfahan) 2013 10(5):647-51. [Google Scholar]
[34]. Erdinç AME, Dinçer B, Perception of pain during orthodontic treatment with fixed appliancesEur J Orthod 2004 26(1):79-85. [Google Scholar]
[35]. Singla R, Singla N, Pain Perception Due To Orthodontic Separator With And Without Diclofenac MouthwashJInt Acad Res Multidiscip 2014 2(2):475-86. [Google Scholar]
[36]. Fujiyama K, Deguchi T, Murakami T, Fujii A, Kushima K, Takano-Yamamoto T, Clinical effect of CO(2) laser in reducing pain in orthodonticsAngle Orthod 2008 78(2):299-303. [Google Scholar]