The human Occipital Condyle (OC) is the distinctive bony structure linking the skull and the vertebral column [1]. The OC partly cover the fringe of the foramen magnum anteriorly and form an articulation with the superior articular facets on the lateral masses of the atlas inferiorly. Each OC which is oval in outline and oriented obliquely is traversed by hypoglossal canal. A condylar fossa is situated just posterior to the OC and can contain a posterior condylar canal for an emissary vein from the sigmoid sinus. Laterally, the occipital bone connects with the petrous part of the temporal bone anteriorly and the mastoid process posteriorly [2].
During interventional operations; the direction, angle and position of the nail may change according to the OC morphometry and the difference in measurements may alter the surgical procedure [3]. Occipital plates are frequently utilized during occipitocervical fixation but the complex anatomy of the craniocervical junction poses challenge during these procedures [4]. The surgical mistakes in this region may damage the neuro-vascular structure and result in craniocervical instability. Further, the management of ventrally placed space-occupying lesion at the level of foramen magnum necessitates the use of dorsal approach as high rate of morbidity and complications are frequently linked with ventral approaches. This requires transcondylar approach demanding partial resection of the OC which is a vital step for entrance to the ventral and ventrolateral foramen magnum [1]. Hence, the surgical instrumentation of the craniovertebral region necessitates a thorough anatomical knowledge of the OC.
Differences exist in OC morphometric values across different study populations. So far, out of the studies available, few determine the morphometry of OC, especially in the Indian population [1,3–16]. The present study quantified morphometric characteristics of the OC which are mandatory for safe screw placement during surgical instrumentation of this region.
Materials and Methods
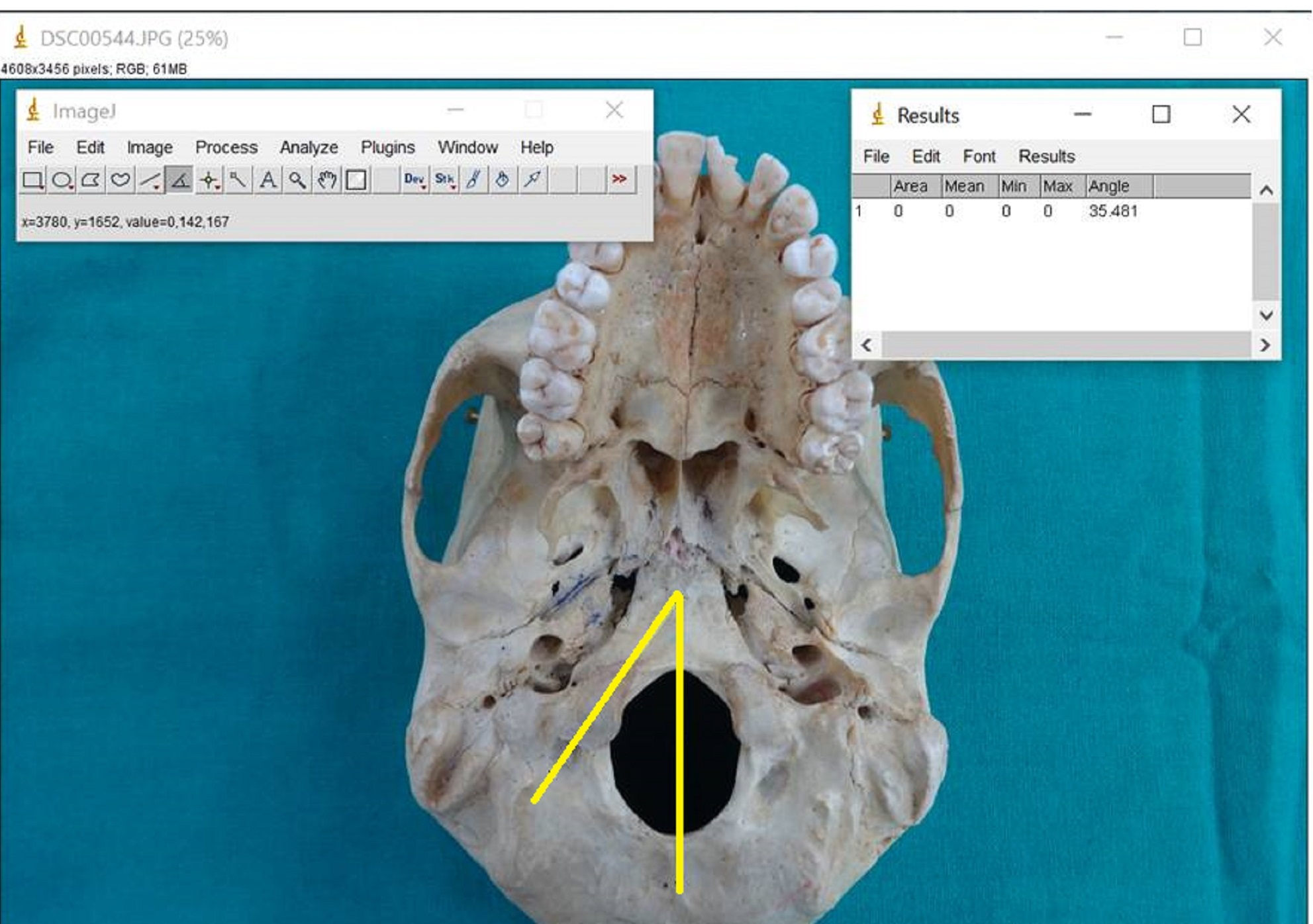
The present study included 228 OC of 114 adult human skulls of unknown sex which were part of the osteological collection of the Department of Anatomy. The study commenced in July, 2015 and accomplished in May, 2016. Skulls that were damaged or those with deformities, which may influence measurements, were excluded from the study and only intact skulls in good condition were studied. All linear measurements were ascertained using digital Vernier’s Calliper with 0.01mm precision while angular measurements were recorded with software Image J. [Table/Fig-1] demonstrates methodology of angle measurement.
Methodology of angle measurement with software Image J.
The following morphometric parameters were studied and analysed:
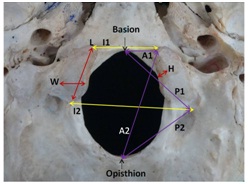
1. Linear Parameters [Table/Fig-2]
Inferior view of base of skull showing; (L)- Length of OC; (W)- Width of OC; (H)- Height of OC; (I1)- Anterior intercondylar distance; (I2)- Posterior intercondylar distance; (A1)- Distance between the anterior tip of occipital condyle and basion; (A2)- Distance between the anterior tip of occipital condyle and opisthion; (P1)- Distance between the posterior tip of occipital condyle and basion; (P2)- Distance between the posterior tip of occipital condyle and opisthion
Length of OC: Maximum anteroposterior distance between anterior and posterior tips of OC.
Width of OC: Maximum transverse distance between medial and lateral border of OC.
Height of OC: Maximum vertical distance between upper and lower border of medial margin of OC.
Anterior Intercondylar Distance (AICD): Distance between anterior tips of right and left OC.
Posterior Intercondylar Distance (PICD): Distance between posterior tips of right and left OC.
Distance between the anterior tip of Right OC and Basion (Right AOCB)
Distance between the anterior tip of Left OC and Basion (Left AOCB)
Distance between the anterior tip of Right OC and Opisthion (Right AOCO)
Distance between the anterior tip of Left OC and Opisthion (Left AOCO)
Distance between the posterior tip of Right OC and Basion (Right POCB)
Distance between the posterior tip of Left OC and Basion (Left POCB)
Distance between the posterior tip of Right OC and Opisthion (Right POCO)
Distance between the posterior tip of Left OC and Opisthion (Left POCO)
2. Angular Parameters [Table/Fig-3]
Inferior view of base of skull showing; (S1)- Sagittal condylar angle; (S2)- Sagittal intercondylar angle.
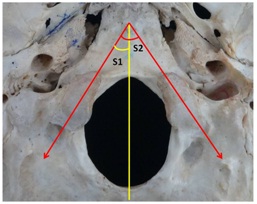
Sagittal Condylar Angle (SCA): The angle between OC axis and midline passing through basion and opisthion.
Sagittal Intercondylar Angle (SICA): The angle between the long axis of right and left OC.
Statistical Analysis
The mean and standard deviations of the linear and angular parameters were calculated. The comparison of morphometric dimensions of the right and left sides was performed using Student’s t-test and p-value was calculated.
Results
1. Linear Parameters: Mean length and width of the OC were 22.75±2.90mm and 12.97±1.53mm respectively, while mean height was found to be 9.21±1.22mm. These dimensions of the OC were comparable on both the sides.
Anterior and posterior intercondylar distances were noted to be 17.81±2.93mm and 38.91±4.16mm respectively.
The distance between Anterior Tip of OC (AOC) and basion was 9.65±1.56mm while the distance between AOC and opisthion was 37.70±2.37mm. Mean distance between Posterior Tip of OC (POC) and opisthion was observed to be 26.48±2.24mm and there was no significant difference among these parameters on both the sides. But the distance between POC and basion was observed to be 27.54±2.81mm and it was significantly greater on the right side (p-value= 0.01).
[Table/Fig-4] summarizes the mean and standard deviation of each linear parameter.
Linear parameters of occipital condyle.
| Parameters | Range(Min-Max)(mm) | Mean(mm) | StandardDeviation | Significance(p-value) |
|---|
| Occipital Condyle | Length | Right | 16.61-27.88 | 22.90 | 3.11 | 0.41 |
| Left | 17.89-29.27 | 22.60 | 2.72 |
| Mean | 16.61-29.27 | 22.75 | 2.90 |
| Width | Right | 10.89-16.39 | 12.98 | 1.62 | 0.97 |
| Left | 10.51-15.88 | 12.97 | 1.46 |
| Mean | 10.51-16.39 | 12.97 | 1.53 |
| Height | Right | 6.02-11.85 | 9.32 | 1.23 | 0.12 |
| Left | 6.35-11.16 | 9.12 | 1.23 |
| Mean | 6.02-11.85 | 9.21 | 1.22 |
| Anterior Intercondylar Distance | 12.68-26.82 | 17.81 | 2.93 | - |
| Posterior Intercondylar Distance | 27.62-49.58 | 38.91 | 4.16 | - |
| Distance between AOC & Basion | Right | 6.37-15.39 | 9.74 | 1.78 | 0.41 |
| Left | 6.55-12.9 | 9.56 | 1.33 |
| Mean | 6.37-15.39 | 9.65 | 1.56 |
| Distance between AOC & Opisthion | Right | 33.72-43.92 | 37.53 | 2.26 | 0.43 |
| Left | 33.32-43 | 37.88 | 2.5 |
| Mean | 33.32-43.92 | 37.70 | 2.37 |
| Distance between POC & Basion | Right | 22.08-39.35 | 28.16 | 3.26 | 0.01 |
| Left | 23.32-32.16 | 26.93 | 2.16 |
| Mean | 22.08-39.35 | 27.54 | 2.81 |
| Distance between POC & Opisthion | Right | 22.26-31.14 | 26.78 | 1.92 | 0.19 |
| Left | 21.42-33.64 | 26.17 | 2.51 |
| Mean | 21.42-33.64 | 26.48 | 2.24 |
2. Angular Parameters: Mean sagittal condylar angle was noted to be 42.57°±4.48 and it was significantly larger on the left side (p-value= 0.001). Mean sagittal intercondylar angle was observed to be 87.97°±8.75 [Table/Fig-5].
Angular parameters of occipital condyle.
| Parameters | Range(Min-Max) (degrees) | Mean (degrees) | Standard Deviation | Significance (p-value) |
|---|
| Sagittal Condylar Angle | Right | 33.27-53.52 | 41.10 | 4.45 | 0.001 |
| Left | 37.21-53.77 | 44.04 | 4.07 |
| Mean | 33.27-53.77 | 42.57 | 4.48 |
| Sagittal Intercondylar Angle | 71.47-109.21 | 87.97 | 8.75 | |
Discussion
Lesions of craniovertebral regions are presently managed by lateral approaches. Different forms of lateral approaches to this section have been illustrated, including transfacetal approach, the partial transcondylar approach, the complete transcondylar approach, the extreme-lateral transjugular approach and the transtubercular approach. Majority of these approaches demand resection of the OC partially or completely. The dimensions and orientation of the OC may influence the surgical approach to the lesions of craniovertebral junction [1,3,4].
Different investigators have reported variable morphometry of OC [1,3–13]. These variations may be due to different methods of data assimilation and genetic endowment of different populations. Most of the researchers conducted morphometry of OC in dry skulls, though a few investigators studied cadaveric specimens and CT scans which can yield variable results [1,3,4,6,7,10,12,13]. Similarly, morphometric analysis of the OC of different population can exhibit inconsistent values. In the present study we have endeavoured to analyze OC morphometry and provide a reference database for designing customized implants and screws for Indian population. Such data also allows for comparison with other study populations and enables identification of osteological remains, especially of Indian population.
In present study in Indian population, we found the mean length of OC to be 22.75 mm which was comparable to the findings of Lang J and Hornung G in German population (22.9 mm) and Bozbuga M et al., in Turkish population (23.1 mm) but Yu Z et al., in Chinese population (21.53 mm), Salih AM et al., in Sudanese population (20.66 mm) and Wen HT et al., in American population (21 mm) observed shorter length of OC [5–9]. Other researchers including Naderi S et al., Bozbuga M et al., Kizilkanat ED et al., in Turkish population, Dowd GC et al., in American population, Olivier GE in French population and Guidotti A in Italian population reported higher values than our findings [1,6,10–13] [Table/Fig-6]. The anatomical and biomechanical effects of partial condylectomy are different in long type and short type OC. Greater occipitocervical instability results in short OC with the same amount of partial condylectomy, whereas a long condyle may necessitate more widespread resection for optimum visualization [1].
Comparison of occipital condyle dimensions with previous studies [8,10].
| Researchers | Year | Population | Length (mm) | Width (mm) | Height (mm) |
|---|
| Present study | 2016 | Indian | 22.75 | 12.97 | 9.21 |
| Yu Z et al., [7] | 2014 | Chinese | 21.53 | - | - |
| Salih AM et al., [8] | 2014 | Sudanese | 20.66 | 12.81 | - |
| Ozer MA et al., [3] | 2011 | Turkish | 23.95 | 11.3 | - |
| Le TV et al., [4] | 2011 | American | 22.4 | 11.2 | 9.9 |
| Kizilkanat ED et al., [10] | 2006 | Turkish | 24.5 | 13.1 | - |
| Naderi S et al., [1] | 2005 | Turkish | 23.6 | 10.5 | 9.2 |
| Bozbuga M et al., [6] | 1999 | Turkish | 23.1 | 11.3 | - |
| Dowd GC et al., [11] | 1999 | American | 30 | - | - |
| Wen HT et al., [9] | 1997 | American | 21 | - | - |
| Lang J and Hornung G [5] | 1993 | German | 22.9 | - | - |
| Guidotti A [13] | 1984 | Italian | 23.7 | - | - |
| Olivier GE [12] | 1975 | French | 23.7 | 11.5 | 8.8 |
The mean OC width may engage similar surgical contemplations. In the present study, we found the mean width of OC to be 12.97 mm which was comparable to the finding of Salih AM et al., (12.81mm) in Sudanese population and Kizilkanat ED et al., (13.1mm) in Turkish population [Table/Fig-6]. Other researchers reported lesser values suggesting that OC of Indian population are wider [1,3,4,6,12]. Condylectomy in a wider condyle may be more challenging. The height of the OC is also a significant surgical issue. The greater height of OC may facilitate the successful screw placement during occipitocervical fixation. The mean height of the OC was noted to be 9.21 mm in Indian population which was analogous to the other populations [Table/Fig-6].
Anterior and Posterior intercondylar distances illustrate the orientation and convergence of OC which is essential prerequisite for screw placement during occipitocervical fixation. These parameters were found to be lesser in our study compared to other researchers [Table/Fig-7]. Shorter AICD and PICD may offer challenges during condylectomy by lateral approach.
Comparison of occipital condyle dimensions with previous studies.
| Researchers | AICD (mm) | PICD (mm) | AOCB (mm) | AOCO (mm) | POCB (mm) | POCO (mm) | SCA (degree) | SICA (degree) |
|---|
| Present study | 17.81 | 38.91 | 9.65 | 37.70 | 27.54 | 26.48 | 42.57 | 87.97 |
| Ozer MA et al., [3] | 20.9 | 43.1 | 11.4 | 40.5 | 29.4 | 29.5 | 35.5 | 68.7 |
| Le TV et al., [4] | - | - | - | - | - | - | 20.3 | - |
| Kizilkanat ED et al., [10] | 22.6 | 44.2 | - | - | - | - | 31.4 | 62.2 |
| Naderi S et al., [1] | 21.0 | 41.6 | 10.8 | 39.0 | 27.8 | 26.4 | 29.6 | 59.3 |
| Bozbuga M et al., [6] | - | 30.2 | - | - | - | 24.3 | 28.9 | 57.8 |
| Lang J and Hornung G [5] | - | - | - | - | - | - | - | 41.4 |
The distances between the tips of OC and opisthion and basion are also essential anatomical features. The AOCB and AOCO distances were noted shorter in our study than findings of Naderi S et al., and Ozer MA et al., [Table/Fig-7] [1,3]. However, the POCB and POCO distances were comparable to the findings of Naderi S et al., but shorter than those reported by Ozer MA et al., [Table/Fig-7] [1,3]. These values suggest that tips of OC are nearer to the median plane in Indian population which should be considered during application of screws in the OC. Awareness of these findings can prevent injury to the adjacent neurovascular structures.
Sagittal condylar angle and sagittal intercondylar angle constitute vital parameters for insertion of screws in the OC. We report higher values of these angles (SCA: 42.57°; SICA: 87.97°) compared to other researchers suggesting that OC of Indian population converge more ventrally [Table/Fig-7]. Wide SCA and SICA may provide additional space for posterolateral approach during condylectomy and may be more useful for reaching the foramen magnum [1]. Further these facts should be reckoned during placement of screws and plates in the OC.
Ultimately, the other Indian researchers found analogous results for length and height of the OC but other parameters were observed to be variable [14–16] [Table/Fig-8] displays the comparison between different Indian studies and provides a range of each parameter for Indians which should be considered during operative procedures of craniovertebral region.
Comparison of occipital condyle dimensions with other Indian studies.
| Parameters (mm) | Present study | Tale AK [14] | Sahoo S [15] | Kalthur SG [16] |
|---|
| Length of OC | 22.75 | 22.01 | 22.55 | 22 |
| Width of OC | 12.97 | 11.25 | 12.73 | 11 |
| Height of OC | 9.21 | 8.22 | - | 9 |
| AICD | 17.81 | 21.28 | 20.31 | 21 |
| PICD | 38.91 | 40.61 | 41.17 | 39 |
| AOCB | 9.65 | - | 11.03 | 12 |
| AOCO | 37.70 | - | - | 39 |
| POCB | 27.54 | - | - | 27 |
| POCO | 26.48 | - | 27.84 | 28 |
Limitation
We could not incorporate the morphometric parameters of adjacent structures due to the scrupulous nature of manual measurements of 228 OC by digital callipers, which require time and accurate positioning. Further studies are required on the morphometry of foramen magnum, hypoglossal canal, jugular formen and upper cervical vertebrae to complete the morphometric database for successful surgeries of craniovertebral region.
Conclusion
The present study yielded the characteristics of the Indian OC. We found the wider OC in Indians when compared to other populations. The intercondylar distances were found to be shorter and the tips of the OC were closer to the median plane suggestive of vigilant instrumentation of OC in Indian population. We observed the sagittal condylar angle and sagittal intercondylar angle to be wider in Indians. Hence, awareness of detailed morphometry of the OC can facilitate the successful instrumentation and minimize the neurovascular injuries. We anticipate that our study will be able to provide a reference database for designing implants and for planning the appropriate surgical approach in the OC.