Root canal treatment involves treating diseased dental pulp, so that patients retain natural teeth in function and aesthetics. Canal preparation is one of the major factors in determining the success of root canal therapy. Unfortunately, preparation of root canal is influenced by the highly complex anatomy and the inability of the clinician to identify this anatomy in a radiograph [1,2].
During shaping and cleaning of curved canals, occurence of iatrogenic errors such as ledges, zips, perforations, and root canal transportation is common [3].
The common factors responsible for canal transportation are: insufficiently designed access cavities, inflexible canal preparation instruments, instrumentation technique like crown down preparation using hand instruments, degree and radius of a canal curvature, unseen canal curvatures in two dimensional radiographs and experience of the operator [3].
Canal transportation is defined in the ‘American Association of Endodontists’ Glossary of Endodontic Terms as “the removal of canal wall structure on the outside curve in the apical half of the canal due to the tendency of files to restore themselves to their original linear shape during canal preparation” [4].
Mattison stated that the remaining strength of a tooth is directly related to the remaining bulk of dentin [5]. It is accepted that, greater the amount of residual dentin, the more predictable the longevity and strength of a tooth and its restoration. Hansen and Asmussen suggested that coronal flare with rotary canal preparation burs like Gates Glidden burs and subsequent canal instrumentation may result in further weakening of tooth structure [5,6].
When compared to hand instrumentation with files made of stainless steel, new generation of Ni-Ti rotary instruments such as ProTaper (PT), Mtwo and ProTaper NEXT (PTN) are designed to prepare rounder and tapered preparation, are more flexible and have superior resistance to torsional fracture. However, more aggressive preparation could produce canal transportation.
Manufacturers claim that PTN rotary files are best in shaping curved canals due to its specific design features. Currently less information is available regarding this rotary system.
To evaluate the maintenance of curvature post-instrumentation, a non-invasive technology in the form of 3-Dimensional Computed Tomography (3D-CT) imaging can be used. It renders cross-sectional (cut plane) 3D images that are remarkably accurate and quantifiable. This non-destructive technology has provided repeatable results. It has also allowed non-invasive experimentation of endodontic instrumentation of root canal. Without specimen loss the canal transportation can be viewed at any level in parameters like amount and direction of canal transportation [7]. Although this is an in-vitro study, a non-destructive method is considered in order to simulate clinical conditions.
There have been very few studies done to evaluate the canal transportation and volumetric change using Mtwo, PT, and PTN Ni-Ti instruments while maintaining the original shape of the root canal. Thus, the present study was set-up to comparatively evaluate the canal transportation and volumetric change of these three Ni-Ti Rotary instruments using CT.
Materials and Methods
This in-vitro study was undertaken in the Department of Conser-vative Dentistry and Endodontics, Bapuji Dental College and Hospital, Davangere, Karnataka, India. Ethical clearance was obtained from the institutional review board.
Permanent teeth with completely formed apices and teeth with similar characteristics of length (20mm-22mm) and mesio-buccal canal curvature (10°-35°) measured according to the criteria described by Schneider were included in the study [8]. Those teeth which were decayed, restored, calcified, teeth with resorptive defects, root canals with double curvatures and teeth with curvatures less than 10° were excluded from the study.
A total of 45 (15 mandibular and 30 maxillary roots) mesiobuccal root canals of extracted maxillary and mandibular first molar teeth were used. The teeth were stored in 10% buffered formalin. Access cavity was prepared by using an airotor handpiece (NSK) and access preparation kit (DENTSPLY). Distobuccal and palatal roots of maxillary and distal roots of all mandibular teeth were separated by using diamond disc at the furcation. Specimens were divided as shown in [Table/Fig-1]. To determine the working length, a size 10 K-file was placed into the canal until it was visible at the apical foramen and Working Length (WL) was established 0.5mm short of this length. For standardization, the crown was flattened with diamond disk to obtain a final WL of 16mm for each specimen. A glide path was created using a size 15 K-file [9]. The roots were positioned in a custom-made specimen holder (Specimens were arranged on a wax sheet and numbered, supported by paper cardboard sheet) and were randomly divided into three experimental groups containing 15 teeth each. All specimens were covered in a single exposure.
Division of study groups.
| Study Groups | Number of root canals/teeth | Files used | Final finishing done with |
|---|
| Group I | 15 | Mtwo | 25/0.06 taper to WL |
| Group II | 15 | ProTaper | 25/0.08 F2 to WL |
| Group III | 15 | ProTaper NEXT | 25/0.06x2 to WL |
WL-Working Lenth
All the groups were scanned by CT (Toshiba Activion 16 Slice MDCT) pre-operatively with high resolution supplied by the CT scanner, at 120 KV and 50mA, 512×512 pixels matrix, 0.5mm-thick axial sections, 32cm display field of view, and beam incidence at the central portion on the device was used to fix the specimens to determine the root canal shape before instrumentation. The sections were taken at three levels. Sections at 3mm, 7mm and 11mm from the apical end of the root were recorded. After initial scan, root canals were instrumented using standard techniques.
In all the groups, canals were instrumented with crown-down technique, torque and rotational speed was used according to the manufacturer’s recommendation. For all the groups after the use of each file, canals were irrigated with 3ml of 2.5% sodium hypochlorite (NaOCl) as an irrigant during instrumentation and when root canal instrumentation was completed, 1ml of 17% EDTA was used for 1minute followed by a final flush of 3ml NaOCl. Teeth were then scanned under the same condition as the initial scan. Data were recorded.
FORMULA FOR THE DETERMINATION OF CANAL TRANS-PORTATION AND VOLUMETRIC CHANGES
Evaluation of Canal Transportation: The canal transportation that occurred during shaping and cleaning was determined by measuring the shortest distance from the edge of instrumented and uninstrumented canal to the periphery of the root (mesial and distal) and then comparing these measurements. A mean value was calculated from all measurements [Table/Fig-2].
Image cross sections for measurements.
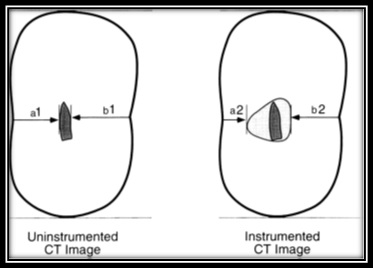
The formula used for the calculation of root canal transportation [8]:
(a1– a2) - (b1– b2),
Where, a1 is the shortest distance from the mesial edge of the root to the mesial edge of the uninstrumented canal, b1 is the shortest distance from distal edge of the root to the distal edge of the uninstrumented canal, a2 is the shortest distance from the mesial edge of the root to the mesial edge of the instrumented canal and b2 is the shortest distance from distal edge of the root to the distal edge of the instrumented canal.
With the above formula, following interpretation is done [8]:
0 – indicates no canal transportation
Value other than 0 indicates transportation has occurred in the canal
Negative value indicates transportation towards distal
Positive value indicates transportation towards mesial
Volumetric Measurements: Mesio-buccal canal in each specimen was traced before and after instrumentation. The 3D scanned images were used in the Osirix software to manually mark points following the outline of the canal. The software then provides the volume of the area marked. The volume of removed dentin was determined in mm3 for each root canal by subtracting the un-instrumented canal volume from the instrumented canal volume.
Canal transportation between and within the groups, before and after instrumentation, was analyzed using ANOVA. Volumetric changes between and within the groups, before and after instrumentation, was analyzed using paired t test.
Results
[Table/Fig-3] provides the values of canal transportation at 3mm, 7mm and 11mm. When analyzed statistically, there was no significant difference within and between groups in relation to Mtwo, PT and PTN.
Analysis of canal transportation between and within groups using ANOVA.
| 3mm | 7mm | 11mm | F | p-value |
|---|
| Mean | SD | Mean | SD | Mean | SD | - | - |
|---|
| Mtwo | 0.0033 | 0.01363 | -0.0153 | 0.04818 | 0.0085 | 0.01524 | 2.556 | 0.090 |
| ProTaper | 0.0046 | 0.01248 | 0.0049 | 0.00892 | 0.0057 | 0.02695 | 0.014 | 0.986 |
| ProTaper NEXT | -0.0021 | 0.02252 | 0.0013 | 0.01233 | 0.0060 | 0.01580 | 0.825 | 0.445 |
| F | 0.674 | 2.037 | 0.087 | - | - |
| p-value | 0.515 | 0.143 | 0.917 | - | - |
Mtwo showed negative mean at 7mm and was found to promote canal transportation in the distal surface of the canal curvature. The PT was found to promote higher amount of canal transportation on mesial surface at 11mm. The PTN was found to promote canal transportation on the distal surface of canal curvature at 3mm.
[Table/Fig-4,5] provide values of volume differences within and between the groups respectively.
Analysis of volume difference within groups using paired t test.
| Study Groups | N | Mean | SD | T | p | 95% Confidence Interval |
|---|
| Mtwo | Before | 15 | 0.033 | 0.007 | -9.02 | 0.000 | -0.013 | -0.008 |
| After | 15 | 0.044 | 0.006 |
| ProTaper | Before | 15 | 0.340 | 0.005 | -7.24 | 0.000 | -0.012 | -0.007 |
| After | 15 | 0.440 | 0.006 |
| ProTaper NEXT | Before | 15 | 0.320 | 0.067 | -12.47 | 0.000 | -0.013 | -0.009 |
| After | 15 | 0.433 | 0.004 |
Analysis of volume difference between groups using paired t test.
| N | Mean | SD | F | p |
|---|
| Mtwo | 15 | 0.0103 | 0.00321 | 0.323 | 0.726 |
| ProTaper | 15 | 0.0109 | 0.00535 |
| ProTaper NEXT | 15 | 0.0107 | 0.00458 |
The amount of volume removed was comparatively more in case of PT (Mean: 0.0109 mm3) and PTN (Mean: 0.0107 mm3) when compared to Mtwo (Mean: 0.0103 mm3) but there was no statistically significant difference found.
There was a statistically significant difference in volumetric changes within the groups.
Discussion
Shaping and cleaning of the root canal can be best accomplished by preparing tapered canal from the apical to the coronal area; thereby, the original general shape of the canal is preserved. Mechanical debridement includes use of hand files or rotary files.
Root canal instruments were manufactured of carbon steel till 1960, which was later replaced by stainless steel alloys [10]. These traditional hand instruments often failed in achieving schielders mechanical objective of maintaining the original canal curvature because of their increasing stiffness with increase in size [11]. Because of this, they resulted in procedural errors like ledges, perforation, zips and elbows. Many instruments, devices and instrumentation techniques have been recommended but only few seem to be capable of consistently achieving these primary objectives of root canal preparation. Rotary Ni-Ti instruments differ in size, taper and the sequence of use. The manufacturer’s aim in designing these Ni-Ti files was to achieve better debridement and greater apical size with fewer files and errors [12].
Rotary Ni-Ti instruments have been recommended to be used in crown down instrumentation sequence, in which larger one is preceded by smaller ones, from coronal to apical end. The amount of canal transportation increases with apical preparation greater than size 25 according to Buchanan. Hence, the apical preparation was limited to size 25 K-file in the present study [13]. Irrespective of the instrumentation technique, shaping and cleaning procedures leads to dentine removal from the canal walls [9].
Extracted teeth were used in the present study, since they provide conditions that closely mimic clinical situations [9]. Mesiobuccal root canals of first molar teeth were selected because they usually present with accentuated curvature and mesio-distal flattening. These flat shapes are more predominant than oval and the round shapes are scarce. During chemo-mechanical preparation, these characteristics are additional difficulties for predictable cleaning and shaping of canals [14,15]. It was reported that the characteristics of these mesiobuccal canals allow for clinical instrumentation with techniques, designed for curved canals. Second mesiobuccal canals were not included because they were not suitable since they did not continue as separate canals along the root and has extreme anatomic variations [16]. In the present study, distal and palatal root of the teeth were separated at the furcation and discarded. This was done in order to place the specimens as close as possible to the X-ray source of the CT unit and for more accurate measurements [14,17].
Like in other studies Schneider method was used to determine root canal curvature [14] which was an effective method in evaluating the root canal curvature. In the present study moderate canal curvatures 10°-35° according to the criteria described by Schneider (1971) has been used [18]. This was done by using Radio-Visio-Grapgy (RVG) and Image J software.
This wide degree of canal curvature is selected in order to evaluate canal transportation and the amount of dentin removed during instrumentation. The direction of transportation in the apical area is mainly related to the degree of curvature, it also depends on the instrument design, the physical properties of the alloy and the techniques of instrumentation [19].
For standardization, all teeth were shortened to a length of 16 mm; thus, several parameters usually found in the in-vivo situation (e.g., complicated access to cavity, greater length of root canals, etc.) could not be simulated, this may have an effect on the final results. Three levels (i.e., 3mm, 7mm, 11mm from the root apex) were chosen representing the coronal, middle and apical thirds of the mesiobuccal root canals wherein the curvatures usually exist and are highly susceptible to iatrogenic mishaps [20]. In the present study, all root canals were uniformly prepared to size 25 with different taper; this was to maintain the uniformity in apical preparation size of 25 for all the three rotary system, and also studies have shown that preparation to size 25 is exceptionally safe in all canals. The size of the taper is a major factor involved in apical root transportation because as taper increases the instrument flexibility decreases.
Compared with other rotary Ni-Ti files, instrumentation time with Mtwo instruments were substantially faster than with all other rotary Ni-Ti instruments tested under identical experimental conditions [21].
In this in-vitro study three rotary Ni-Ti systems: Mtwo, PT and PTN have been used. The instruments selected in this study are different in several factors that make them different from other systems, such as manufacturing processes and different cutting profiles.
The canal transportation was calculated using a technique developed by Gambill JM et al., [8] since this technique is similar to Bramante’s technique without actually cutting the sample [7]. There are various methods of determining canal transportation like radiographic imaging, cross sectioning, CT, Micro-CT and Cone Beam Computed Tomography (CBCT) [22,23].
The methods used earlier comprised of radiographic imaging cross-sectioning and longitudinal cleavage of the samples. The latter methods might lead to sample loss [23]. Recently, CT, Micro- CT and CBCT have been added as measuring devices for the same. These methods have given acceptable and reproducible results by virtue of their non-destructive nature and possibility to have precise linear measurements [24]. They also measure the volume of dentin removed after instrumentation [11].
Mtwo showed a reduced tendency for canal transportation. This is in agreement with previous studies, which found that Mtwo files maintained the original canal curvature well both in simulated canals and in real canals of extracted teeth [7].
In present in-vitro study, in terms of volume, PT removed dentin more than PTN and Mtwo. This is in accordance with several other studies that have surveyed canal preparation with the PT rotary instrument [16]. These studies have yielded controversial results in relation to canal transportation due to preparation with the PT system. According to a study done by Ozer et al., there was no statistically significant difference in canal transportation between PT and Hero 642. In addition, studies have also shown that canal transportation of the PT files was more than that with the RaCe files [25]. However, the extent of transportation with the PT system is similar to that with the RaCe system according to Guelzow et al., [16]. In summary, based on studies comparing PT with other instruments, PT system has shown to result in the greatest amount of canal transportation. But it is also seen that, PT rotary system when combined with the PathFiles reduce the extent of this transportation [14]. The PT instruments are designed to have a convex triangular cross-sectional design, three cutting edges with a negative cutting angle, a non-cutting modified safety tip and a flute design that combines progressive tapers within the shaft [22].
Caper has stated that, newly manufactured rotary systems with size 25 and a taper of 0.06 (PTN) or 0.08 (PT universal) could be used in curved canals because of minimal transportation [22]. Jain D, et al., concluded that canal transportation was more in case of PTN when compared with Revo s and one shape file system [26].
In the present study, PTN has shown less canal transportation when compared to PT and is not statistically significant. The probable reason for increased canal transportation with PT would be the progressive taper of the file, 3 point contact of the file to the canal wall when compared to PTN which has lesser taper and 2 point contact (Offset design) to the canal wall, as per the design characteristics of the file systems.
The other parameter assessed is the volumetric measurements before and after instrumentation.
The mesiobuccal canal in each specimen was traced before and after instrumentation, and the total volume was measured. The volume of removed dentin was determined in mm3 for each root canal. Volumetric measurements were taken by using Osirix software. However, there is no statistical significant difference between all the three systems (p>0.05) [24]. This may be due to variable taper of the PT.
In this study root canals were shaped with minimum errors. This is in agreement with previous studies that showed that more recent rotary systems shaped curved root canals without significant shaping errors [14].
As per an in-vitro study done by Gluskin et al., the volume of dentin removed at the coronal portion of root canals after Mtwo, PT, PTN instrumentation techniques were compared, and no difference was found between these instrument systems [24] PT recorded significantly more tooth structure removal than Mtwo, PTN as previously reported [27].
The volume of dentin removed was more with PT and PTN when compared to Mtwo. This may be due to variable taper and glide path created prior to the use of these file systems. The null hypothesis is accepted in the study.
Limitation
The present study has its limitations in the form of not completely mimicking clinical situations. Hence, more in-vivo studies can be done in this field. The present study also throws light on facts that a proper glide path and less aggressive instrumentation of root canals results in maintaining the original root canal curvature thus, satisfying Schilder’s mechanical objective of root canal preparation.
Conclusion
Within the limitations of this in-vitro study the following conclusions were drawn from the results of this study. All the three file systems have removed tooth structure and canal transportation has occurred in both mesial and distal directions. But it is not statistically significant. Clinically this finding is more important because less canal transportation, reduced amount of dentin removal and three dimensional obturation of the root canal are considered as the main keys for the success of endodontic treatment. However, more studies evaluating the canal transportation and volume of dentin removed using Micro CT and CBCT are desirable to further substantiate the findings of our study.
WL-Working Lenth