Spectrum of MDCT Findings in Bowel Obstruction in a Tertiary Care Rural Hospital in Northern India
Ranjana Gupta1, Puneet Mittal2, Amit Mittal3, Sharad Gupta4, Kapish Mittal5, Arpit Taneja6
1 Associate Professor, Department of Radiodiagnosis, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
2 Associate Professor, Department of Radiodiagnosis, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
3 Professor and Head, Department of Radiodiagnosis, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
4 Resident, Department of Radiodiagnosis, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
5 Resident, Department of Radiodiagnosis, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
6 Resident, Department of Radiodiagnosis, Maharishi Markandeshwar Institute of Medical Sciences and Research, Mullana, Ambala, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Puneet Mittal, F-9, Residential Complex, MM University, Mullana, Ambala, Haryana, India.
E-mail: drpuneetmittal@gmail.com
Introduction
Multidetector Computed Tomography (MDCT) provides clinically and surgically important information in bowel obstruction. It can depict the severity, level and cause of obstruction.
Aim
To depict the spectrum of MDCT findings in cases of small and large bowel obstruction.
Materials and Methods
Contrast enhanced MDCT examination of 50 patients were retrospectively included in the study who had evidence of clinical as well as MDCT evidence of bowel obstruction and in whom surgical/clinical follow-up for final diagnosis was available. CT scan was done in all the patients with Ingenuity CT (128 slice MDCT, Philips Medical Systems). The axial sections were reconstructed in coronal and sagital planes to determine site and cause of bowel obstruction.
Results
There were 34 males and 16 females patients in this study with mean age of 28.4 years. The level of obstruction was in small bowel in 39 patients (76.67%) and large bowel in 11 patients (23.33%). Adhesive bands were the cause of Small Bowel Obstruction (SBO) in 17 patients (43.5% of SBO patients). The most common CT signs in adhesive band SBO were beak sign (seen in 70.6% patients) and fat notch sign (52.9% patients). Five cases of SBO were secondary to benign stricture. Matted adhesions were the cause of obstruction in 3 patients. All these patients showed transition zone in pelvis with positive small bowel faeces sign. Two patients with SBO due to adhesive band had evidence of closed loop obstruction with evidence of gangrenous gut on surgery. Large Bowel Obstruction (LBO) was seen in 11 patients. Most common cause of LBO was primary colonic malignancy, accounting for 7 patients (63.6%). In one patient, the cause was direct invasion of hepatic flexure by carcinoma of gall bladder. Other causes of LBO were pelvic adhesions, faecal impaction and ischaemic stricture.
Conclusion
SBO is more common than LBO with adhesive bands being the most common cause of SBO. MDCT is very useful for depicting site and cause of obstruction and any associated complications.
Adhesive band, Closed loop, Ischaemia, Transition zone
Introduction
Bowel obstruction is one of the most common non-traumatic abdominal emergencies encountered in surgical practice, accounting for approximately 20% of surgical admissions for acute abdominal conditions with small bowel being involved in 60-80% of cases [1].
Diagnosis of bowel obstruction is based on clinical signs, patient history and radiographic findings, however for deciding appropriate management, further cross-sectional imaging with Ultrasound (USG) and Computed Tomography (CT) is frequently requested. Diagnostic value of CT in management of intestinal obstruction is well documented in literature [2–4]. CT imaging can be performed rapidly, even in unstable patients and is useful to demonstrate the level and cause of obstruction and any associated complications [2].
With the advent of Multi Detector CT (MDCT), CT can provide nearly isotropic imaging with reconstruction of images in any planes. Due to high spatial resolution and real time reconstruction in any plane, it is particularly helpful in locating the zone of transition and many times can directly depict the cause of obstruction. The cause of obstruction can have important implications in management, particularly closed loop obstructions and associated features of bowel ischaemia or gangrene may need early surgical management. On the other hand, in cases of malignant obstruction, treatment is based on the stage of the disease and extent and level of obstruction. Thus MDCT is very helpful for deciding the management in cases of bowel obstruction [5].
Aim
To depict the spectrum of MDCT findings in cases of small and large bowel obstruction.
Materials and Methods
The present study was conducted in Radiodiagnosis Department of Maharishi Markandeshwar Institute of Medial Sciences and Research, Ambala. Study was approved by the ethical committee. Contrast enhanced MDCT examinations of a total of 50 patients from January 2014 to September 2015 were retrospectively included in the study who had evidence of clinical as well as MDCT evidence of bowel obstruction and in whom surgical/clinical follow-up for final diagnosis was available. CT examinations were selected from departmental Picture Archiving and Communication System (PACS). CT scan was done in all the patients with Ingenuity CT (128 slice MDCT, Philips Medical Systems). Scanning was done using a pitch of 0.797, collimation of 64 X 0.625 with multiplanar reconstruction. Factors selected were 120 kV and 300 mAS. Contrast enhanced CT scan of abdomen was obtained after intravenous administration of 80-100ml of non-ionic contrast (Iohexol) containing 300mg/ml of iodine as a single bolus and CT was done in a single breath hold or in quite respiration if patient could not hold his/her breath. Study was done with positive or neutral oral contrast depending upon clinical condition. The axial sections were reconstructed in coronal and sagittal planes to determine site and cause of bowel obstruction.
Results
There were 34 males and 16 females patients in this study. The mean age was 28.4 years (range 4-74 years). Based on the MDCT findings, the level of obstruction was in small bowel in 39 patients (78%) and large bowel in 11 patients (22%). Causes of small bowel obstruction are as shown in [Table/Fig-1]. Adhesive bands were the cause of small bowel obstruction (SBO) in 17 patients (43.5% of SBO patients) MDCT was able to show the site of transition confidently in all subjects and to rule out bowel thickening and any mass lesion. The most common CT signs were beak sign (seen in 70.6% patients) and fat notch sign (52.9% patients). Small bowel faeces sign just proximal to the site of obstruction was seen in six subjects (35.3%) and whirl sign was seen in four subjects (23.5%) [Table/Fig-2]. Five cases of SBO secondary to benign stricture on MDCT showed concentric mural thickening at the site of transition and increased vascularity in mesentery. Matted adhesions were the cause of obstruction in three patients. All these patients showed dilated small bowel loops with transitional zone in pelvis without any discrete single focal point of narrowing. Small bowel faeces sign was seen in all these patients. None of these cases showed closed loop obstruction or gangrene. Cocoon formation was seen in two patients. Hernias accounted for five of the patients, all of which were depicted well on MDCT. Malignant strictures (primary bowel malignancy in one and mesenteric metastatic deposits in one patient) were seen in two patients. Other rare causes of SBO included intussusception (two patients), mid-gut volvulus (one patient), annular pancreas (one patient) and endometriosis (one patient). Two patients with SBO had evidence of closed loop obstruction with evidence of gangrenous gut on surgery. In both, it was caused by adhesive band. The closed loop obstruction as well as gangrenous gut was well depicted on MDCT [Table/Fig-3,4 and 5]. Large bowel obstruction (LBO) was seen in 11 patients [Table/Fig-6]. Most common cause of LBO was primary colonic malignancy, accounting for seven patients (63.6%). In one patient, the cause was direct invasion of hepatic flexure by carcinoma of gall bladder. Other causes were pelvic adhesions, faecal impaction and ischaemic stricture [Table/Fig-7,8 and 9].
Showing causes of small bowel obstruction.
| Cause | Number of cases |
|---|
| Adhesive band | 17 |
| Benign stricture | 5 |
| External hernia | 4 |
| Matted adhesions | 3 |
| Coccon formation | 2 |
| Primary malignant stricture | 1 |
| Extrinsic compression by mesenteric metastasis | 1 |
| Internal hernia | 1 |
| Intussusception | 2 |
| Mid gut volvulus | 1 |
| Annular pancreas | 1 |
| Endometriosis | 1 |
| Total | 39 |
Showing CT findings in SBO due to adhesive bands.
| CT-findings | Number of cases |
|---|
| Fat notch sign | 8 |
| Beak sign | 12 |
| Small bowel faeces sign | 6 |
| Whirl sign | 4 |
| Closed loop obstruction | 2 |
| Gangrenous gut | 2 |
| Total | 17 |
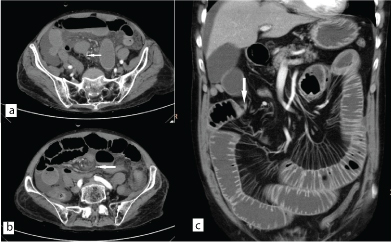
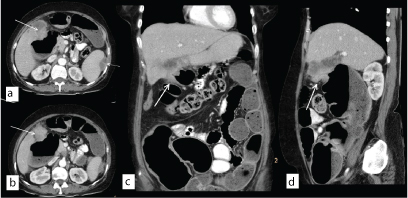
Axial CECT image (a) showing beak sign (white arrow) in a patient with SBO due to adhesive band with distal collapsed bowel. Axial section superior to it (b) shows twisting of mesentery (whirl sign) (white arrow in b). Coronal (c) CECT image of different patients showing fat notch sign due to adhesive band (white arrow).
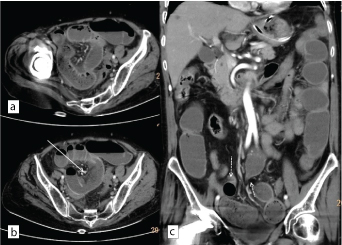
Axial CECT images (a&b) in case of closed loop obstruction showing dilated ileal loop with small bowel faces sign. Bowel gangrene is seen as evident by mural non-enhancement (white arrow in b). Coronal CECT image (c) showing adhesive band causing ileal obstruction at two levels (dotted white arrows).
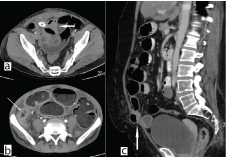
Axial CECT image (a) showing matted adhesions in the pelvis (white arrows). Note drainage catheter in pelvis. Axial CECT section (b) showing benign stricture of distal ileum with thickening and enhancement and increased vascularity in adjacent mesentery (white arrow). Note small bowel faeces sign. Sagittal (c) image showing herniated bowel loop through incisional hernia with SBO.
Showing causes of large bowel obstruction.
| Cause | Number of cases |
|---|
| Primary colon malignancy | 7 |
| Pelvic adhesions | 1 |
| Faceal impaction | 1 |
| Ischaemic stricture | 1 |
| Direct invasion by gall bladder carcinoma | 1 |
| Total | 11 |
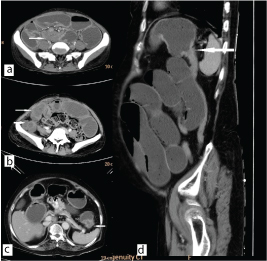
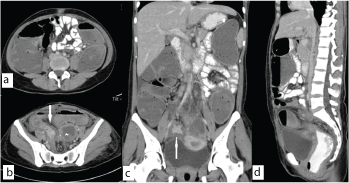
Axial CECT images showing SBO due to endometriosis (white arrow in a) and due to mesenteric deposits (white arrows in b). Note non-specific nature of mass in case of endometriosis which cannot be differentiated from primary or secondary tumors. Axial (c) and sagittal (d) images showing short segment splenic flexure growth with large bowel obstruction and distal collapsed descending colon (white arrows).
Axial (a&b), coronal (c) and sagittal (d) images showing gall bladder mass infiltrating into hepatic flexure with large bowel obstruction (white arrows). Note perisplenic necrotic deposits (dotted white arrow in a).
Axial (a&b), coronal (c) and sagittal (d) images showing large bowel obstruction with narrowing of sigmoid colon due to pelvic tubercular adhesions (white arrows). Note left tubo-ovarian abscess (star in b).
Discussion
Bowel obstruction is one of the common abdominal surgical emergencies which is frequently diagnosed on clinical and radiographic basis. CT has proven efficacy for confirming the obstruction and to look for site and cause of obstruction. Distinction of partial or complete bowel obstruction is often unreliable and difficult on CT, therefore, the primary focus should be to detect any associated complications which can affect clinical management [5]. CT can also help to exclude other causes of acute abdominal pain like pancreatitis, mesenteric ischaemia and bowel malignancies in which immediate surgery may not be indicated. With the advent of MDCT, true multiplanar imaging can be achieved without any blurring or loss of spatial resolution [6,7].
In present study, SBO was much more common than LBO, accounting for a total of 76.67% of cases. The most common cause of SBO is adhesive bands accounting for 43.5% of cases. Although adhesive bands are not directly visualized on CT, due to direct multiplanar imaging, sensitivity of MDCT for depiction of transition zone in these cases is nearly 100%. These are characterised by sudden transition at the site of obstruction without any mass lesion or bowel thickening. Various signs have been described for indirect depiction of adhesive bands. Most useful of these are beak sign (characterised by beak like narrowing at point of transition) and fat notch sign (characterised by focal fatty indentation at the site of transition) seen in 70.6% and 52.9% of patients, respectively.
When present, these signs can help in confident diagnosis of adhesive bands as the cause of SBO. Another useful sign is the twisting of the mesentery adjacent to the adhesive band (whirl sign) which was seen in 23.5% of the subjects. None of these signs were seen in SBO due to other causes. Small bowel faeces sign was seen in 35.3% of patients with adhesive bands however it was seen in all patients with matted adhesions, however this sign is not very helpful for differentiating the two [8,9]. Of much more clinical importance is the presence of closed loop obstruction which is characterised by obstruction at two levels with intervening dilated bowel which is at increased risk of ischaemia and gangrene. This type of obstruction is seen mostly in association with obstruction due to adhesive bands [8]. MDCT with multiplanar imaging can depict closed loop obstruction well. Moreover, lack of mural enhancement is indicative of bowel gangrene which is an indication for early surgical intervention. MDCT can readily depict bowel thickening and mesenteric inflammation, lymph nodes and deposits in benign and malignant strictures. Benign strictures are most commonly secondary to tuberculosis and Crohns disease. MDCT is useful for depicting features of active inflammatory changes like mural enhancement, mesenteric stranding and increased vascularity, however absence of such changes may not exclude active inflammation [5]. Malignant strictures are relatively rare causes of SBO and can be primary or secondary to metastatic disease. External hernias which were earlier most common cause of SBO are seen less frequently now. They are usually diagnosed clinically and MDCT also depicts them well.
There was one subject of internal hernia in our study which was diagnosed on MDCT. Cocoon formation as cause of SBO was seen in two patients which is seen as thick fibrous encapsulating peritoneal thickening encasing the small bowel loops, both of them were secondary to tuberculosis. Other causes of cocoon formation can be post-surgical and secondary to prolonged dialysis [10]. Other rare causes of SBO like midgut volvulus, intussusception and annular pancreas were adequately depicted and diagnosed on MDCT. One rare cause of SBO seen in our study was endometriosis in which the patient presented with cyclical abdominal pain and obstruction. MDCT showed non-specific enhancing mass in relation of ileal loops which cannot be differentiated on imaging from primary mesenteric masses [11]. Other rare causes of SBO include gall stone ileus, radiation stricture, post-operative strictures [5].
The most common cause of LBO is primary colonic malignancy. In our study, MDCT was accurately depicting the level of obstruction and mass lesion in all cases which is similar to previous studies [12]. One rare cause of LBO was due to gall bladder carcinoma invading hepatic flexure which was well visualized on MDCT, especially with coronal reformats.
Limitation
The present study has few limitations. Being retrospective in nature, the study may have inherent selection bias. Only those subjects with both clinical and MDCT evidence of bowel obstruction were included in study, therefore cases with clinical obstruction but no bowel dilatation at the time of MDCT were excluded from the study. Also cases with mild and intermittent obstruction may have been excluded. Another limitation of this study is that it was limited to only 50 subjects.
Conclusion
MDCT is very useful for depicting the site and cause of both small and large bowel obstruction. With various indirect signs, MDCT can help to confidently diagnose adhesive bands which are most common cause of small bowel obstruction and help to differentiate from other causes. Moreover, MDCT is helpful in diagnosis of closed loop obstruction and bowel ischaemia which are indications for early surgical intervention.
[1]. Suh RS, Maglinte DDT, Lavonas FJ, Emergency abdominal radiography: discrepancies of preliminary and final interpretation and management relevanceEmerg Radiol 1995 2:1-4. [Google Scholar]
[2]. Khurana B, Ledbetter S, McTavish J, Wiesner W, Pablo RR, Bowel obstruction revealed by multidetector CTAm J Roentgenol 2002 178:1139-44. [Google Scholar]
[3]. Nicolaou S, Kai B, Ho S, Su J, Ahamed K, Imaging of acute small-bowel obstructionAm J Roentgenol 2005 185:1036-44. [Google Scholar]
[4]. Desser TS, Megan G, Multidetector row computed tomography of small bowel obstructionSemin Ultrasound CT MR 2008 29(5):308-21. [Google Scholar]
[5]. O’Malley RG, Al-Hawary MM, Kaza RK, Wasnik AP, Platt JF, Francis IR, MDCT findings in small bowel obstruction: implications of the cause and presence of complications on treatment decisionsAbdom Imaging 2015 40(7):2248-62. [Google Scholar]
[6]. Matrawya KA, El-Shazlyb M, Intestinal obstruction: Role of multi-slice CT in emergency departmentAlexandria Journal of Medicine 2014 50:171-78. [Google Scholar]
[7]. Saini DK, Chaudhary P, Durga CK, Saini K, Role of multislice computed tomography in evaluation and management of intestinal obstructionClinics and Practice 2013 3(2):e20 [Google Scholar]
[8]. Delabrousse E, Lubrano J, Jehl J, Morati P, Rouget C, Mantion GA, Small-bowel obstruction from adhesive bands and matted adhesions: CT differentiationAJR Am J Roentgenol 2009 192(3):693-97. [Google Scholar]
[9]. Osada H, Watanabe W, Ohno H, Okada T, Yanagita H, Takahashi Multidetector CT appearance of adhesion-induced small bowel obstructions: matted adhesions versus single adhesive bandsJpn J Radiol 2012 30(9):706-12. [Google Scholar]
[10]. Manchanda SD, Prasad A, Sachdev N, De P, Abbas SZ, Baruah BP, Multi detector computed tomography (MDCT) evaluation of small bowel obstruction: pictorial reviewTrop Gastroenterol 2010 31(4):249-59. [Google Scholar]
[11]. Slesser AA, Sultan S, Kubba F, Sellu DP, Acute small bowel obstruction secondary to intestinal endometriosis, an elusive condition: a case reportWorld J Emerg Surg 2010 5:27 [Google Scholar]
[12]. Angelelli G, Moschetta M, Binetti F, Cosmo T, Stabile Ianora AA, Prognostic value of MDCT in malignant large-bowel obstructionsRadiol Med 2010 115(5):747-57. [Google Scholar]