"Adolescence has been defined by World Health Organization (WHO) as the period of life spanning between the ages 10-19 years" [1]. It forms 20% of the population of the South-East-Asia [2] and 21.4% of India’s population [2]. It is the formative period of life when maximum amount of physical, psychological and behavioural changes take place [3].
Adolescents are the future generation of any country. Adolescence, a second period of rapid growth may serve as an opportunity for compensating faltered early childhood growth, though the potential for significant catch-up is limited [4]. Adolescent girls are a very important section of our society as they are not only valuable citizens of this generation, but will also eventually, mother the next. Several factors such as socio-economic status, environment, attitude towards female children and adolescent girls, ignorance with regard to nutritional requirement, hygiene and illness are responsible for present sub-optimal nutritional status of adolescent girls.
Poor nutrition before birth is carried into adult life and can span into generations. Investing in nutrition throughout the life-cycle will have both short-term as well as long-term benefits of economic and social significance. It is imperative to know the baseline nutritional status of adolescents in a community for planning appropriate interventions. Studying the nutritional status of adolescents will help to plan strategies for combating macro and micro deficiencies of future citizens, including future mothers. There is a difference in the growth patterns and menstrual characteristics between rural and urban adolescent girls and this difference is due to differences in nutrition and life style factors between these two groups.
The current study was therefore, planned to determine anthro-pometric, socio-demographic, menstrual and nutritional status of rural and urban adolescent school going girls of Jodhpur Rajasthan, India and to study the factors affecting them. A review of literature revealed that there is paucity of research from India which specifically focuses on adolescent nutrition and especially adolescent females [5,6].
Materials and Methods
The present study is a cross-sectional, community based, descriptive study conducted in three different (1 urban and 2 rural) schools of Jodhpur under Department of Pediatrics, Dr. S. N. Medical College, Jodhpur (Rajasthan, India) from December 2011 to May 2012 (6 months). Ethics approval was obtained from Medical College ethics committee and permission from school administration was obtained after explaining the objectives and the detailed methodology of this study.
As per census 2011, urban areas of Jodhpur includes Jodhpur city, Kuri Bhagtasani, Mandore Industrial Area, Nandri, Pal Village and Sangariya. Rest all are rural area. We took a urban school from Jodhpur city and two rural schools from Baori, a sparsely populated tehsil, located 49 km away from Jodhpur, where girls from surrounding villages come to study (strength of adolescent girls in government schools was only 10-20).
The study was planned to find out the prevalence of anemia in adolescent school going girls. All adolescent girls between the ages of 11-16 years of age studying in these schools and residing in the study area for more than 6 months willing for sampling were enrolled in study. As per National Family Health Survey-3 (NFHS-3), estimated prevalence of anemia among adolescent girls is 56%. Considering this, a sample size of 327 was obtained with approximately equal inclusion from rural and urban schools by using the formula n= 4pq/d2 and allowable error of 5% (where p = prevalence of study, q = 100-p, d = allowable error). A total of 137 girls from urban area and 190 girls from rural area constituted the final cohort. Adolescent girls of age group 11-16 years studying in school, residing in the study area for a minimum period of 6 months were included in study.
After an introductory lecture on nutrition to all adolescent school going girls in a camp, a pre-determined questionnaire was given to the girls satisfying inclusion criteria. Data of household characteristics, socioeconomic indicators, menstrual history and eating habits were collected by pre-determined questionnaire and an anthropometric examination (including height, weight and body mass index) was done in all these girls. Dietary habits were recorded using a 24 hr dietary recall method. They were also categorized into socioeconomic class using Modified Kuppuswamy scale [7]. Height (in cm) was measured using a simple non-elastic measurement tape to the nearest integer. Weight (in kg) was recorded using a portable personal weighing machine to the nearest integer with ordinary clothing and without shoes. Two readings each were taken for height and weight and the average was used for analysis. BMI was defined as the ratio of weight (in kg) to the square of height (in m). Stunting (height for age) and thinness (BMI for age) were calculated by CDC chart as per the National Centre for Health and Statistics (NCHS) standards [8].
BMI <18.5, 18.5-22.9, 23-24.9, 25-29.9, >30 were classified as Underweight, Ideal BMI, Overweight, Obese Grade I and Obese grade II respectively. Adolescents with BMI values less than 18.5 were considered to be suffering from Chronic Energy Deficiency (CED). CED was further graded into various degrees on the basis of BMI as CED I (17-18.5), CED II (16-17) and CED III (below 16) as per WHO classification [9].
Statistical Analysis
The data was analysed with the help of Microsoft Excel 2010 and Graph pad. Continuous data were calculated and summarized as mean ± SEM and categorical data of the sample were presented as proportion or percentage. The statistical analysis was performed by using graph pad prism employing student t-test, fisher-exact test and Chi-square test to find out the significance of difference in mean between two variables. Fisher-exact test and Chi-square test were used to find out independence/association. The p-value < 0.05 was considered significant.
Results
The mean age of girls was 13.59 ± 1.46 years (13.50 ± 1.34 years in urban areas and 13.65 ± 1.56 years in rural areas). Majority (42.6%) of the adolescent girls included for the study belonged to age group of 13 to 14 years (36.8% in rural area and 50.5% in urban area) followed by 15 to 16 years (35.2% rural area and 24.1% urban area) and 11-12 years (27.8% in rural area and 25.5%).
The anthropometric measurements (weight, height, BMI) of adolescent girls of rural and urban areas are indicated in [Table/Fig-1]. Growth spurt in both the groups was seen between 12-13 years, showing maximum increase in mean height coinciding with menarche.
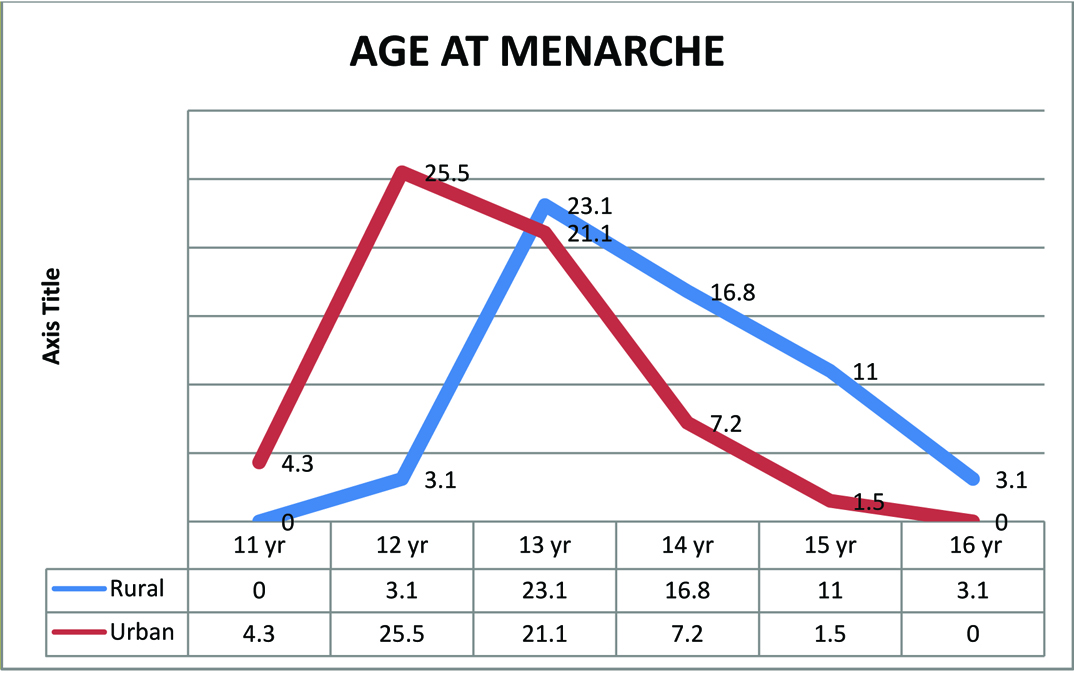
Mean age of menarche was 13.2 year. Most of the girls achieved menarche by 13 years of age (23.3%) followed by 14 years (12.8%) and 12 years (12.5%). Menarche was one year earlier in urban girls as compared to rural girls (p<0.001) [Table/Fig-2]. Only 11.4% girls achieved menarche in 11-12 year age group, 64% girls in 12-14 years age group and 95.9% in 14-16 years age group.
Mean weight, height and BMI of adolescent females in different age groups in urban and rural areas (n=327).
| Age group(in years) | Area(n) | Mean weight(in kg) ± S.E.M. | Mean height(in m) ± S.E.M. | Mean BMI ±S.E.M. |
|---|
| 11-12 Year | Urban(n=34) | 34.38 ± 1.196 | 145.6 ± 1.508 | 16.06 ± 0.4532, |
| Rural (n=54) | 32.76 ± 0.9816 | 142.1 ± 1.119 | 16.45 ± 0.3175 |
| p-value | 0.30 | 0.057 | 0.47 |
| 12-14 Year | Urban(n=69) | 40.86 ± 0.7138 | 155 ± 0.9105 | 17.01 ± 0.2048 |
| Rural (n=70) | 41.09 ± 0.6337, | 153.2 ± 0.657 | 17.62 ± 0.2369 |
| p-value | 0.80 | 0.10 | 0.054 |
| 14-16 Year | Urban(n=34) | 44.24 ± 1.38, | 157.5 ± 1.146 | 17.76 ± 0.4448 |
| Rural (n=66) | 44.59 ± 0.698, | 156.1 ± 0.7013 | 18.33 ± 0.2768 |
| p-value | 0.79 | 0.29 | 0.26 |
| TOTAL | Urban(n=137) | 39.96 ± 0.5581 | 153.3 ± 0.7585 | 16.96 ± 0.1937 |
| Rural (n=190) | 40.09 ± 0.6497 | 151.1 ± 0.6316 | 17.53 ± 0.1664 |
| p-value | 0.88 | 0.02 | 0.02 |
Student’s t-test.
Thinness in urban areas ranged from 26.5% to 35.3% and in rural areas from 12.9% to 22.7%. The prevalence of stunting in the rural areas ranged from 22.7% to 31.5% among rural as compared to 17.6% to 29.4% among urban females. Thinness was more prevalent among females in urban areas and stunting was more in rural areas. However, difference in thinness and stunting among rural and urban population was not significant [Table/Fig-3].
Age-wise prevalence of stunting and thinness in adolescent females in urban and rural population (n=327).
| Age group (in years) | Area (n) | Stunting (%) | Thinness (%) |
|---|
| 11-12 Year | Urban(n=34) | 6 (17.6) | 9 (26.5) |
| Rural (n=54) | 17 (31.5) | 12 (22.2) |
| p-value | 0.21 | 0.79 |
| 12-14 Year | Urban(n=69) | 13 (18.8) | 16 (23.2) |
| Rural (n=70) | 18 (25.7) | 9 (12.9) |
| p-value | 0.41 | 0.13 |
| 14-16 Year | Urban(n=34) | 10 (29.4) | 12 (35.3) |
| Rural (n=66) | 15 (22.7) | 15 (22.7) |
| p-value | 0.47 | 0.23 |
| Overall | Urban (137) | 29(21.2) | 37 (27.0) |
| Rural (190) | 50 (26.3) | 36 (18.9) |
| p-value | 0.29 | 0.10 |
Fisher-exact test
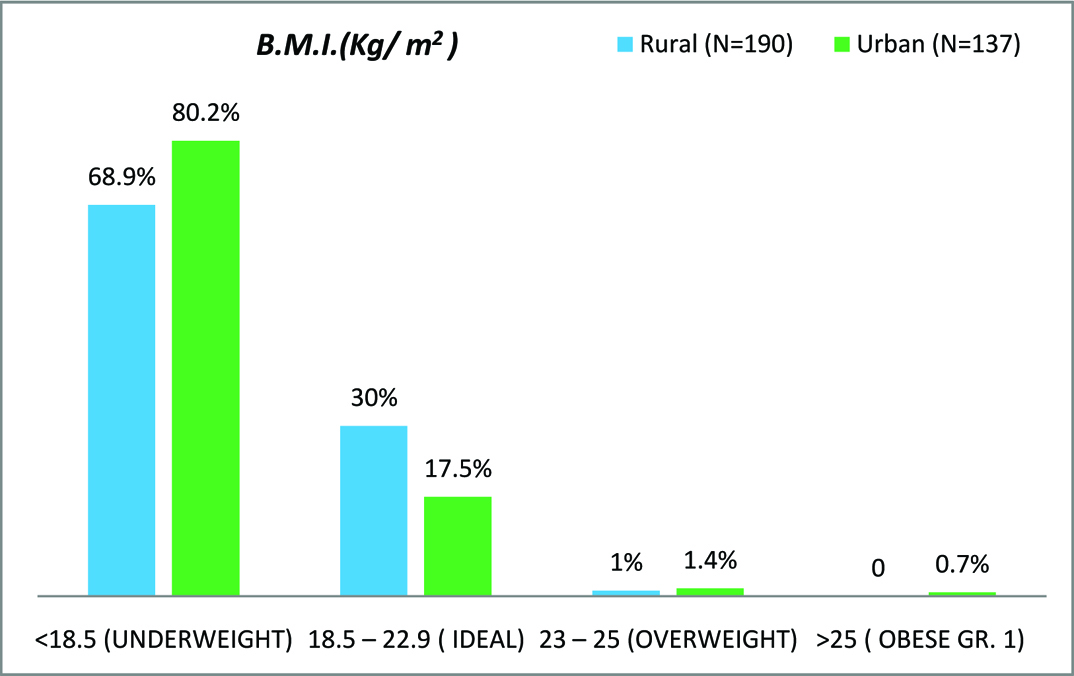
It was disappointing to note that only 24.7% girls were found to have a normal BMI. Majority of the adolescent girls (73.7%) in both the groups combined were underweight. The number of underweight rural girls was statistically significantly lower (p <0.05) as compared to urban underweight girls [Table/Fig-4]. In the present study, 24.7%, 25.6%, 19.9%, and 28.1% of population had normal BMI, CED I, II and III respectively.
Distribution of adolescent girls based on BMI classification.
In the current study; however, all the anthropometric measurements of 25-35% adolescents in both the groups were lower than National Center for Health and Statistics (NCHS) standards. Interestingly, rural girls had a better status in terms of weight and BMI for age as compared to urban girls, except for height which was significantly lower in rural girls.
Majority of the girls (76.3% and 70.0% in urban and rural area respectively) in the current study belonged to a nuclear family and 23.7% urban girls as compared to 30% rural girls were from a joint family. Most of the girls in both the groups were in a family with size of 5 to 10 members (85.8% and 67.2% in rural and urban area, respectively) followed by 2 to 4 members (9.5% and 14.5% in rural and urban area, respectively) and above 10 members (4.7% in rural area and 18.3% in urban area). A 51.1% of the mothers were literate in the current study and rural mothers had significantly lower literacy as compared to urban mothers [Table/Fig-5].
| Maternal education | Urban (%) | Rural (%) | Total (%) |
|---|
| Illiterate | 49 (35.7) | 118 (62.1) | 167 (51.1) |
| Primary School Certificate | 21(15.3) | 26 (13.7) | 47 (14.4) |
| Middle School Certificate | 35 (25.5) | 22 (11.6) | 57 (17.4) |
| High School Certificate | 24 (17.5) | 16 (8.4) | 40 (12.2) |
| Intermediate / Post high school diploma | 0 (0) | 5 (2.6) | 5 (1.5) |
| Graduate/ Post graduate | 6 (4.4) | 0 (0) | 6 (1.8) |
| Profession / Honours | 2 (1.4) | 3 (1.6) | 5 (1.5) |
| Overall | 137 (100) | 190 (100) | 327 (100) |
Chi-square- 37.19, p-value <0.0001
Out of 327 subjects, negligible (1.2%) girls were consuming eggs apart from their vegetarian diet. However, more than three-fourth of the girls (89.6%) were pure vegetarians, while the rest (9.2%) were also consuming non-vegetarian food stuff in their diet. There was significant difference in intake of green leafy vegetables which was more frequent in rural population and intake of pulses was significantly higher in urban population [Table/Fig-6]. In the present study only 20% girls consumed jaggery which is an excellent source of iron for population of western Rajasthan. Most of the population in this region does not consume enough green leafy vegetables, non –vegetarian food and other significant sources of iron in their diet.
Frequency of consumption of pulses and green leafy vegetables.
| Frequency of consumption | Pulses | Green leafy vegetables |
|---|
| Urban (%) | Rural (%) | Total (%) | Urban (%) | Rural (%) | Total (%) |
|---|
| Daily | 7 (5.1) | 18 (9.5) | 25 (7.6) | 28 (20.4) | 64 (33.7) | 92 (28.1) |
| Twice a week | 52 (38.0) | 45 (26.7) | 97 (29.7) | 56 (40.9) | 38 (20) | 94 (28.7) |
| Weekly once | 26 (19.0) | 40 (21.1) | 66 (20.2) | 19(13.9) | 24 (12.6) | 43 (13.1) |
| Once in fortnight | 4 (2.9) | 1 (0.5) | 5 (1.5) | 2 (1.5) | 5 (2.6) | 7 (2.1) |
| Monthly | 7 (5.1) | 8 (4.2) | 15 (4.6) | 6 (4.4) | 4 (2.1) | 10 (3.1) |
| Occasionally | 38 (27.7) | 77 (40.5) | 115 (35.2 | 17 (12.4) | 54 (28.4) | 71 (21.7) |
| Not at all | 3 (2.2) | 1 (0.5) | 4 (1.2) | 9 (6.6) | 1 (0.5) | 10 (3.1) |
| Total | 137 (100) | 190 (100) | 327 (100) | 137 (100) | 190 (100) | 327 (100) |
| Chi-square | 12.21 | 37.89 |
| p value | 0.057 | <0.0001 |
Chi-square test with yate’s correction
Discussion
Nearly one fourth of India’s population comprises of adolescents [2] and nutritional status of this group is an important determinant of health outcomes. Hence, it is of utmost importance to improve nutritional status during adolescence. Moreover rural adolescent girls are considered a deprived segment and urban girls have lifestyle problems related to human health. The current study noted many interesting observations related to the aforementioned issues and tried to tease apart the impact of deprivation and life style issues on the health of adolescent girls.
The anthropometric measurements/parameters of adolescent school going girls in the present study were comparable to the observations made by Prabhakaran et al., NCHS reference standard and Zanvar et al., and for that age [2,6,10] and higher in our study at all ages when compared to another study James et al., and Thakor et al., [9,11]. This may be explained by the fact that in the current study most of the girls were from a private school where parents may have access to better nutrition. Although the weight gain was more in rural girls as compared to urban girls but the difference was not significant. This can be attributed to the fact that these girls had not yet achieved pubertal spurt as compared to their urban counterpart who started to have a pubertal spurt related to onset of menarche. Rah et al., observed that the rural menstruating girls are given more nutritious food due to cultural reasons, while no special focus is made on diet and nutrition of girls between 11-12 years who have yet not started to menstruate [12].
Increase in height in present study (from 140 cm to 157 cm) was comparable to a study carried out by Thakor et al., (132.8 to 150 cm in age group 10-15 years), Venkaiah et al., (144.1 to 149.8 cm in age group 13-16 years) [11,13]. A little slowing down of growth was observed in the present study (in terms of weight and height) in 15-16 years age group. Pubertal spurt has been seen between 12-13 years [14]. Other studies have also reported the occurrence of growth spurt between 12 and 15 years of age [14,15]. Urban girls were significantly taller than rural girls. Similar results were observed by Prabhakaran [2] and Zanvar et al., [10]. No clear cut reason was found for this observation but it may be possible that the urban girls gave more emphasis to pulses and protein rich diet. However, girls in both urban and rural areas showed a similar increment in mean height at all ages. This might be due to delayed growth spurt in rural females.
It was dismal to observe that in the current study majority of adolescent girls (73.7%) were underweight (BMI<18.5) which again raises the issues related to poor parental and community attitudes regarding nutrition of girl child right from her birth. This was also proved in the current study by the fact that maternal education was lower in rural area. Similar results (prevalence of underweight ranging from 53.8% to 68.52%) have been reported by Shahabuddin et al., Choudhary et al., and Deshmukh et al., [16–18]. The status of chronic energy deficiency seen in the present study was comparable with the observations made by Choudhary S et al., and Kumari and Singh [17,19]. There was consistently increasing trend of mean BMI from the age of 11 years onwards as reported by Das et al., [20]. The mean BMI in the current study subjects was more as compared to the studies conducted by Thakor et al., [11]. It was found that the mean BMI was significantly higher in rural subjects as compared to the urban subjects except 11-12 years age group.
However, the applicability of BMI and its categorization for labeling underweight in pediatric population using the current criteria is questionable and the authors propose that instead of using BMI <18.5 to label underweight, age specific criteria for BMI should be used to categorize underweight or more specifically thinness in pediatric population. In the present study, the nutritional status of adolescents was also assessed using NCHS standards. Stunting, which is considered as an index for chronic under nutrition and thinness which indicates acute under nutrition, were observed among the subjects in all the age groups in both the areas. Prevalence of both stunting and thinness increased with age except stunting in rural girls where a decrease in prevalence was noted. Venkaiah et al., showed 39% of the adolescents were stunted [13]. The prevalence of thinness varied between 12% to 35% among females. Mulugeta et al., in their study among Ethiopian adolescent females, recorded the prevalence of stunting and thinness as 26.5% and 58.3 % respectively using the WHO 2007 growth reference [21]. Bose & Bisai observed a decreasing trend of under nutrition from from 45.76% to 20.17% among girls from 10 years to 15 years of age [22]. Medhi et al., in their study found that the prevalence of stunting was 51.9% among females and thinness among females was (41.3%) [23].
In the current study, thinness was more prevalent among females in urban areas and stunting was more common amongst girls residing in rural areas. Height being denominator in BMI may be the reason for more thinness despite less stunting in urban girls. The prevalence of stunting was higher than the prevalence of thinness among girls. The phenomenon of the higher proportion of stunting may indicate that consumption of foods rich in protein is responsible for height was far below the required level. This could be attributed to the increased intake of milk and milk products, fats and oils, sugar and jaggery by rural children and unhealthy nutrition and life-style of urban children [3]. Intake of fat rich diet (milk and milk products) in rural girls contributed to less thinness in them and protein rich diet (pulses) in urban girls contributed to less stunting in them. The current study sampled private schools in both rural and urban areas and therefore, it is presumed that the economic status of the parents of children in these schools was very similar in rural and urban areas. Therefore, the access to good diet from economic perspective was presumed, not be an issue in both the groups. However, in the urban areas there is easy access to junk food/ fast food the frequency of eating at home is much lesser and moreover the intake of fruits and vegetables is also much less. BMI is a good index to assess the current form of malnutrition and general obesity and is due to net effect of influences like childhood malnutrition, worm infestations, body consciousness, dieting, missing meals and fast-food intake [2].
In the current study, mean age of menarche was (13.2 years) almost similar to the age of menarche reported by Shekhar et al., (13 years). It was also observed that urban girls achieved menarche 1 year earlier as compared to rural girls [24]. Bhanushali et al., Hesketh et al., found that girls who reach menarche are significantly heavier and taller with higher BMIs than those of the same age who are pre-menarche [25,26]. Similar findings were observed by Hesketh et al., and Kaur et al., [26,27]. As explained above the causes for this earlier age of menarche could be due to life style issues typical of urban living and mostly attributed to dieting, missing meals, fast-food intake and unhealthy lifestyle in urban girls as has also been reported by Prabhakaran [2]. Toress et al., found that BMI and improving socioeconomic status and urban residence is said to effect the age at menarche [28]. In the present study, 89.6% girls were vegetarian and had a cereal based (wheat and bajra) staple diet. Das et al., also observed that the diet of adolescent girls in India is basically cereal based with wheat and rice as a staple food [29]. Tatia and Taneja also reported low intake of green leafy vegetables in adolescent girls [30]. In the present study as indicated above, the intake of milk products, fresh vegetables and fruits of the rural girls was much better as compared to urban girls.
Limitation
Despite the fact that an appropriate sample was used in the study, sample was still not representative of the whole population. This is because of the fact that children studying in private schools may not be truly representative of the adolescent health status of the country as most of these children are from and affluent family. More studies with a larger sample size involving general population of girls in the age group from 10 years to 19 years drawn from the community will therefore provide more accurate information in this regard.
Conclusion
The results of the current study therefore, clearly conclude that in general there is a huge gap between optimal/ recommended and observed physical growth, dietary and lifestyle habits and nutritional status of adolescent girls in India, specifically in difficult terrains of Western Rajasthan and majority of rural India. It is unfortunate to note that despite good availability of dairy products, vegetables and fruits in rural area, the rural girls have a lower final height. More studies will be required to find out the reasons for this observation and specific targeted strategies need to be in place to improve this situation. It can also be concluded that the age of menarche is very much related to urbanization, diet and lifestyle. More urbanization therefore may translate into physiologic processes that will start showing a negative or pathologic trend. The current study therefore adds to the understanding of the nutritional and lifestyle factors causing alterations in the anthropometric and pubertal growth of Indian children which represent a mix of developed and underdeveloped population strata.
Student’s t-test.
Fisher-exact test
Chi-square- 37.19, p-value <0.0001
Chi-square test with yate’s correction