Successful Obstetric Outcome in Dextrocardia with Situs Inversus and Moderate Pulmonary Hypertension- Rare Case
Deepika1, Leena Wadhwa2, Chandna Shekhar3, Jyoti Saini4, Monica Chetani5
1 Senior Resident, Department of Obstetrics and Gynaecology, ESI, Basaidarapur, New Delhi, India.
2 Associate Professor, Department of Obstetrics and Gynaecology, ESI, Basaidarapur, New Delhi, India.
3 Senior Resident, Department of Obstetrics and Gynaecology, ESI, Basaidarapur, New Delhi, India.
4 Senior Resident, Department of Obstetrics and Gynaecology, Babu Jag Jivan Ram Memorial, Hospital, New Delhi, India.
5 FNB Trainee, Institute of Reproductive Medicine, Kolkata, West Bengal, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Deepika, Hno.132/First Floor, Defence Enlave, Near Preet Vihar Metro Station, New Delhi-110092, India.
E-mail: lhmcdeepika@gmail.com
Situs inversus is a rare congenital anomaly, which is characterized by right sided heart (Dextrocardia) and inversely rotated visceral organs of abdomen. In present case, the patient reported with G3p2l2, 34 weeks of gestational period along with breathlessness accompanied and labour pains. On further investigation, she was diagnosed as dextrocardia with situs inversus and moderate pulmonary artery hypertension along with severe iron deficiency anaemia. Patient had normal vaginal delivery with intra-partum and post-partum period. Normally, any patient having situs inversus has a normal life expectancy and is not associated with any significant morbidity or mortality.
Congenital anamoly, Iron deficiency anaemia, Right sided heart
Case Report
A 31-year-old female, G3p2l2 was presented with history of 8 and half month amenorrhea with backache and breathlessness since 2 days. Breathlessness was insidious in onset and progressive, even on walking some distance. There was no history of orthopnea or paroxysmal nocturnal dyspnea. In past, prior to her previous pregnancy she was diagnosed with dextrocardia. She had two normal vaginal deliveries, both were alive and healthy. Both intra-partum and post-partum period were uneventful. Her first girl baby was four-year-old and inter-pregnancy period between 2nd and 3rd one was one and half year. In her family, her grandmother had dextrocardia and her father also died due to some cardiac disease.
On examination, patient was found conscious and well oriented to time, place and person. On general physical examination, she was very pale, had a pulse of 60/min, which was regular, with average volume, Blood Pressure (BP) of 100/60mmHg. Her Jugular Venous Pulse (JVP) was normal; RR-24/min, pedaloedema 1+, no cyanosis and clubbing. There were no signs of Congestive Cardiac Failure (CCF) and Chest examination was normal. On cardiovascular examination, the apex was present in the 6th Intercostal Space (ICS) on the right side and a systolic murmur (2/6 grade) heard over right parasternal border.
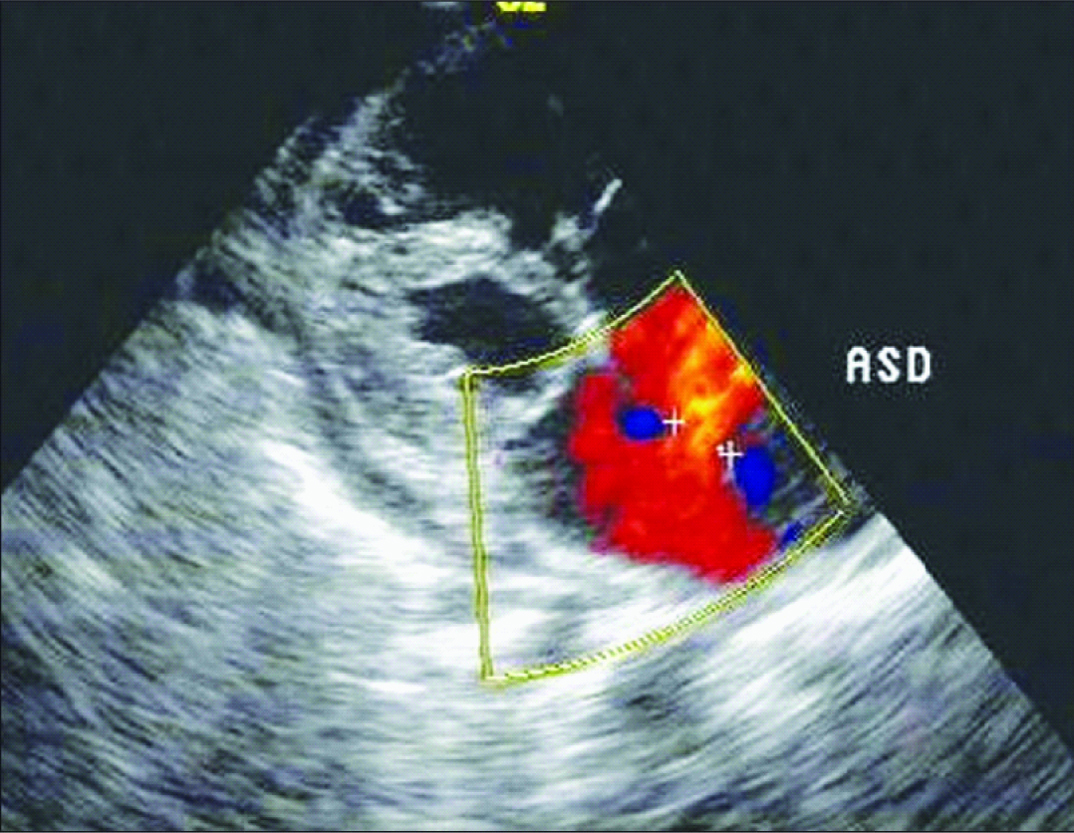
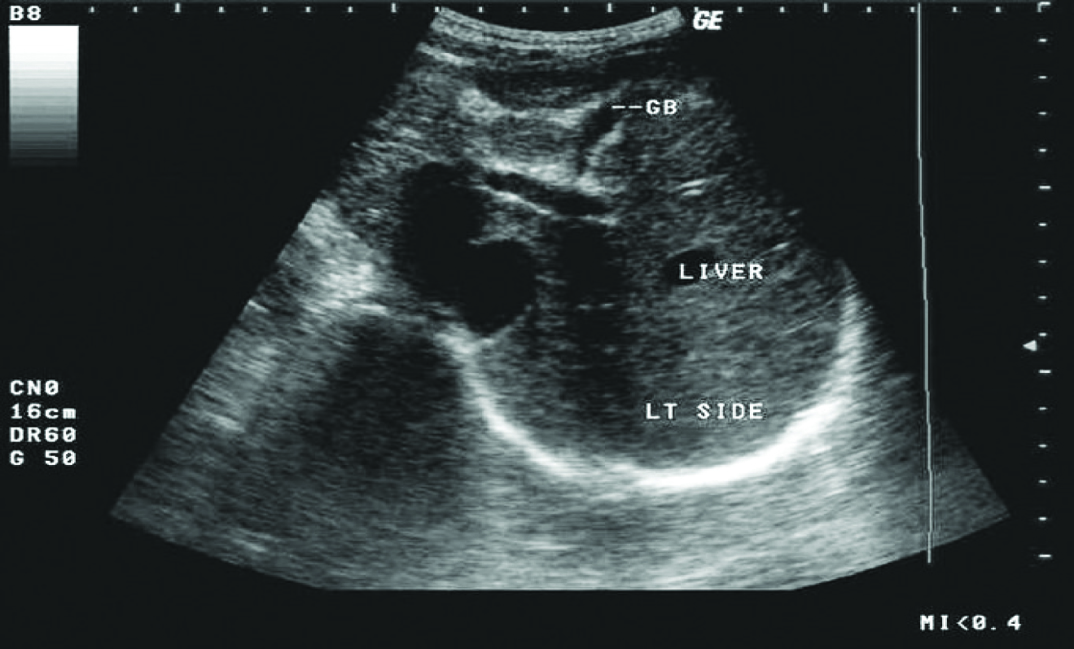
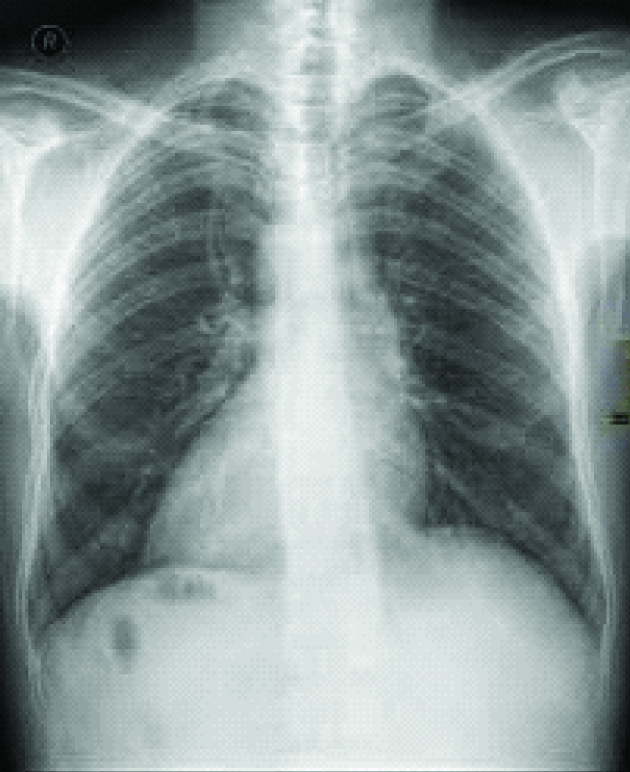
On investigation, her haemogram was normal except Hb-6.5 gm/dl with reduced MCV/MCH/MCHC. The peripheral smear showed microcytic hypochromic picture making diagnosis of iron deficiency anaemia. Other blood and urine investigations were normal. ECG showed right axis deviation. A 2D Echo Doppler [Table/Fig-1] showed dextrocardia /acyanotic heart disease along with large ostium secundum ASD 42mm, moderate pulmonary artery hypertension, normal biventricular function associated with moderate tricuspid regurgitation. Diagnosis of situs inversus was confirmed by ultrasound abdomen in which all visceral organs were inversely rotated [Table/Fig-2]. Obstetric sonography made diagnosis of severe oligohydramnios. Chest x-ray and CT which were done pre-pregnancy but after her first delivery confirming dextrocardia and situs inversus in 2012 [Table/Fig-3,4 and 5].
2D echocardiography showing atrial septal defect.
Ultrasound of abdomen showing liver on the left side.
Chest X-ray showing dextrocardia.
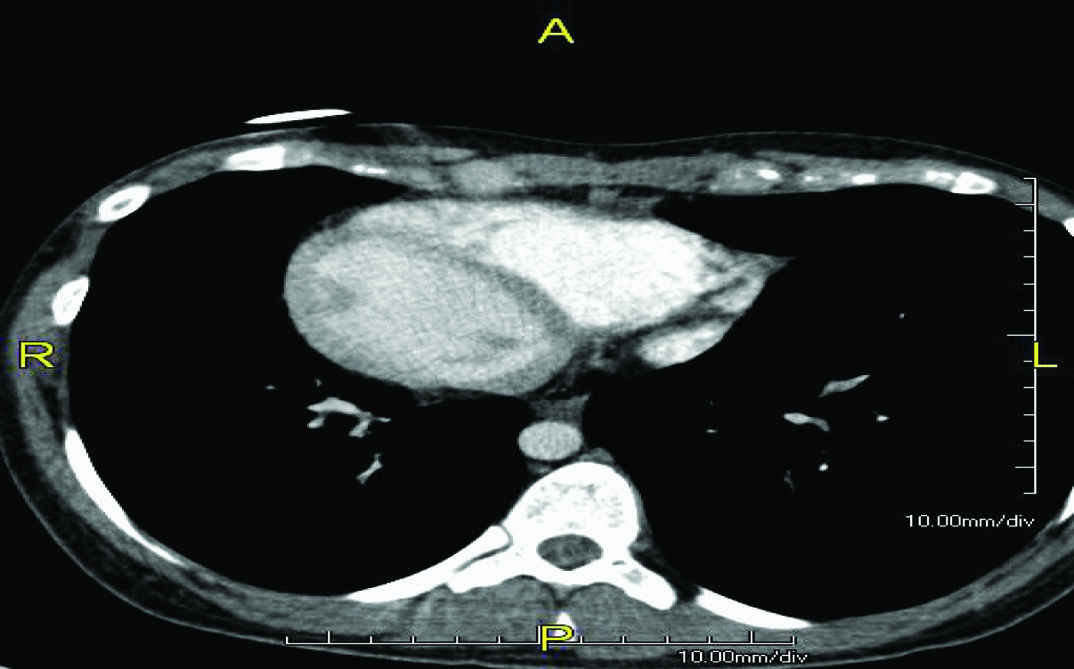
Axial CT image showing situs inversus (liver and IVC on the left, spleen and aorta on the right).
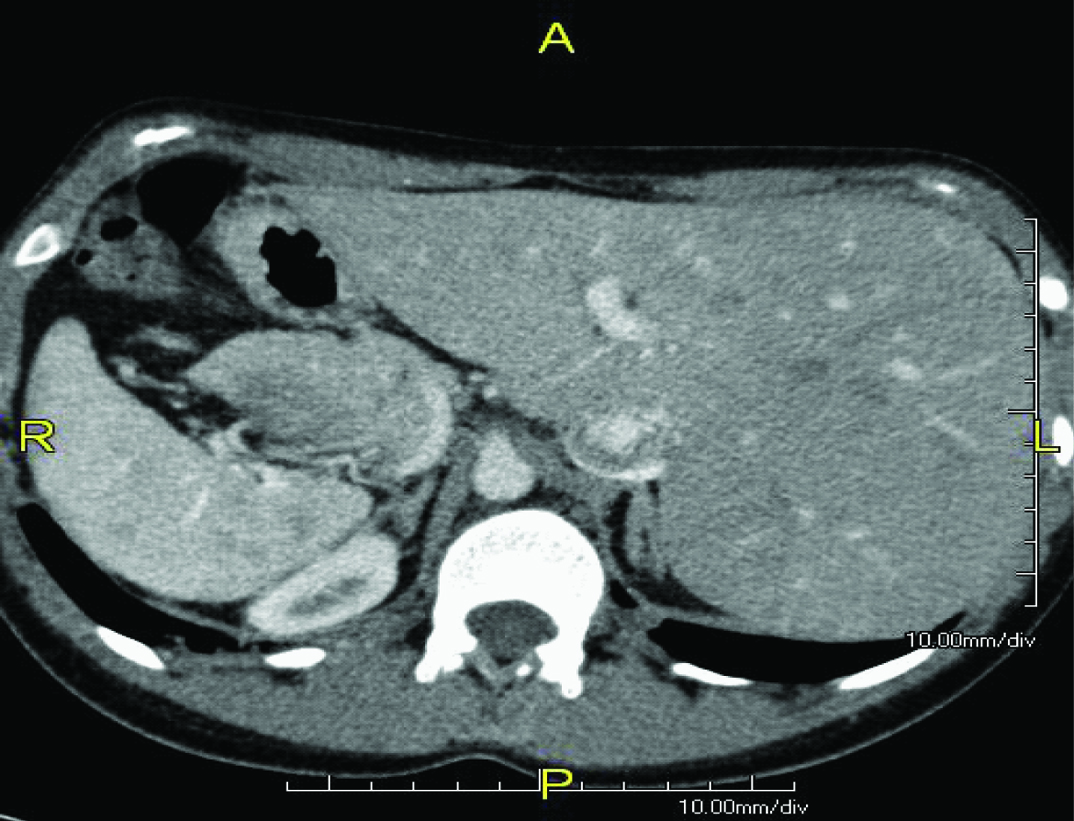
Axial CT image showing dextrocardia and situs inversus.
Patient was transfused 2 unit of packed cell volume under lasix coverage. She was kept in ICU care. She maintained her saturation on oxygen and Betamethasone coverage was done. CVP, Pulse, BP, RR, Spo2, ECG, input/output were monitored. Patient kept propped up and spontaneously went into labor. Concentrated syntocinon was given to augment labor in view of delayed progress and oligohydramnios. Patient had pre-term normal vaginal delivery of female baby of average weight 2.5 kg. Her intra-partum and post-partum period was normal.
Discussion
Dextrocardia with situs inversus is defined as right sided heart along with all inversely rotated visceral organs (mirror image) [1]. It is a rare disease with incidence rate of 1/10,000 live births [2,3]. Autosomal mode of inheritance is seen with dextrocardia, along with equal ratio seen in both gender [4].
Dextrocardia with situs inversus remains asymptomatic and normally remains undiagnosed unless diagnosed incidentally while investigating for another ailment. In our case, the diagnosis was made during investigation of cause of severe iron deficiency anaemia and associated respiratory problem. The common congenital cardiac anomalies associated by dextrocardia with situs inversus are atrial situs solitus (93%), discordant AV connection (44%), and discordant Ventriculo-Atrial (VA) connection (30%). Congenitally corrected Transposition of Great Arteries (TGA) occurs in less than 1% of all forms of congenital heart disease [5]. Certain congenital anomalies such as polysplenia (left isomerism)/asplenia (right isomerism) or Kartagener’s syndrome (primary ciliary dyskinesia often leading to infection of the paranasal sinuses and lungs) are known to occur [6]. About 25% of individuals with situs inversus have an association with Primary Ciliary Dyskinesia (PCD). Situs inversus with PCD together known as Kartagener syndrome characterized by the triad of situs inversus, chronic sinusitis and bronchiectasis [7]. More complex cardiac malformations can also be associated with dextrocardia, such as tricuspid atresia single ventricle and double-outlet or double-inlet ventricles [8]. However, our patient did not have any of these abnormalities.
Jain et al., reported a case of situs inversus with dextrocardia, Lutembacher’s syndrome and pericardial effusion. The pericardial effusion was acquired and was tubercular in aetiology [9]. There have been numerous reports [10–12] till date describing the presence of rheumatic MS with dextrocardia and/or situs inversus. Ultrasongraphy or radiography can be used for confirmation of associated complications with situs inversus [13]. A case report reported in year 2013[14] that child having dextrocardia and situs inversus with multiple congenital heart anomalies, born from a diabetic mother have been rarely described in literature. For definitive diagnosis of situs inversus with dextrocardia is Computed Tomography (CT) as this provides an excellent anatomic detail and magnetic resonance imaging is reserved for patients with associated cardiac abnormalities [15,16]. ECG can confirm the medical diagnosis of the two forms of dextrocardia. ECG can show inversion of the electrical waves and is considered one of the best diagnostic test option. Pregnancy which are complicated by isolated dextrocardia do not have significant effect on the disease or vice-versa unless complicated by other complications, however small for gestational babies should be watched [17].
The treatment for dextrocardia with situs inversus is usually supportive. Generally, patients may live a normal life without any complaints. The prognosis and treatment varies and usually depends on the condition and its associated cardiac abnormalities and complications. Affected families may benefit from genetic counseling.
Conclusion
Situs inversus with dextrocardia patients have normal life span and uncomplicated life, unless it is complicated with structural and functional defects.
[1]. Radhika BH, Harshini V, Ramaiah R, Successful pregnancy outcome in a rarecase of complete situs Inversus in a primigravidaInt J Reprod Contracept Obstet Gynecol 2015 4(4):1203-05. [Google Scholar]
[2]. Supriya G, Saritha S, Madan S, Situs inversus totalis - a case reportIOSR Journal of Applied Physics (IOSR-JAP) 2013 3(6):12-16. [Google Scholar]
[3]. Bohun CM, Potts JE, Casey BM, Sandor GG, A population-based study of cardiac malformations and outcomes associated with dextrocardiaAm J Cardiol 2007 100(2):305-09. [Google Scholar]
[4]. Tayeb M, Khan FM, Rauf F, Situs inversus totalis with perforated duodenal ulcer: a case reportJournal of Medical Case Reports 2011 5;279(10):1186/1752-1947 [Google Scholar]
[5]. Ma N, Jiang SL, Huang LJ, Zhao SH, Xu ZY, Ling J, Diagnosis of isolated dextrocardia using angiocardiography or surgeryChin Med J (Engl) 2004 117:1655-58. [Google Scholar]
[6]. Shapiro AJ, Davis SD, Ferkol TF, Dell SD, Rosenfeld M, Olivier KN, Laterality defects other than situs inversus totalis in primary ciliary dyskinesia: Insights into situs ambiguus and heterotaxyChest 2014a 146:1176-86. [Google Scholar]
[7]. Dabhi AS, Chaudhari SR, Throat PB, Pandya HB, Shah MC, Meswani UN, Kartagner syndrome: A triad of bronchieatasis, situsinversus and chronic sinusitisJIACM 2005 6(3):241-43. [Google Scholar]
[8]. Huhta JC, Hagler DJ, Seward JB, Tajik AJ, Julsrud PR, Ritter DG, Two-dimensional echocardiographic assessment of dextrocardia: a segmental approachAm J Cardiol 1982 50:1351-60. [Google Scholar]
[9]. Jain VV, Gupta OP, Jain J, A rare case of situs inversus with dextrocardia, lutembacher syndrome, and pericardial effusionHeart Views 2011 12(3):107-11. [Google Scholar]
[10]. Hussain S, Ahmed W, Percutaneous transvenous mitral commissurotomy in mitral restenosis with situs inversusJ Coll Physicians Surg Pak 2009 19:117-19. [Google Scholar]
[11]. Namboodiri N, Harikrishnan SP, Ajitkumar V, Tharakan JA, Percutaneous mitral commissurotomy in a case of mirror-image dextrocardia and rheumatic mitralstenosisJ Invasive Cardiol 2008 20:E33-35. [Google Scholar]
[12]. Verma PK, Bali HK, Suresh PV, Varma JS, Balloon mitral valvotomy using Inoue technique in a patient of isolated dextrocardia with rheumatic mitral stenosisIndian Heart J 1999 51:315-17. [Google Scholar]
[13]. Silverman NH, An ultrasonic approach to the diagnosis of cardiac situs, connections, and malpositionsCardiol Clin 1983 1(3):473-86. [Google Scholar]
[14]. Voshtani SH, Saadat SNS, Saadat SMS, Mehrdad M, Moladoust H, Nasiri E, A rare case of dextrocardia with situs inversus totalis in a patient of diabetic motherAnatomical Science 2013 10(4):41-44. [Google Scholar]
[15]. Tonkin IL, Tonkin AK, Visceroatrial situs abnormalities: sonographic and computed tomographic appearanceAJR Am J Roentgenol 1982 138(3):509 [Google Scholar]
[16]. Yoo SJ, Kim YM, Choe YH, Magnetic resonance imaging of complex congenital heart diseaseInt J Card Imaging 1999 15(2):151-60. [Google Scholar]
[17]. Fung TY, Chan DL, Leung TN, Leung TY, Lau TK, Dextrocardia in pregnancy: 20 years’ experienceJ Reprod Med 2006 51(7):573-77. [Google Scholar]