India has nearly 26.8million people suffering from one or the other type of disability according to the census conducted in 2011 [1]. This is equivalent to 2.21% of the total population. Out of these, 7.8million are children aged 0-19 years accounting for 29% of the total disabled population [1]. The five common types of disabilities in children are visual impairment, hearing impairment, physical disability, mental disability and learning disability. Each disability affects the overall development of a child but if he/she has multiple disabilities, the negative impact on quality of life increases manifolds. When one of the senses is lost, the child uses the other sense to compensate for the disability. In children with disabilities other than visual disabilities, vision is one of the important senses which has more value for these children as they heavily depend on visual inputs for their understanding and communication with the outer world [2,3]. Thus, even a minor visual problem, reducing their visual clues, needs to be identified and addressed at the earliest in order to optimize their social and academic performance.
The ocular problems in children with disabilities other than visual disabilities are often overlooked, as the main focus always remains on the primary disability [4]. Additionally, the ocular examination in these children is a challenge and needs patience, skills and a broader range of assessment instruments [3].
Studies have reported higher incidence of ophthalmologic abnormalities among children with other disabilities [2–6]. Thus, the aim of the present study was to assess the visual function and ocular status of children with other disabilities and to identify the preventable and treatable causes of visual impairment.
Materials and Methods
This study was conducted on children with disabilities (other than visual disabilities), aged 3-16 years, who were studying in rehabilitation centers and special schools (excluding schools for blind children) in Ludhiana district, between 1st June 2014 and 31st December 2014. Prior permission was sought from the principals of the special schools. Parents were informed and their presence was requested during the examination of the children. A team from the Department of Ophthalmology of Christian Medical College, Ludhiana comprising of an ophthalmologist, refractionist and ophthalmic technician visited these institutes.
The examination process was explained to the parents and the teachers. Written informed consent was taken. Relevant history regarding the type of disability, birth history, family history and history of consanguinity was recorded.
Ocular examination was carried out in diffuse illumination with a flash light to observe head posture and facial anomalies. Snellen’s E-chart was used for assessing visual acuity in children who could read and co-operate. For other children, visual acuity was tested using Cardiff’s preferential looking tests or Cambridge cards or both. Near vision testing was done at 33cm followed by distant vision testing at 6 metres. Hirshberg light reflex test and cover uncover test was used to evaluate visual axis and strabismus. Ocular movements were tested and presence of nystagmus was checked. Anterior segment was examined using torch light and magnifying loupe of 6X to rule out any abnormalities of eyelids, conjunctiva, cornea, anterior chamber, iris and lens. Direct and consensual papillary light reflexes were also checked.
Subjective correction of refractive errors was attempted in children aged 12 years and above. Cycloplegic retinoscopy was done in all children aged 3-12 years and in those who were unco-operative for subjective refraction. Cycloplegic retinoscopy was done using 0.3% cyclopentolate eye drops after ascertaining that the child didn’t have seizures. In case of history of seizures, 0.5% homide eye drops were used. Spectacle prescription was given to all children with refractive errors. The type of refractive error was recorded. Myopia was defined as spherical equivalent of less than or equal to -0.5 diopter, Hypermetropia as more than or equal to +1.0 diopter and Astigmatism as more than or equal to ±0.5 diopter. Amblyopia was defined as best corrected visual acuity of 6/12 or less or difference of 2 lines in the best corrected visual acuity between the two eyes with no intra-ocular anatomical pathology.
A detailed fundus examination after dilatation was done by direct ophthalmoscope either after cycloplegic retinoscopy or after dilating the pupils with 1% tropicamide eye drops. Children requiring further evaluation were referred to the base hospital.
The data was entered using an excel sheet and analysed using SPSS software version 22. The data was expressed using descriptive statistics.
Results
The study was conducted in seven rehabilitation centers/special schools in Ludhiana district. A total of 404 children with disabilities (other than visual disabilities) aged 3-16 years, who were studying in these schools, were enrolled in the study. Out of these, 141 (34.9%) were in the age group of 3-9 years and 263 (65.1%) were in the age group of 10-16 years. There were 280 males (69.3%) as compared to 124 females (30.7%) in the study. Out of these, 96 (23.8%) had positive birth history of adverse antenatal, natal or post-natal events, 73 (18.1%) had positive family history, 3 (0.7%) had positive history of consanguinity and 56 (13.9%) had positive history of ocular morbidity like history of use of spectacles, ocular medication or ocular surgery.
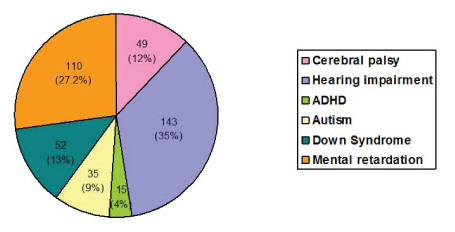
The study covered children with six different types of disabilities – Cerebral palsy, Hearing impairment, Attention Deficit Hyperactive Disorder (ADHD), Autism, Down syndrome and Mental retardation. Majority of the children were hearing impaired and with Mental retardation. [Table/Fig-1] shows the distribution of children according to the disabilities.
Distribution of children according to disabilities.
Out of 404 children, ocular disorders were present in 174 (43%) of children. These included 69.3% children with Cerebral palsy, 25.1% with Hearing impairment, 53.3% with ADHD, 25.7% with Autism, 69.2% with Down syndrome and 46.3% with Mental retardation [Table/Fig-2].
Frequency of ocular findings in children with disabilities.
| Disability | No of children with ocular findings (Total number) | % |
|---|
| Cerebral palsy | 34 (49) | 69.3 |
| Hearing impairment | 36 (143) | 25.1 |
| ADHD | 8 (15) | 53.3 |
| Autism | 9 (35) | 25.7 |
| Down Syndrome | 36 (52) | 69.2 |
| Mental retardation | 51 (110) | 46.3 |
| Total | 174 (404) | 43.0 |
The most common ocular manifestation observed in the study was refractive errors, present in 23.0% children. Strabismus was the second most common finding, seen in 18.1% children. [Table/Fig-3] shows the distribution of ocular disorders in details.
Distribution of ocular disorders.
| Ocular disorders | Frequency | Percent |
|---|
| Defective distant vision | 115 | 28.4 |
| Refractive errorsHypermetropiaMyopiaAstigmatism | 93275313 | 23.06.713.13.2 |
| Strabismus | 73 | 18.1 |
| Nystagmus | 67 | 16.6 |
| Squamous blephritis | 9 | 2.2 |
| Megalocornea | 2 | 0.5 |
| Microcornea | 4 | 1 |
| Ptosis | 4 | 1 |
| Discharge | 3 | 0.7 |
| Nodular episcleritis | 1 | 0.2 |
| Corneal opacity | 1 | 0.2 |
| Conjunctival congestion | 21 | 5.2 |
| Vernal keratoconjunctivitis | 2 | 0.5 |
| Deep anterior chamber | 1 | 0.2 |
| Eccentric pupil | 1 | 0.2 |
| Cataract | 5 | 1.2 |
| Vitreous floaters | 1 | 0.2 |
| Optic atrophy | 1 | 0.2 |
| Disc pallor | 5 | 1.2 |
| Disc hypoplasia | 1 | 0.2 |
| Vertically oval disc in both eyes | 1 | 0.2 |
| Nystagmus | 7 | 1.7 |
| Externum hordeolum | 3 | 0.7 |
| Iris coloboma | 1 | 0.2 |
| Anisocoria | 1 | 0.2 |
| Congenital glaucoma | 3 | 0.7 |
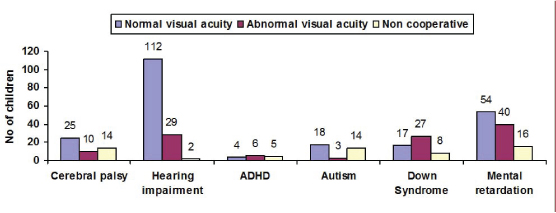
Abnormal distant visual acuity (0.1-1 logmar) was seen in 115 (28.4%) children, Normal distant visual acuity (0 logmar) was seen in 230 (56.9%) children and 59 (14.6%) children did not cooperate for vision testing. [Table/Fig-4] shows the distribution of the distant visual acuity in the better eye of children with various disabilities.
Distribution of distant visual acuity in the better eye.
Refractive errors were seen in 23.0% children with various disabilities. Hypermetropia, Myopia and Astigmatism were found in 6.7%, 13.1% and 3.2% children respectively [Table/Fig-5]. Refractive errors were seen in 50% children with Down syndrome, 46.7% with ADHD, 36.7% with Cerebral palsy, 23.6% with Mental retardation, 9.1% with Hearing impairment and 8.6% with Autism Details of ocular findings in children with various disabilities are shown in [Table/Fig-6].
Distribution of refractive errors.
| Disability (Total) | Hypermetropia | Myopia | Astigmatism | Total |
|---|
| Cerebral palsy (49) | 13 (26.5%) | 3 (6.1%) | 2 (4.1%) | 18 (36.7%) |
| Hearing impairment (143) | 0 | 13 (9.1%) | 0 | 13 (9.1%) |
| ADHD (15) | 0 | 7 (46.7%) | 0 | 7 (46.7%) |
| Autism (35) | 3 (8.6%) | 0 | 0 | 3 (8.6%) |
| Down Syndrome (52) | 5 (9.6%) | 17 (32.7%) | 4 (7.7%) | 26 (50.0%) |
| Mental retardation (110) | 6 (5.4%) | 13 (11.8%) | 7 (6.3%) | 26 (23.6%) |
| Total (404) | 27 (6.7%) | 53 (13.1%) | 13 (3.2%) | 93 (23.0%) |
Distribution of ocular findings in children with various disabilities.
| OcularDisorder | Cerebralpalsy(Total:49) | Hearing impai-rment(Total: 143) | ADHD(Total: 15) | Autism(Total: 35) | Down syndrome(Total:52) | Mental retar-dation(Total:110) |
|---|
| Refractive errors | 18(36.7%) | 13(9.1%) | 7(46.7%) | 3(8.6%) | 26(50.0%) | 26(23.6%) |
| Strabismus | 29 (59.2%) | 7 (4.9%) | 1 (6.7%) | 7 (20%) | 9 (17.3%) | 20 (18.1%) |
| Nystagmus | 24(49%) | 7 (4.9%) | 1 (6.7%) | 7 (20%) | 8 (15.4%) | 20 (18.1%) |
| Ptosis | 0 | 0 | 0 | 0 | 0 | 4 (3.6%) |
| Megalocornea | 2 (4.1%) | 0 | 0 | 0 | 0 | 0 |
| Microcornea | 0 | 2 (1.4%) | 0 | 0 | 2 (3.8%) | 0 |
| Total corneal opacity | 1 (2%) | 0 | 0 | 0 | 0 | 0 |
| Peripherial corneal infiltrate | 1 (2%) | 0 | 0 | 0 | 1 (1.9%) | 0 |
| Anisocoria | 1 (2%) | 0 | 0 | 0 | 0 | 0 |
| Eccentric pupil | 0 | 0 | 0 | 0 | 0 | 1 (0.9%) |
| Congenital Cataract | 0 | 0 | 0 | 0 | 4 (7.7%) | 1 (0.9%) |
| Optic atrophy | 1 (2%) | 0 | 0 | 0 | 0 | 0 |
| Disc pallor | 2 (4.1%) | 1 (0.7%) | 0 | 0 | 1 (1.9%) | 1 (0.9%) |
| Disc hypoplasia | 1 (2%) | 0 | 0 | 0 | 0 | 0 |
Refractive errors, strabismus and abnormal extra-ocular movements were seen in children with all six types of disabilities covered in the study. In addition, few of the children with Cerebral palsy had megalocornea, corneal opacity, corneal infiltrate, anisocoria, optic atrophy and disc hypoplasia. Microcornea and disc pallor was seen in few of the hearing impaired children. Microcornea, congenital cataract, corneal infiltrates and disc pallor was seen in some of the children suffering from Down syndrome. Some of the children with Mental retardation had ptosis, congenital cataract, eccentric pupil and disc pallor.
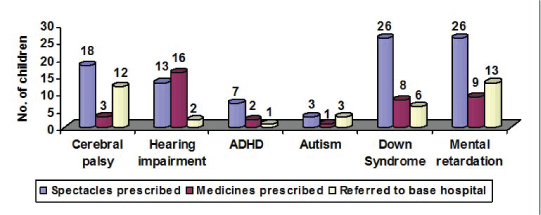
Spectacles were prescribed to 93(23%) children and medicines were prescribed to 39(9.7%) children in their respective schools/centers. A total of 37(9.2%) children were referred to base hospital for further evaluation and treatment [Table/Fig-7].
Discussion
Children with disabilities (other than visual disability) are entirely dependent on the visual inputs for their personal and educational needs. If a visual handicap gets added to their already existing disability, it will affect the overall development of the child much more than it will affect a normal child. Unfortunately, children with other disabilities are at a significantly higher risk of visual impairment [7]. Our study showed, the presence of ocular problems in 43% children with other disabilities. Ocular findings were seen in 69.3%, 25.1%, 53.3%, 25.7%, 69.2%, and 46.3% children with Cerebral palsy, Hearing impairment, ADHD, Autism, Down syndrome and Mental retardation respectively in the present study. When compared with various studies done in the past, vision problems were seen in 76% children with cerebral palsy in a study by Elmenshawy et al., [8], 24% children with Hearing impairment in a study by Gogate et al., [9], 45.3% children with learning difficulties in a study by Gogate et al., [3], 57% children with Autism in a study by Black et al., [6], 57.8% children with Down Syndrome in a study by Afifi et al., [10] and 51.45% children with mental retardation in a study by Joshi et al., [11]. Refractive errors and strabismus were the most common ocular disorders identified in our study. The literature search also supports that refractive errors and strabismus are common ocular findings in children with other disabilities [3–12]. [Table/Fig-8] compares the findings of the present study with other published studies.
Comparison of ocular problems with other studies.
| Study | Disability studied | Children examined | Ocular problems (%) | Refractive errors (%) | Strabismus (%) |
|---|
| Elmenshawy et al., [8], 2010 | Cerebral palsy | 46 | 76% | 67.2% | 32.8% |
| Present study | 49 | 69.3% | 36.7% | 59.2% |
| Gogate et al., [9], 2009 | Hearing impairment | 901 | 24% | 18.5% | 1.3% |
| Guy et al., [12], 2003 | 123 | 43.6% | 39.1% | - |
| Present study | 143 | 25.1% | 9.1% | 4.9% |
| Gogate et al., [3], 2011 | ADHD | 664 | 45.3% | 27.3% | 15.8% |
| Present study | 15 | 53.3% | 46.7% | 6.7% |
| Black et al., [6], 2013 | Autism | 44 | 52% | 27% | 41% |
| Present study | 35 | 25.7% | 8.6% | 20% |
| Aifif et al., [10], 2011 | Down Syndrome | 90 | 57.8% | 41% | 14.4% |
| Present study | 52 | 69.2% | 50% | 17.3% |
| Joshi et al., [11], 2013 | Mental retardation | 241 | 51.5% | 20.8% | 10.4% |
| Present study | 110 | 46.3% | 23.6% | 18.1% |
Refractive errors are easily corrected by prescribing spectacles. Majority of the cases of strabismus can be corrected by either surgery or spectacles. Thus, a simple and timely intervention in the form of spectacles can make a huge difference in the lives of children with other disabilities. The very fact that, majority of the causes of visual impairment like refractive errors, amblyopia and strabismus are easily treatable, signifies the need for regular ocular examination in children with disabilities [9]. The parents, caretakers and the teachers need to be sensitized and motivated for the regular ophthalmic examination of these children, even if the disability is not visual in nature. Protocols should be made regarding, mandatory vision screening at the time of admission in the schools, an annual comprehensive eye examination, early intervention and treatment if an ocular disorder is detected. The ophthalmologists can play an important role in this regard by conducting regular screening camps in special schools and rehabilitation centers. This initiative may prove to be the starting point for the establishment of the educational, social and psychological well being of these children.
Limitation
A major lacunae in this study is the inability to reach out to the children with disabilities who don’t attend the special schools and rehabilitation centers. Thus, there is a need for developing strategies for universal screening of children with disabilities, either by aiming for universal education or by encouraging community based screening camps for them.
Conclusion
The prevalence of visual impairment is higher in children with other disabilities than in normal population. Majority of the causes of visual impairment are treatable. As the children with disabilities use their visual sense to compensate for their primary disability, an early ophthalmic intervention and treatment of ocular disorders can help in the academic and social performance of these children.