Case Report
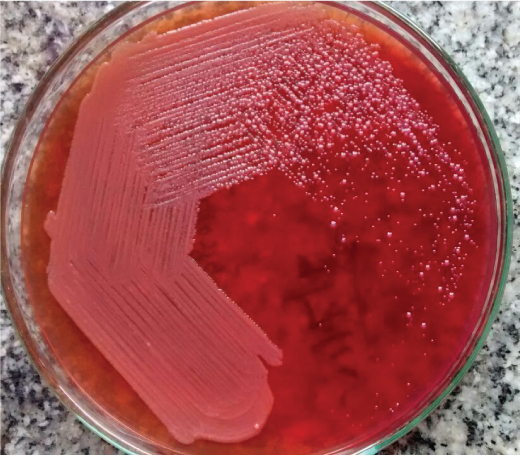
An eight-day-old male child full term/normal delivery/Small for Gestational Age (SGA) (Birth weight – 2.24 kg) was admitted for respiratory distress and fever in the Neonatal Intensive Care Unit (NICU) of All India Institute of Medical Sciences (AIIMS), Raipur, Chhattisgarh. On clinical evaluation the child was found febrile, dull and had poor respiratory efforts. Baby was non arousable and grossly hypotonic. Deep tendon reflexes were also absent. Pitting oedema was present over the dependant parts. There was no history of seizures and icterus. Baby was born in a private hospital by normal vaginal delivery and APGAR score at 1 minute and 5 minute was 3 and 5 respectively. Child received mechanical ventilation along with Inj. efcorlin, Inj. gardinal, Inj meropenem 120 mg 8 hourly and Inj. amikacin 30mg IV OD for 7 days. With this history and clinical examination of SGA with respiratory failure, the diagnosis of hypoxic ischaemic encephalopathy grade III with sepsis was established. After admission in NICU, treatment was started with maintenance of vitals, mechanical ventilation and Inj. meropenem 100mg 8 hourly and Inj colistin 100mg. The clinical samples of multiple blood, ET (Endotracheal) secretions and tip were sent for Complete Blood Count (CBC) and culture/sensitivity on various time schedules respectively. Blood and ET secretion were sent on day 1 of admission to AIIMS, prior to the commencement of antibiotic treatment and on day 9 and 17. The sample of ET tip was also received on day 6 and 9. In addition a sample of CSF (Cerebro Spinal Fluid) was received on day 2. No bronchoalveolar lavage was taken. The blood culture was done in a commercially available medium containing 50ml of Tryptone Soy broth and Bile broth(Hi-Media, Mumbai) and was incubated at 37OC with periodic subcultures on Blood Agar(BA) and MacConkey Agar(MA) after 24 hours, 3rd and 7th day or whenever any visual turbidity found. No bacterial growth after 7 days was considered sterile for respective clinical sample. ET secretion and CSF were inoculated on BA and MA and incubated for 48hours aerobically in the presence of 5-10% CO2. CSF was also inoculated in enrichment broth. Any bacterial growth was subjected to bacterial identification by conventional biochemical test and antibiotic sensitivity testing was done as per the Clinical and Laboratory Standards Institute (CLSI) guidelines, 2014 [1]. Laboratory investigation revealed a White Blood Cell (WBC) count of 20,100/μl, haemoglobin 8.2mg/dl, urea 62mg/dl, creatinine at 0.60mg/dl and C-Reactive Protein (CRP) 105.6 mg/dl. Microbiological culture of CSF on day 2 and blood and ET secretion received on day 17 were found sterile. Culture finding of blood received on day 1, 9 and ET secretions obtained on day 1, and ET tip on day 6 grew A. baumannii susceptible only to colistin and polymyxin B while resistant to penicillin, ceftazidime, cefepime, amikacin, gentamycin, ciprofloxacin, imipenem, meropenem, ampicillin-sulbactam and piperacillin-tazobactam. Gram’s stain of ET secretion and tip received on 9th day of intubation showed 4-5 polymorphonuclear leukocytes/ oil immersion field and Gram negative organism of two different morphologies i.e., Gram Negative Bacilli (GNB) and Coccobacilli (GNCB). Culture grew two types of colonies on MA and BA [Table/Fig-1]. First type was non-lactose-fermenting, mucoid and smooth colonies with a diameter of approximately 2 mm. The Gram stain showed motile GNB and biochemically was found positive for catalase, oxidase, nitrate reduction test, Ortho-nitrophenyl beta-D-galactopyranoside (ONPG), Urease, 10% Lactose and Lysine decarboxylation test. It oxidised glucose, lactose, mannitol, and maltose. It was found negative for Indole, Methyl Red, Voges Proskauer, Citrate, Bile esculin and DNAse test. It was characteristically found resistant to polymyxin B and colistin. The isolate was eventually identified as B.cepacia. The second type of colonies were of scanty growth and depicted characteristics of large pink, smooth, mucoid, catalase positive, oxidase negative, nonmotile GNCB identified as A.baumannii by biochemical tests. Biochemical identifications were further confirmed by rapid automated system- API20NE (bioMerieux, Marcy I’Etoile, France). B.cepacia was found sensitive to ciprofloxacin, cotrimoxazole, imipenem, meropenem, piperacillin- tazobactem and resistant to cefotaxime, ceftazidime, ceftriaxone, cefepime, amikacin and gentamycin. The A.baumanni isolate showed the same sensitivity pattern as exhibited by earlier isolates of A.baumanni. The child was continued on Inj meropenem and colistin with the same doses as mentioned earlier till the repeat culture was negative. Stabilization of the respiratory function and improvement of the general condition, led to extubation on 15th day of admission. The child received Inj meropenem and colistin for a total of 24 days. He remained afebrile and asymptomatic until his discharge on day 25. On follow up after 1 week, 1 and 2 months the child was doing well and gaining weight, length and head circumference.
Large pink, smooth, mucoid colonies of A.baumanii and small colonies of entire margin, slightly convex, opaque B.cepacia respectively.
Discussion
B.cepacia associated infections were increasingly reported in the last two decades especially in immunocompromised and hospitalized patients [2,3]. It is famously known as devastating pulmonary pathogen in Cystic Fibrosis (CF) and Chronic Granulomatous Disease (CGD) patients [3]. It has also been implicated in bronchiectasis, pneumonia, meningitis, peritonitis, septicaemia with significant mortality and morbidity because of high intrinsic antimicrobial resistance [2,3].
B.cepacia is an aerobic, motile, glucose-nonfermenting, multidrug resistant opportunistic nosocomial pathogen that proliferates under minimal nutritional condition and survive even lethal action of certain disinfectants [3]. It is widely distributed in the natural environment and has been isolated from water, soil, fruits, and vegetables as it survives and multiplies in aqueous hospital environments where it may persist for long periods [4,5]. B. cepacia associated infections of the bloodstream, respiratory tract, and urinary tract in Intensive Care Unit (ICU) settings has been attributed to contaminated antiseptics, disinfectants, ventilators and other types of medical equipment [4–7]. In addition, person-to-person spread has also been documented [2]. The various virulence factors of B.cepacia include siderophores, haemolysins, lipopolysaccharide which increases tumour necrosis factor alpha(TNF-α) levels over nine times more than endotoxin extracted from Pseudomonas aeruginosa to cause strong proinflammatory response leading to a necrotizing response [8]. Potential of various efflux pumps to efficiently remove antibiotics explains multi-drug resistance property of the bacteria making the treatment extremely difficult.
Similarly, A.baumannii, an opportunistic pathogen and a multidrug resistant bug has also been documented in causing various nosocomial infections including ventilator associated pneumonia, bacteraemia, urinary tract infection, secondary meningitis, skin and wound infection due to its surviving capacity for prolonged periods under a wide range of environmental conditions [9]. Erturk et al., reported the isolates of A.baumannii showing multiple drug resistance including carbapenem [9]. Such multidrug resistance demands the utmost requirement of antibiogram based treatment with appropriate sensitive antimicrobial agent for any A.baumannii associated infection.
In the present case, B.cepacia exhibited resistance to aminoglycoside, 3rd and 4th generation cephalosporin and sensitivity to fluoroquinolones, carbapenem and β-lactamase-β-lactamase inhibitor combination (piperacillin-tazobactam) and folate pathway inhibitor (trimethoprim-sulfamethoxazole). A.baumannii also showed multidrug resistance pattern with resistance to penicillin, 3rd and 4th generation cephalosporin, aminoglycoside, carbapenem, ureidopenicillin and β-lactamase-β-lactamase inhibitor combination. Sensitivity pattern of B.cepacia and A.baumannii effectively guided the treating team to continue meropenem and colistin for 24 days. The patient was treated successfully.
The dual isolation of B.cepacia and A.baumannii represented a unique and novel case of isolation from ET secretion of the neonate as previously no such report has ever been published as per our knowledge. However individual causative role of B.cepacia and A.baumannii in lower respiratory tract infection have been reported infrequently [2–13]. Despite worldwide presence, only few studies have reported the isolation of B.cepacia in India [3,4]. Gautam et al., reported the isolation of B.cepacia from septicaemic non-cystic fibrosis cases at Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh and Escorts Heart Institute and Research Centre (EHIRC), Delhi [3]. Mukhopadhyay et al., reported multidrug resistant B.cepacia from a case of multiple liver abscess in a patient with bronchial asthma and B.multivorans from a case of peritonitis in a patient with cirrhosis and hepatitis C virus infection [4]. Vishwanath et al., Dai et al., and Guzek et al., also reported multidrug resistant strain of A.baumannii as the causative agent of lower respiratory tract infection [11–13].
To determine the probable source of infection and whether it was a hospital contaminant, Hospital Infection Control Committee (HICC) was duly informed which took the subsequent relevant measure of surveillance by processing the various samples viz., betadine, cotton pack, bed side, instrument tray, swab from bed linen, disinfectant solutions, intravenous fluids, thermometers and skin swab from the patient for culture. The entire culture findings were found negative. Moreover no outbreak was reported before or after the isolation. Although the source of B.cepacia could not be identified, yet the possibility of it being hospital acquired cannot be ruled out.
The lack of infrastructure to undertake molecular methods to identify genomovars of B.cepacia by Restriction Fragment Length Polymorphism (RFLP) mediated analysis of 16S rRNA and recA and characterization of various drug resistant genes in both A.baumannii and B.cepacia has kept us in lurch of guessing the issues of genomovar and multi-drug resistant genes in our case study. Previous studies have shown that B.cenocepacia (Genomovar IIIA) is the most prevalent species of B.cepacia among a population of Indian non-CF patients which pose serious concern to health authorities due to its highest mortality and transmission rate [3]. Dai et al., have described presence of various drug resistant genes viz., OXA-23, Amp-C, TEM-1, PER-1 and SHV-2 in the A.baumannii isolates obtained from patients with lower respiratory tract infection [12].
Although we could not identify the source of dual infection, yet the isolation and identification of multi-drug resistant non-fermenters should be taken as an early alert sign in terms of hospital infection control. Immediate and strict action are required from hospital infection control committee which would include active surveillance, source identification and targeted measures like strict hand hygiene, barrier technique for colonised or infected patients, education of healthcare workers and strict implementation of appropriate antimicrobial policy based on antibiogram for effective management of any nosocomial infection.
Conclusion
The isolation and identification of B.cepacia and A.baumannii can be difficult in routine bacteriology laboratory work-up and requires high index of suspicion based on a battery of biochemical tests and intrinsic characteristic of antibiotic resistance. Isolation of these nonfermenters in any clinical setting warrants immediate initiation of appropriate antimicrobial treatment. The hospital infection control committee should also be immediately intimated so that adequate infection control measures can be implemented to significantly contain associated morbidity and mortality among in-patients.
[1]. Clinical and Laboratory Standard Institute (CLSI). 24th International supplement, M100-S24. CLSI; Wayne, PA: 2014. Performance standards for antimicrobial susceptibility testing [Google Scholar]
[2]. Karanth SS, Regunath H, Chawla K, Prabhu M, A rare case of community acquired Burkholderia cepacia infection presenting as pyopneumothorax in an immunocompetent individualAs Pac J Trop Bio 2012 2:166-68. [Google Scholar]
[3]. Gautam V, Arora A, Madhup SK, Das A, Vandamme P, Sharma K, Burkholderia cepacia complex in septicaemic non-cystic fibrosis cases from two tertiary care hospitals in North IndiaInd J Med Res 2010 131:829-32. [Google Scholar]
[4]. Mukhopadhyay C, Bhargava A, Ayyagari A, Two novel clinical presentation of Burkholderia cepacia infectionJ Clin Microbiol 2004 42:3904-05. [Google Scholar]
[5]. Matthaiou DK, Chasou E, Atmatzidis S, Tsolkas P, A case of bacteraemia due to Burkholderia cepacia in a patient without cystic fibrosisResp Med CME 2011 4:144-45. [Google Scholar]
[6]. Weinstein L, Knowlton CA, Smith MA, Cervical osteomyelitis caused by Burkholderia cepacia after rhinoplastyJ Infect Developing Countries 2008 2:76-7. [Google Scholar]
[7]. McClean S, Callaghan M, Burkholderia cepacia complex: epithelial cell-pathogen confrontations and potential for therapeutic interventionJ Med Microbiol 2009 58:1-12. [Google Scholar]
[8]. Sousa SA, Ramos CG, Leitao JH, Burkholderia cepacia complex: emerging multihost pathogens equipped with a wide range of virulence factors and determinantsInt J Microbiol 2011 2010:607575 [Google Scholar]
[9]. Erturk A, Cicek AC, Gumus A, Cure E, Sen A, Kurt A, Molecular characterization and control of Acinetobacter baumannii isolates resistant to multi-drugs emerging in inter-intensive care unitsAnnals Clin Microbiol Antimicrobials 2014 13:36 [Google Scholar]
[10]. Avgeri SG, Matthaiou DK, Dimopoulos G, Grammatikos AP, Falaga ME, Therapeutic options for Burkholderia cepacia infections beyond co-trimoxazole: a systematic review of the clinical evidenceInt J Antimicrob Agents 2009 33:394-404. [Google Scholar]
[11]. Vishwanath S, Chawla K, Gopinath A, Multidrug resistant Gram negative bacilli in lower respiratory tract infectionIra J Microbiol 2013 5:323-27. [Google Scholar]
[12]. Dai N, DZ Li, Chen JC, Chen YS, Geng R, Hu YH, Drug resistant genes carried by Acinetobacter baumannii isolated from patients with lower respiratory tract infectionChin Med J 2010 123:2571-75. [Google Scholar]
[13]. Guzek A, Rybicki Z, Korziniewski K, Mackiewicz K, Saks E, Chcialowski A, Aetiological factor causing lower respiratory tract infections isolated from hospitalized patientsAdv Exp med Biol 2015 835:37-44. [Google Scholar]