Prostatitis is a frequent urologic condition that many urologists find difficult to treat efficiently. It has been estimated that up to half of all men suffer from symptoms of prostatitis at some time in their lifetime [1]. Benign Prostatic Hyperplasia (BPH) is characterized by progressive enlargement of the prostate [2]; it is a non malignant neoplastic process secondary to increased cellular growth. BPH is one of the most common causes of Lower Urinary Tract symptoms (LUTS) [3]. LUTS correspond to a group of persistent urinary symptoms that occurs among 15% to 60% of men who are older than 40 years of age [4,5]. About half of the male population over the age of 50 can be diagnosed with histological BPH, and this prevalence increases with age to about 90% over the age of 80 [6]. As the lumen of the prostatic urethra get disturbed by fibroadenomatous enlargement in the periurethral region of the prostate, the outflow of urine is obstructed this results in an incomplete voiding of urine from bladder causing stasis and may incline the chances of infection [7]. The symptoms related to BPH is like lower urinary tract symptoms such as difficulty starting urination, a frequent need to urinate, difficulty in fully emptying the bladder, straining and dribbling [8].
Bladder Outlet Obstruction (BOO) secondary to BPH is partly due to chronic urinary retention, renal insufficiency which leads to complications like recurrent urinary tract infections, gross haematuria, and formation of bladder calculi, kidney stones and kidney failure [9].
The epidemiology of BPH and prostatitis showing male LUTS has evolved considerably in the recent past [10]. Therefore the bacterial aetiology of LUTS in the patients of BPH and/or prostatitis should be studied extensively which will help the clinicians in proper management of the condition and thus, can curb the danger of the complications associated with it.
Materials and Methods
The cross-sectional study was carried out in the Department of Microbiology from June 2014 to May 2015. The inclusion criteria included: 1) Male patients who were suspected (signs and symptoms) of LUTS were included in the study; 2) The age range of the patient included > 40 years; 3) Patients with BPH and/or Prostatitis confirmed by radiological examination, semen culture and Prostate Specific Antigen (PSA) test. The Exclusion criteria included: 1) Females were not included in this study; 2) The patients aging < 40 years; 3) Patients that were on antibiotics within last 48 hours. The study was carried out after the due ethical clearance by institutional ethical committee.
The clinical history including the signs and symptoms like frequency, urgency, hesitancy, straining, difficulty initiating the urinary stream, incomplete bladder emptying [8] etc., were collected from 105 patients during the period. The patients were subjected to Trans Rectal Ultra Sonography (TRUS) and Prostate Specific Antigen (PSA) test which confirmed the presence of BPH and/or Prostatitis.
Using purposive standard sampling technique mid-stream urine samples [11] from non-catheterized patients and catheter specimens after clamping the catheter for 30 minutes in catheterized patients were collected from a total of 105 BPH patients into sterile universal containers. Samples were processed immediately after collection. The centrifuged and uncentrifuged urine specimen was examined under 10X and 40X of bright field microscope to find out the presence of pus cells, RBCs, casts, crystals and bacterial cells were recorded accordingly. The specimens were cultured, using a standard wire loop of 4mm, on CLED, MacConkey and Blood agar (HIMEDIA, MUMBAI). The seeded plates were incubated at 37°C for 18-24 hours. Plates were examined for bacterial growth. Bacterial growths of ≥105 cfu/ml were taken to be significant. The isolates were identified by colony morphology, Gram staining, motility testing and necessary biochemical tests [12]. Antibiotic susceptibility tests were carried out by adopting Kirby Bauer method and CLSI guidelines [13]. The 1st line antibiotics (HIMEDIA, MUMBAI) for Gram negative isolates used were ampicillin (10mcg, AMP), norfloxacin (10mcg, NX), nitrofurantoin (300mcg, NIT) gentamycin (10mcg, GEN), ciprofloxacin (5mcg, CIP), cefuroxime (30mcg CRM), cotrimoxazole (25mcg COT), nalidixic acid (30mcg NA). The 2nd line and 3rd line antibiotics used against the isolates were, amikacin (10mcg, AK), ceftazidime (30mcg, CAZ), cefotaxime (30mcg, CTX), imipenem (10mcg, IMP), meropenem (10 mcg, CL), tigecycline (15mcg, TGC).
The 1st line antibiotics for Gram positive isolates used were oxacillin (1mcg, OX), cefoxitin (30mcg, CX), doxycyline hydrochloride (30mcg, DO), nitrofurantoin (300mcg, NIT), gentamycin (10/120mcg, GEN), norfloxacin (10mcg, NX). The 2nd and 3rd line antibiotics used against the isolates were teicoplanin (30mcg, TEI), ciprofloxacin (5mcg, CIP), ofloxacin (5mcg, OF), vancomycin (30mcg, VA), netilmycin (30mcg, NET), teicoplanin (30mcg, TEI) Leinezolid (30mcg, LZ). Zones of inhibition diameters were interpreted according to the guidelines (interpretation chart) provided by the manufacturer. The control strains used were Escherichia coli American Type Culture Collection (ATCC) 25922 and Staphylococcus aureus ATCC 25923.
SPSS version 21 and Microsoft office 2007 were used for data tabulation and analysis. Proportions and percentages were used as statistical measures.
Results
Out of the 105 urine specimens from the patients of BPH and/or prostatitis with LUTS, 66 (62.86%) samples showed the bacterial growth. The mean age group of the patient was 64.7 years. The most number of patients belonged to age group 65-74 years n= 30 (28.57%) followed by age group 55-64 n=28 (26.66%) and 75-84 n= 24 (22.85%). The maximum percentage of the isolates was from the specimen of age group 75-84 yrs (70.83%) followed by 65-74 yrs (70.0 %) [Table/Fig-1]. The predominant bacterial isolate were E. coli n=21(31.81%), Klebsiella species n=19 (28.78 %) followed by others as depicted in [Table/Fig-2].
The percentage of isolates from different age group of the patients of BPH and/or prostatitis.
| Age group | Number of patients | Number of isolates from the specimens | Percentage of isolated organism (%) |
|---|
| 45-54 yrs | 21 | 11 | 11/21 (52.38 %) |
| 55-64 yrs | 28 | 15 | 15/28 (53.57 %) |
| 65-74 yrs | 30 | 21 | 21/30 (70.00%) |
| 75-84 yrs | 24 | 17 | 17/24 (70.83%) |
| ≥85 yrs | 02 | 02 | 2/2 (100%) |
| TOTAL | 105 | 66 | 66/105 (62.86%) |
The frequency of bacteria isolated from the patients of BPH.
| S. No | Bacteria | Frequency and percntage (%) |
|---|
| 1 | Escherichia coli | 21/66 (31.81 %) |
| 2 | Klebsiella species | 19/66 (28.78 %) |
| 3 | Staphylococcus aureus | 11/66 (16.66%) |
| 4 | Pseudomonas aeruginosa | 07/66 (10.60 %) |
| 5 | Proteus species | 03/66 (4.54%) |
| 6 | Enterococcus species | 02/66 (3.03%) |
| 7 | Acinetobacter species | 02/66 (3.03%) |
| 8 | Citrobacter species | 01/66 (1.51%) |
| Total | 66 (100%) |
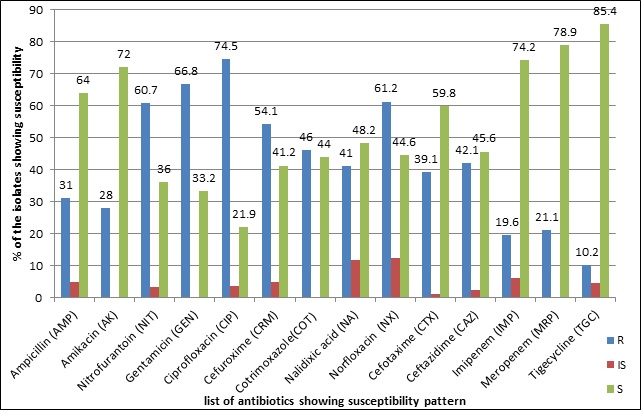
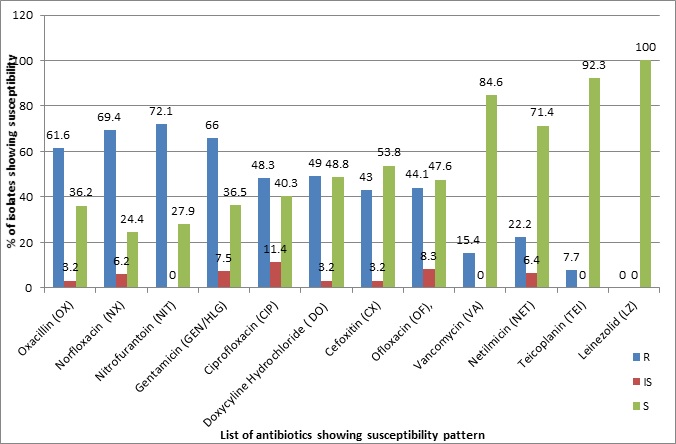
The most susceptible 1st line antibiotic for Gram negative isolates was Ampicillin (AM) 40/53 (64%), among the 2nd line was Amikacin (AK) 38/53 (72%) and 3rd line antibiotic was tigecycline 11/13 (TGC) (85.4%) [Table/Fig-3]. Amongst the Gram positive isolates, the most susceptible 1st line antibiotic was Cefoxitin (CX) 7/13 (53.8%), 2nd line antibiotic was Teicoplanin (TEI) 12/13 (92.3%) and 3rd line antibiotic was Linezolid (LZ) (97.6%) [Table/Fig-4].
Susceptibility pattern of Gram negative isolates against the different antibiotics in percentage (%).
Susceptibility pattern of Gram positive isolates against the different antibiotics in percentage (%).
Discussion
BPH and prostatitis are the most common benign diseases of the prostate gland (and probably of the entire genitourinary tract) and over time affect a considerable majority of men [14]. UTI is one of the most common infections encountered as a complication in patients of BPH [15], which affects generally elderly male of different age groups (>45 years) worldwide. We got an overall prevalence of Urinary Tract Infection (UTI) to be 62.86% among the BPH and/Prostatitis patients. This is quite higher as compared to another study which showed overall prevalence of 33% [7]. The increase can be due to variability of the number of patients in different age groups in both studies. Our study shows that the number of the pathogens isolated among the patients of BPH and/or prostatitis increases with increase in age group, the result shows prevalence of 52- 55% among patients of 45-64 years age group, 70%-71% among 65-84 years and highest of 100% among patient >85 years. These results are quite similar with the other studies, which reported prevalence of LUTS as 56% in men of 50–79 years, 70% in 80–89 years and 90% in men of 90 years of age [16,17].
In our study Escherichia coli 21 (31.81 %) was the leading cause of LUTS in patients while Klebsiella species 19 (28.78 %), Staphylococcus aureus 11 (16.66%), P. aeruginosa and Proteus spp follows the list. This is in align with the study of Oshodi et al., in 2015 which states that the Enterobacteriaceae, in particular E. coli, are the predominant pathogens in bacterial prostatitis (acute and chronic), but to a lesser extent other uropathogens are also found, e.g., Pseudomonas aeruginosa and Enterococci while the other study also shows E. coli as a prime pathogen followed by other bacteria but with some more aetiological agents [7,18]. A similar aetiology has also been reported by a study from Babylon, Iraq in 2009 [19].
Our study, shows that the most sensitive 1st line antibiotic for Gram negative isolates was Ampicillin (AMP) (64%), among the 2nd line was Amikacin (Ak) (72%) and 3rd line antibiotic was Tigecycline (TGC) (85.4%). Flouroquinolones resistant isolates especially to ciprofloxacin were (74.5%); these results are in line with the study by Oshidi AJ et al., [7]. The resistance to gentamycin and amikacin were found to be 66.8% and 28% respectively, which is quite similar to a previous study conducted in 2009 [19]. Amongst the Gram positive isolates, the most susceptible 1st line antibiotic was Cefoxitin (CX) (53.8%), 2nd line antibiotic was Teicoplanin (TEI) (92.3%) and 3rd line antibiotic was Linezolid (LZ) (100%). The resistance against the oxacillin (61.6%) and vancomycin (15.4 %) indicates the rise in resistant pathogens like Methicillin Resistant Staphylococcus aureus, Vancomycin Resistant Staphylococcus aureus and Enterococci. Among the Gram negative isolates there may be high number of ESBLs, or MBLs producing Pseudomonas aeruginosa as indicated by the resistance pattern. This may be due to the increase in the resistant strains as described in an Indian study [20]. High resistance, to the majority of the antibacterial agents tested, shown by the isolates from this study may be due to the fact that patients with BPH recurrently experience UTI which must have led the patients to the use of different antibiotics, hence development of resistant strains.
Limitation
Our study, has not used the other tests for the diagnosis of benign prostatic hyperplasia like histology and for prostatitis like 2-glass pre- and post-prostatic massage test. This test could have refined the results more.
Conclusion
LUTS are of significant importance to public health, affecting millions of older men suffering from BPH and prostatitis. The rapid increase in the prevalence of BPH and/or prostatitis and LUTS within the general population places huge burden on the management of the patients. The bacterial agents in LUTS associated with BPH are primarily the Enterobacteriaceae, less commonly Gram positive organisms and Pseudomonas aeruginosa. To manage this condition the clinicians should take into consideration the development of Multi Drug Resistance (MDR) among the aetiological agents.