Scrape cytology is a quick and effective method that can be utilised to reduce the turn-around time in providing a diagnosis. It has been used in many tissue types as an adjunct or replacement for frozen section and intra-operative consultation [1]. This technique provides the surgeon and pathologist a quick insight in to the type of lesion in question. Fine Needle Aspiration Cytology (FNAC) is a valuable diagnostic technique for thyroid lesions with diagnostic accuracy of 93.6% [2]. However, all cases of thyroid nodules may not be adequately diagnosed on FNAC due to lack of characteristic diagnostic features on aspirated material, extensive cystic changes and fibrosis leading to repeated non-diagnostic aspirates and diagnosed as suspicious and non-diagnostic of malignancy on FNAC. A subsequent histopathological diagnosis of malignancy on resection specimens usually requires a repeat surgery for completion thyroidectomy and neck dissection [3]. Such cases pose a diagnostic and management dilemma leading to inadequate resections and repeat surgeries for completion thyroidectomy. However, scrape cytology can act as a timely rescue in most such cases, especially papillary carcinoma. Frozen section of thyroid nodules is usually carried out to avoid repeat surgeries. Frozen section may not be available in all institutions especially resource limited settings. This study was carried out to determine the utility of scrape cytology in thyroid nodules; that are suspicious and non diagnostic on FNAC and as a possible replacement and adjunct to frozen section. The study was carried out on post-surgical thyroidectomy specimens received in the department.
Materials and Methods
This was a prospective study done on 50 thyroid specimens. Histopathology was the gold standard for comparison. Pre-operative FNAC diagnoses were also reviewed and recorded for comparison. Specimens received in the Department of Pathology, GMC, Srinagar, India were examined for gross nature and all findings were recorded. Scrapings were obtained from the freshly received specimen from the operating room sent in 10% buffered formalin before their fixation. After gross examination of the specimen and recording of all findings the specimen was cut with a sharp knife into two halves. Using a filter paper excess blood was wiped-off from the cut surfaces and the area most representative of the lesion was chosen for scrape. A sharp scalpel or the edge of a glass slide was used to scrape the lesion and the semi-fluid material obtained was used to prepare slides in a manner similar to FNAC slides. Smears were then labelled and immediately fixed in 95% ethyl alcohol and stained with rapid Haematoxylin and Eosin (H & E) stain. In Rapid H&E staining procedure; the fixed smears were stained with Haematoxylin for 30-45 seconds, then dipped in Eosin for 15-30 seconds and washed to remove any excess stain. Out of 50 specimen, 4 were already fixed by the time they were received in our lab. The scrapings of lesions in these cases did not yield material suitable for slide preparation. The smears which contained 5-6 groups of well preserved follicular cells with each group containing 10 or more cells were considered to be adequate for cytological study. Other variables taken in to consideration while interpreting the smears included overall cellularity (the whole slide was scanned for density of cell groups and features including cellular overlap and crowding), cell cluster morphology (whether arranged as papillae, sheets, follicles, mono-layer /multi-layered), cell size (cuboidal to columnar cells; enlarged two times), nuclear size (larger and more oval than nuclei of normal follicles), amount of cytoplasm and amount of colloid. All the resected samples were routinely processed, stained with H&E and correlation of cytological findings of scrape smears with histopathological diagnosis was carried out using descriptive statistical evaluation.
Results
A total of 50 cases of thyroid resections were evaluated during the study period and diagnosis were made on scrape smears in 46 cases. 4 cases yielded inadequate material for evaluation due to over-fixation of gross specimen.
Scrape cytology of 50 cases resulted in diagnosis shown in [Table/Fig-1].
Scrape Cytology results of 50 patients.
| Scrape Cytology | No. of cases |
|---|
| Goitre (Colloid Goitre/ Adenomatoid Nodule) | 13 |
| Follicular neoplasm | 05 |
| Hashimoto’s/ Inflammatory Thyroiditis | 02 |
| Papillary Thyroid Carcinoma (PTC) | 19 |
| Follicular Variant of PTC | 06 |
| Suspicious of malignancy | 01 |
| Non-diagnostic | 04 |
The diagnosis made on the smears included 20 benign diagnoses; including goitre [Table/ Fig-2a&b], thyroiditis [Table/Fig-3a&b], and follicular neoplasm. 26 malignant diagnoses included Papillar Thyroid Carcinoma (PTC) classic; 19 cases [Table/Fig-4a,b and c], Follicular Variant of PTC (FVPTC); 6 cases [Table/Fig-5a,b and c], medullary carcinoma; 1 case [Table/Fig-6a,b and c]. Features taken in to consideration for diagnosis of papillary carcinoma-conventional included increased cellularity, papillary fronds and nuclear features. The nuclear features were noted in all cases of papillary carcinoma (classic and follicular variant). In addition; a follicular pattern was noted with suspicion for findings of nuclear features to rule out a follicular variant of papillary carcinoma. Other features that supported diagnosis of papillary carcinoma included thick colloid, follicular giant cells and calcification.
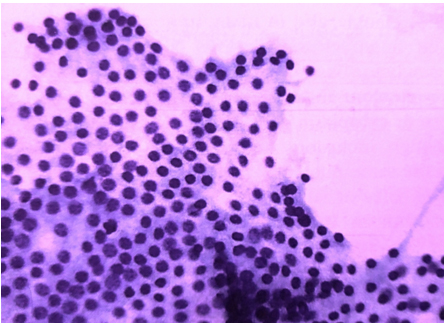
Scrape smears from a case of Colloid Goitre showing thyroid follicular cells in syncytial sheets with benign nuclear features. (H&E, 40X).
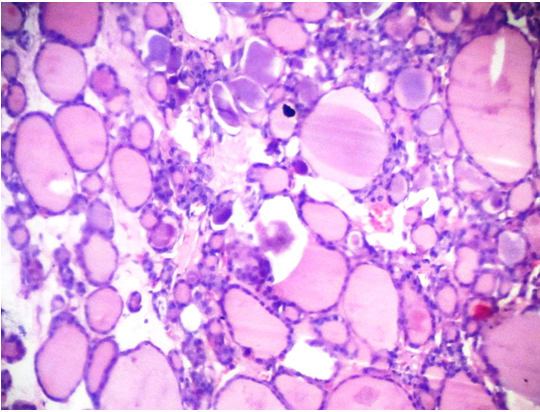
Microphotographs of the H&E stained sections of the same case (2a) as above showing variable sized thyroid follicles filled with colloid. (H&E, 10X).
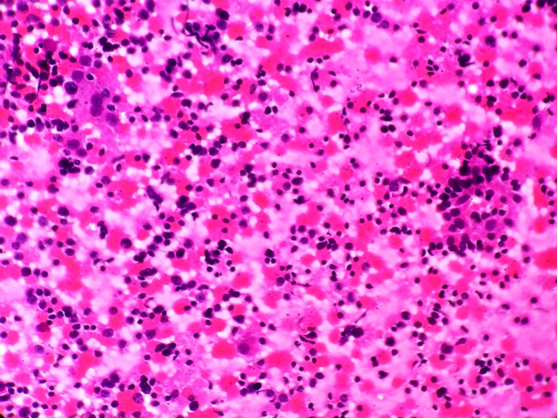
Scrape smears from a case of Lymphocytic Thyroiditis showing lymphoid cells in a cluster of thyroid follicular cells. (H&E, 40X).
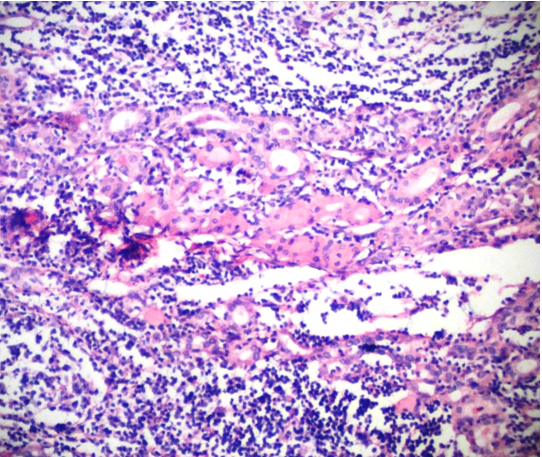
Microphotograph of the H&E stained section of the same case (3a) showing thyroid follicles entrapped in a dense lymphocytic infiltrate in the interstitium. (H&E, 10X).
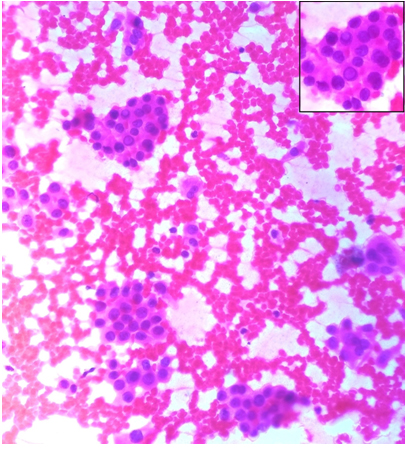
Scrape smears from a case of Papillary Thyroid Carcinoma showing sheets and papillae of follicular epithelial cells. (H&E, 10X).
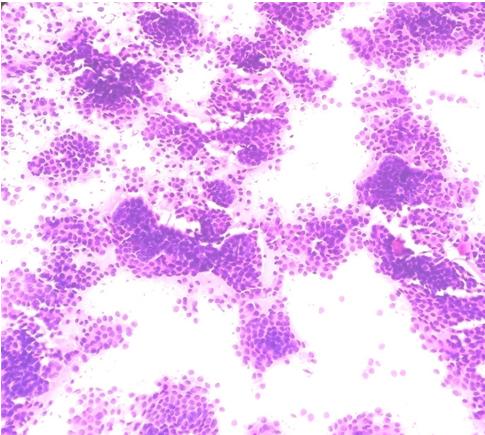
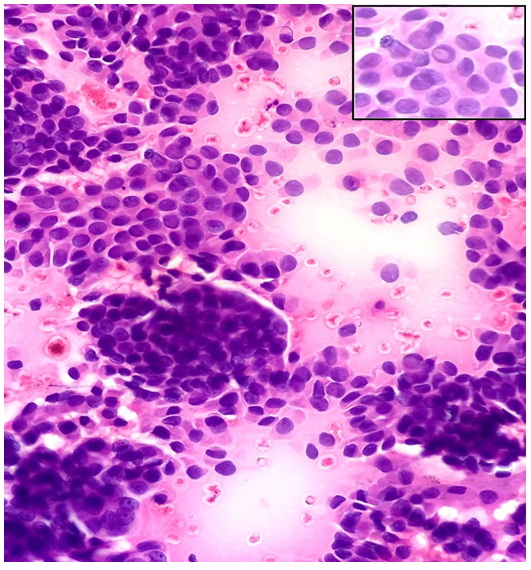
Scrape smears from the same case as above showing nuclear crowding and overlapping, dense cytoplasm with well defined borders, large pale nuclei and intranuclear cytoplasmic inclusion (INCI) (inset). (H&E, 40X).
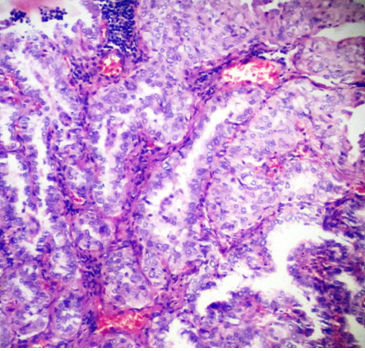
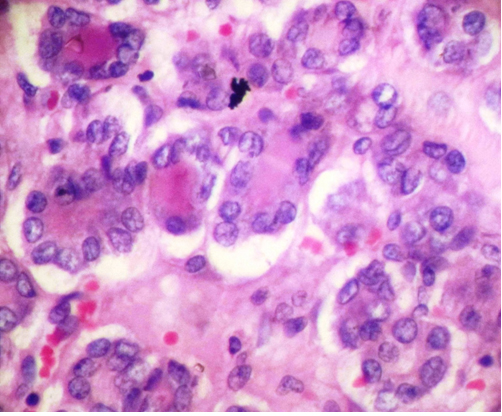
Microphotograph of the H&E stained section of the same case as above showing follicular epithelial cells forming papillae with prominent fibrovascular cores. (H&E, 40X).
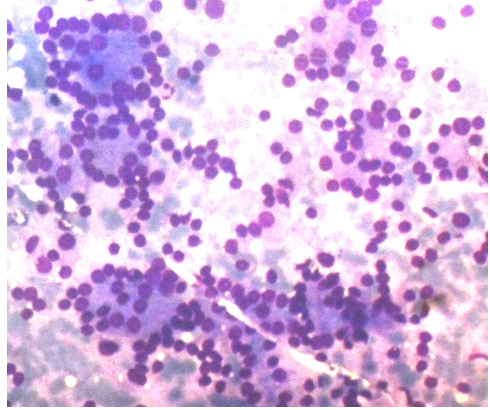
FNAC smears from a case diagnosed as Follicular Neoplasm showing syncytial cell clusters forming microfollicles in a repetitive manner. (Geimsa, 40X).
Scrape smears from the same case as above showing intranuclear cytoplasmic inclusions (INCI) (inset) in two of the nuclei and diagnosed as Follicular Variant of PTC on scrape. (H&E, 40X).
Microphotograph of the H&E stained section of same case as above showing follicular architecture with typical nuclear features of PTC (nuclear enlargement, clearing and prominent nuclear grooves) diagnosed as FVPTC on histopathology. (H&E, 40X).
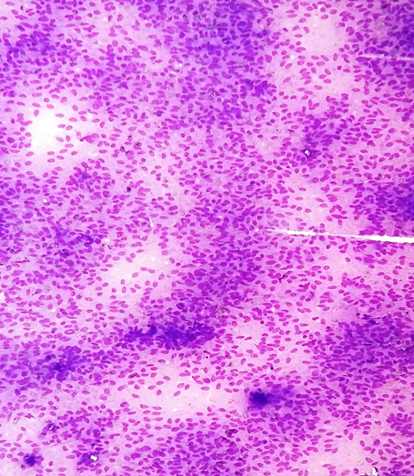
Scrape smears from a case showing hypercellular smears with round to oval cells diagnosed as suspicious of malignancy. (H&E, 10X).
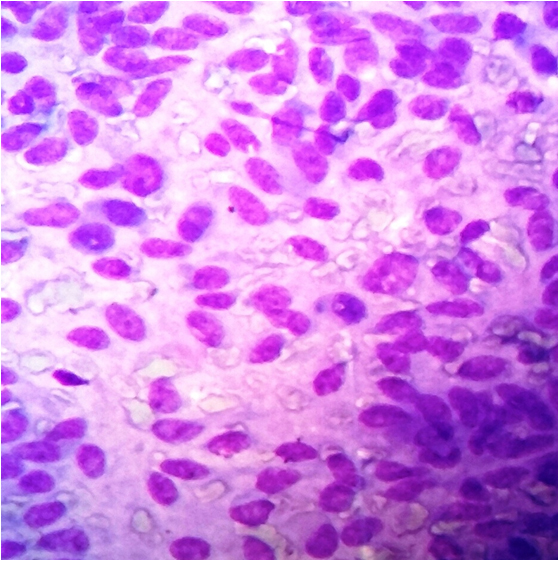
High power view of scrape smears from the same case as above showing loosely cohesive groups of cells with round to oval nuclei, little pleomorphism and “salt and pepper” type chromatin with inconspicuous nucleoli. (H&E, 40X).
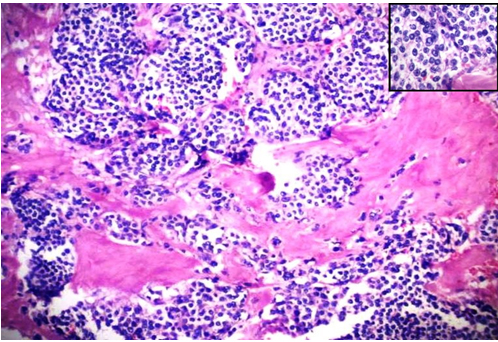
Microphotograph of the H&E stained section of the same case as above diagnosed as Medullary Carcinoma of Thyroid with extensive amyloid deposition and nuclei showing “salt and pepper” appearance (inset). (H&E, 10X).
Few cases of adenomatous goitre also showed increased cellularity; due to vigorous scraping and collections of cells that appeared to be arranged as papillae. However, there was lack of obvious nuclear changes. Criteria for diagnosis of follicular variant of papillary carcinoma taken into consideration were; flat syncytial sheets on low power with branching pattern of cells and overcrowding of nuclei, nuclear changes including; enlargement, fine chromatin, intra-nuclear cytoplasmic pseudo-inclusions and grooves. These findings were considered significant when observed uniformly in maximum number of cells. A diagnosis of follicular neoplasm was entertained in smears with cells arranged in repetitive micro-follicular pattern and scant amount of colloid in the background. The 4 cases in non-diagnostic category included smears from over-fixed samples. Over-fixation of the specimens led to distortion of nuclear details, shrinkage of cells and nuclei.
The histopathology results obtained are shown in [Table/Fig-7] and the correlation of scrape cytology with histopathology is shown in [Table/Fig-8].
Histopathology results of 50 patients.
| Histopathology Examination | No. of cases |
|---|
| Colloid Goitre and Adenomatoid Nodule | 10 |
| Follicular neoplasm | 03 |
| Hashimoto’s Thyroiditis | 02 |
| Papillary Thyroid Carcinoma | 19 |
| Follicular Variant of PTC | 11 |
| Microinvasive PTC | 02 |
| Multicentric PTC | 02 |
| Medullary carcinoma | 01 |
Correlation of cytological and histopathological diagnosis (n=50 patients).
| HistopathologicalDiagnosis → | ColloidGoiter | FollicularNeoplasm | Hashimoto’sThyroiditis | PapillaryCarcinoma | FVPTC | MicroinvasivePTC | MulticentricPTC | Medullary carcinoma | Total |
|---|
| ScrapeCytology ↓ |
|---|
| Colloid goiter/Colloid nodule | 10 | - | - | - | - | 2 | 1 | - | 13 |
| FollicularNeoplasm | - | 3 | - | - | 2 | - | - | - | 5 |
| Hashimoto’sThyroiditis | - | - | 2 | - | - | - | - | - | 2 |
| Papillarycarcinoma | - | - | - | 19 | - | - | - | - | 19 |
| FollicularVariant PTC | - | - | - | - | 6 | - | - | - | 6 |
| Suspicious ofmalignancy | - | - | - | - | - | - | - | 1 | 1 |
| Non Diagnostic | - | - | - | - | 3 | - | 1 | - | 4 |
| Total | 10 | 3 | 2 | 19 | 11 | 2 | 2 | 1 | 50 |
The scrape smear findings correlated well with histopathological findings in almost all cases except few cases with discrepancy. Of the 5 discrepant diagnoses; two cases of follicular variant of papillary carcinoma on histopathology were diagnosed as follicular neoplasm on scrape cytology. Two cases of micro invasive papillary carcinoma were misinterpreted as colloid goitre. One case of multicentric papillary carcinoma was diagnosed as adenomatous nodule. One case diagnosed as medullary carcinoma on histopathology; on scrape showed cells arranged in sheets with an obvious salt and pepper chromatin. However, this case was diagnosed as follicular neoplasm with suspicious nuclear features on scrape cytology, positive for malignancy.
Out of the 50 patients 15 were diagnosed as benign on scrape; of which 100% of cases were true negative for malignancy and five cases of malignancy on histopathology were diagnosed as benign on scrape-false negative rate of 16.1% and true positive rate of 83.8%. Histopathological correlation was available in all cases. Inadequate material was obtained in 4 (8%) cases. The overall diagnostic accuracy of scrape cytology was 89.1% with sensitivity and specificity of 83.87% (C.I.; 66.27% to 94.55%) and 100% (C.I; 76.84% to 100.00%) respectively.
FNA results were available in 41 cases of which 2 were non-diagnostic. Of the remaining 39 cases 19 were benign and 20 were malignant. Of the 30 malignant cases on histopathology 18 were diagnosed as malignant (true positive); and 12 were diagnosed as benign (false negative). In the benign group of 9 cases; 7 were diagnosed as benign and 2 were diagnosed as malignant.
On comparing scrape and FNAC; 13 diagnoses were found to be discrepant. Of these 9 cases were true positive for malignancy on scrape and false negative on FNAC (3 diagnosed as follicular neoplasm and 6 as colloid goitre). The rest of the 4 discrepant cases were diagnosed correctly as malignant on FNAC whereas, benign on scrape (2 colloid goitre, 2 inflammatory)
Scrape cytology was also found to be of benefit in cases of PTC diagnosed as suspicious and negative for malignancy on FNAC; 6 cases and follicular variant of papillary carcinoma diagnosed as follicular neoplasms on FNAC; 3 cases. The need for a repeat surgery for completion thyroidectomy could have been obviated in these nine cases; had a diagnosis of malignancy been offered by intra-operative scrape cytology.
Discussion
Cytopathology as a science has been recognized and implemented as a diagnostic tool as early as the 18th and 19th centuries. However, the progress and the standardization of this branch of pathology were seen only in the late years of the 20th century [4–6]. The art and practice of cytopathology is emerging as a standard procedure for initial diagnosis of many lesions, overcoming the limitations that it faced at the time of its inception. In the present times FNA is widely used as an inexpensive, simple, accurate and a safe procedure for making a specific and reliable diagnosis that helps the treating clinicians to tailor the management protocols of the individual patients [7,8].
FNAC of thyroid gives valuable information about the nature of the lesion and most patients can be managed adequately on an optimal FNAC diagnosis [8]. However, some lesions may not be diagnosed on FNAC. To bridge the gap between the non-diagnostic FNAC’s and final histopathological diagnosis; many techniques have been employed to give additional information that helps in better management decisions. Intraoperative consultation is of importance in such cases. Frozen sections can give valuable information intra operative. However, frozen section might not be available in all centres. A plausible alternative to this modality is scrape cytology. In our study 4 of the patients of papillary carcinoma had to undergo a follow up thyroidectomy and neck dissection due to a benign diagnosis on FNAC. Three cases of follicular variant of papillary carcinoma thyroid diagnosed as follicular neoplasm on FNAC was correctly identified as FVPTC on scrape cytology. Several studies have advocated the use of frozen section along-with intra-operative cytology to determine the extent of thyroid resection [9]. Whereas cases with a diagnosis of “suspicious for papillary carcinoma” on FNAC may benefit a lot by utilising scrape cytology for intra-operative consultation and obviate the need for a repeat procedure/ follow-up completion thyroidectomy. Some studies have found that, scrape preparations from surgically removed thyroid nodules had an efficacy of 98%; as compared to frozen section with efficacy of 71% [10].
Scrape cytology can also be utilised to support the diagnosis offered on frozen section with the advantages of being less time consuming, easy to adopt, reliable and without need of any special equipment [11–13]. We made scrape preparations from the nodules and stained them with rapid H&E to reduce the time of staining. Some studies have used rapid ultrafast Papanicolaou- stained scrape preparations and found good results [14]. Diff Quick and Papanicolaou stained smears improve the diagnostic accuracy of FVPTC by enhancing the nuclear features like nuclear grooves, powdery chromatin and intra-nuclear pseudoinclusions [15,16].
Scrape preparations of specimens done as a routine at the grossing station can help in learning and teaching cytological features of tumors and can improve interpretation skills of FNAC [17–19]. It has been utilised as a tool for intraoperative diagnosis in many studies for tumours of various sites [20].
In our study we found excellent results for diagnosing benign thyroid lesions; with all lesions benign on histopathology, were also diagnosed as benign on scrape cytology. Malignant lesions also were diagnosed satisfactorily with a true positive rate of 83.3%.
Limitation
There were limitations of scrape cytology in the diagnosis of over-fixed and small tumours (micro-papillary carcinoma), which require histologic architectural evaluation and adequate histologic sampling.
Conclusion
We conclude that scrape cytology can act as a useful adjunct to FNAC and is a good procedure for intra-operative consultation. It is especially helpful in neoplasms diagnosed as suspicious for papillary carcinoma on aspiration and may obviate the need for a second procedure for completion thyroidectomy. Scrape cytology is a simple, rapid, and inexpensive adjunctive technique that should be used in intra-operative consultation for thyroid lesions.