Study showed that among Indians, both abdominal and central obesity are present in male and female [10]. Generalized obesity is more in male and abdominal obesity in female. Also, studies showed that Asian Indians have some special features of obesity regarding effect of excess body fat [11]. The limits of normal Body Mass Index (BMI) are reduced in Asian Indians than in white Caucasians considering percentage body fat. The obesity is generally measured by BMI. BMI greater than or equal to 25 kg/m2 is considered as overweight and greater than or equal to 30 kg/m2 is obesity by WHO. However, for Asian population the BMI cut-off points are much lesser and BMI between 23 to 25 kg/m2 is considered as overweight and above 25 kg/m2 is considered as obese [12,13].
Generally obesity is considered as unbalance of energy intake and energy expenditure. The excessive intake of sugar and junk food causes deposition of fat [14]. Obesity is also linked to behavioural changes and social networks [15]. The mechanism of development of obesity is not completely understood but causes are many like stress, environmental, behavioural, lifestyle, genetic factors etc., [16,17].
The present solutions for reduction and prevention of obesity are limited and have adverse effects [6]. Hence, it is prudent to explore the treatments from alternative therapies like yoga, pilate, tai-chi, etc. The psychological stress will be reduced by yoga as per its definition in the Patanjali yoga sutras [18]. Yoga is defined as inhibition of modification of thoughts [19]. The mental stress is closely related to psychosomatic diseases and yoga practice is useful for reduction of stress [20]. Also earlier studies showed that Yoga will help to increase awareness on satiety and sense of overeating [21]. There are short term studies showing the usefulness of Yoga practices for weight reduction [22]. However studies of the long term yoga training for weight reduction along with weight related psychological parameters were not found. The aim of the present study was to find out the effect of 14 weeks Integrated Approach of Yoga Therapy (IAYT) practice on male obesity parameters in urban setting.
Materials and Methods
Participants
The study was a parallel group study with yoga and control groups. The yoga group was given the intervention of yoga training.
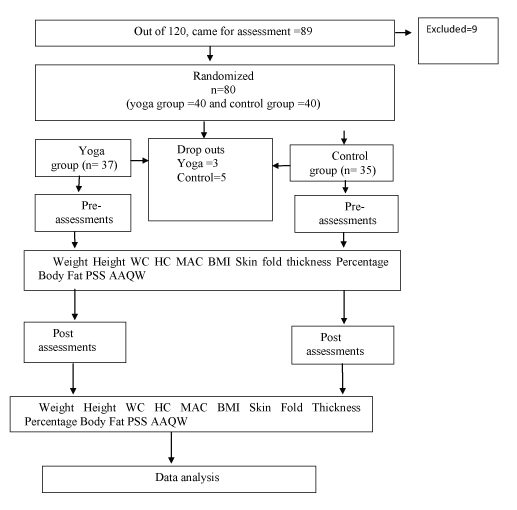
There were total 120 subject who showed desire for joining the research when contacted through advertisement. The subjects were living in Mumbai. They were mostly employees or family members of employees near Anushaktinagar of Mumbai. Total 80 enrolled based on selection criteria. Randomization with minimization of co-factors was done. Total 40 subjects were assigned in yoga group and 40 in control group. The minimization was done using open source software of Minim Py to have balance between groups [23,24]. It is reported that minimization is effective and is desirable in RCTs [25]. These were groups of age (18 to 40 and 41 to 60) and groups of education (up to graduates and post-graduates/ above). The trial profile is given in [Table/Fig-1].
Sample Size
The sample size was calculated based on previous study using G*Power software [26,27]. Out of four primary outcomes variable HC (hip circumference) had lowest effect size and this was considered to calculate sample size in the current study and got minimum sample size as 29.
Ethical Clearance
Approval of institutional ethical committee was obtained.
Informed Consent
Informed consent was taken from participants prior to recruitment.
Screening
Screening for obesity was done based on BMI as per selection criteria. Selection criteria was BMI from 23 Kg/m2 to 35 Kg/m2, Gender male, age 18 to 60years and having normal health conditions except obesity. Each individual was given an alphanumeric code and removing personal identifiers.
Intervention
The IAYT consisting of Asanas, Pranayama, Relaxation and Meditation techniques were introduced in a slow step by step manner. Each session of the intervention was for 90 minutes for five days in a week for 14 weeks. Details of the yoga intervention are provided in [Table/Fig-2].
The five part IAYT intervention.
| Part No | Yoga Practice | Duration (minutes) |
|---|
| 1 | Lecture & Counselling | 10 |
| 2a | Warm Up | 10 |
| 2b | Suryanamaskara | 10 |
| 3 | Asana | 30 |
| 4 | Pranayama | 15 |
| 5 | Meditation | 15 |
| Total duration | 90 |
No specific physical activity was given to control group but asked to continue their regular physical activities which they have been practicing. The intervention was done during March to June in 2015.
Components across both the groups:- Participants received their respective measurement values and a food log format and basic sample meal plan for sedentary male adults based on guidelines of NIN (National Institute of Nutrition Hyderabad) [28].
Assessments
The assessments were wt.(Body Weight), BMI (Body Mass Index), MAC (Mid Upper Arm Circumference) for both right and left upper arms, WC (Waist Circumference), HC (Hip Circumference), WHR (Waist Hip Ratio), ABSI (A Body Shape Index), SKF (Skin Fold Thickness) at 4 body points applicable for male [29]. These were at right upper arm biceps (SKFraf) right upper arm triceps (SKFrab), sub scapular (SKFshob), suprailiac (SKFstof). Percentage body fat was based on cumulative skin fold thickness SKF from table applicable for male [30].
The PSS (Perceived Stress Scale) and AAQW (Acceptance and Action Questionnaire in Weight related difficulties) were assessed [31–33]. The same scales were used for pre and post assessments. The weight was measured using electronic weighing scale. For height inelastic measuring tape and ruler were used and subjects stood against the wall. Waist circumference was measured at the midway between the lowest rib margin and iliac crest and hip circumference at the widest trochanters, with inelastic tape. The standard skin fold caliper was used to measure skin fold thickness [29,34].
Statistical Analysis
The data was analysed using SPSS software 21 version. Normality test was done using Shapiro wilk test. The paired sample t-test was done for pre-post for both groups on all the variables which were found normally distributed. For not normally distributed parameters, Wilcoxon signed ranks test was done. Between groups analysis was done using independent sample t-test for the post values of the groups. Correlation of differences from post to pre readings, among the variables was carried out. A value of p<0.05 was considered statistically significant.
Results
The baseline demographic data of age and height of the yoga and control group are given in [Table/Fig-3]. Results of within group analysis of the anthropometric and psychological parameters are given in [Table/Fig-4a,b]. Between group analysis results are given in [Table/Fig-5]. The pre-post change in each variable was co related with each other and given in [Table/Fig-6].
Baseline data of age and height.
| Variable | Yoga group n=37 | Control Group n=35 |
|---|
| Pre | 95% CI | Pre | 95% CI |
|---|
| Age | 40.03±8.74 | (37.12-42.94) | 42.20±12.06 | (38.76-46.89) |
| Height | 169.45±7.35 | (167.00-171.90) | 169.29±6.37 | (167.17-171.65) |
Within group analysis results.
| Variables | Yoga group n=37 | Control group n=35 |
|---|
| Pre | Post | t | Sig | Pre | Post | t | Sig |
|---|
| Weight- wt | 82.63±10.05 | 81.51±10.00 | 3.1 | 0.004 | 79.45±8.85 | 79.22±8.93 | 0.94 | 0.353 |
| MAC left arm -macl | 29.98±2.02 | 29.42±1.92 | 2.53 | 0.016 | 32.53±16.53 | 28.10±1.70 | 1.61 | 0.118 |
| MAC right arm - macr | 30.18±2.04 | 29.64±2.04 | 2.48 | 0.018 | 32.47±16.73 | 28.10±1.85 | 1.57 | 0.125 |
| Hip circumference-HC | 103.50±5.71 | 101.29±4.95 | 5.39 | <0.001 | 104.28±6.60 | 101.38±6.13 | 4.54 | <0.001 |
| Triceps-SKF right arm back side- Rab | 19.05±7.01 | 17.87±5.05 | 0.89 | 0.379 | 13.70±6.57 | 13.22±4.24 | 0.45 | 0.652 |
| Suprailiac-SKF at stomach front side- Stof | 32.45±7.82 | 28.04±5.45 | 3.29 | 0.002 | 27.46±9.37 | 25.57±7.06 | 1.15 | 0.259 |
| Sub scapular-SKF shoulder back side-Shob | 27.87±6.97 | 26.91±5.23 | 0.86 | 0.396 | 21.76±7.11 | 22.28±4.98 | -0.38 | 0.707 |
| BMI | 28.7±2.35 | 28.33±2.42 | 2.82 | 0.008 | 27.70±2.05 | 27.61±2.01 | 1.04 | 0.306 |
| ABSI | 0.08±0.00 | 0.08±0.00 | 0.97 | 0.337 | 0.08±0.00 | 0.08±0.00 | 4.02 | <0.001 |
| SKF cumulative | 93.93±22.56 | 85.52±13.38 | 2.23 | 0.032 | 73.65±20.61 | 72.17±14.55 | 0.4 | 0.693 |
| PSS | 16.51±6.12 | 12.59±6.65 | 3.83 | <0.001 | 14.29±6.51 | 13.51±5.95 | 0.69 | 0.493 |
| AAQW-aaqw | 81.24±17.35 | 71.54±14.62 | 3.9 | <0.001 | 73.11±14.80 | 69.71±16.28 | 1.24 | 0.224 |
Within group analysis results-Non parametric.
| Variables | Yoga group n=37 | Control group n=35 |
|---|
| Pre | Post | Z score | Sig asymp. sig (2-tailed) | Pre | Post | Z score | Sig asymp. sig (2-tailed) |
|---|
| WC | 99.58±7.37 | 98.25±7.12 | -2.06b | 0.039 | 99.28±6.82 | 95.79±8.33 | -3.71b | <0.001 |
| Biceps-Raf | 14.55±7.19 | 12.70±5.02 | -1.42b | 0.156 | 10.72±5.00 | 11.10±3.69 | -0.672c | 0.502 |
| WHR | 0.96±0.04 | 0.97±0.05 | -1.82c | 0.069 | 0.95±0.06 | 0.94±0.06 | -0.82b | 0.413 |
| Percentage Body Fat (PFC) | 30.78±4.37 | 29.66±3.30 | -1.96b | 0.051 | 27.55±5.17 | 27.58±5.29 | -0.03c | 0.98 |
a-Wilcoxon signed ranks test
b-based on positive ranks
c- based on negative ranks
| Variable | Yoga - Post-Mean Std devn=37 | Control Post-Mean Std devn=35 | t | Sig (t tailed) | Diff. in Mean 95%CI lower/Upper |
|---|
| Wt | 81.51±10.00 | 79.22±8.93 | 1.02 | 0.31 | 2.29 (-2.17- 6.76) |
| MACL | 29.42±1.92 | 28.10±1.70 | 3.07 | 0.003 | 1.32 (0.46-2.17) |
| MACR | 29.64±2.04 | 28.10±1.85 | 3.35 | 0.001 | 1.54 (0.62- 2.46) |
| HC | 101.29±4.95 | 101.38±6.13 | -0.07 | 0.945 | -0.09 (-2.70 – 2.52) |
| Triceps-Rab | 17.87±5.05 | 13.22±4.24 | 4.22 | <0.001 | 4.65 (2.42- 6.85) |
| Suprailiac-Stof | 28.04±5.45 | 25.57±7.06 | 1.66 | 0.101 | 2.47 (-0.49 -5.42) |
| Sub scapular-Shob | 26.91±5.23 | 22.28±4.98 | 3.85 | <0.001 | 4.63 (2.23 -7.04) |
| BMI | 28.33±2.42 | 27.61±2.01 | 1.37 | 0.175 | 0.72 (-0.33 -1.77) |
| Cumulative skin fold-Skft | 85.52±13.38 | 72.17±14.55 | 4.06 | <0.001 | 13.35 (6.79 – 19.91) |
| PSS | 12.59±6.65 | 13.51±5.95 | -0.62 | 0.539 | -0.92 (-3.89 -2.05) |
| AAQW | 71.54±14.62 | 69.71±16.28 | 0.5 | 0.618 | 1.83 (-5.44-9.09) |
Correlations among (n=72) variable.
| WT | MACL | MACR | WC | HC | RAF | RAB | STOF | SHOB | BMI | WHR | SKFT | PFC | PSS | AAQW |
|---|
| WT | 1.00 | | | | | | | | | | | | | | |
| MACL | -0.03 | 1.00 | | | | | | | | | | | | | |
| MACR | -0.02 | 0.995** | 1.00 | | | | | | | | | | | | |
| WC | 0.366** | 0.10 | 0.10 | 1.00 | | | | | | | | | | | |
| HC | 0.234* | 0.08 | 0.08 | 0.396** | 1.00 | | | | | | | | | | |
| RAF | 0.00 | -0.03 | -0.04 | 0.05 | -0.02 | 1.00 | | | | | | | | | |
| RAB | -0.11 | -0.07 | -0.07 | -0.05 | -0.05 | 0.691** | 1.00 | | | | | | | | |
| STOF | 0.12 | -0.01 | -0.03 | 0.08 | 0.04 | 0.420** | 0.18 | 1.00 | | | | | | | |
| SHOB | 0.07 | -0.04 | -0.03 | 0.09 | 0.02 | 0.352** | 0.277** | 0.456** | 1.00 | | | | | | |
| BMI | 0.993** | -0.03 | -0.02 | 0.359** | 0.231* | -0.01 | -0.10 | 0.11 | 0.06 | 1.00 | | | | | |
| WHR | 0.201* | 0.04 | 0.05 | 0.770** | -0.275** | 0.06 | -0.03 | 0.04 | 0.07 | 0.196* | 1.00 | | | | |
| SKFT | 0.04 | -0.05 | -0.06 | 0.06 | 0.00 | 0.813** | 0.697** | 0.735** | 0.708** | 0.03 | 0.05 | 1.00 | | | |
| PFC | 0.12 | -0.04 | -0.05 | 0.11 | 0.02 | 0.736** | 0.630** | 0.727** | 0.714** | 0.11 | 0.09 | 0.953** | 1.00 | | |
| PSS | 0.18 | -0.279** | -0.281** | 0.01 | 0.09 | -0.02 | -0.08 | -0.01 | 0.05 | 0.17 | -0.05 | -0.02 | -0.06 | 1.00 | |
| AAQW | 0.15 | -0.01 | 0.01 | 0.06 | -0.02 | 0.00 | 0.03 | -0.07 | 0.09 | 0.15 | 0.06 | 0.01 | -0.01 | 0.215* | 1.00 |
*. Correlation is significant at the 0.05 level (1-tailed).
**. Correlation is significant at the 0.01 level (1-tailed).
WT: weight MACL: Mid arm circumference left
MACR: Mid arm circumference right
WC: Waist circumference
HC: Hip circumference
AF: Biceps skin fold thickness
RAB: Triceps skin fold thickness STOF: Suprailiac skin fold thickness
SHOB: Sub scapular skin fold thickness
BMI: body mass index WHR: Waist hip ratio
SKFT: Cumulative skin fold thickness
PFC: Percentage body fat
PSS: Perceived stress scale score
AAQW: Action and weight relayed difficulty score
The minimum age in yoga group was 26 and maximum 60 whereas in control group minimum was 21 and maximum was 58 years. The BMI of yoga group ranged from 25.33 to 34.84 with the mean ±SD 28.7±2.35. BMI of control group ranged from 25.01 to 33.64 with the mean ±SD 27.70±2.05. The demographic, educational and anthropometric data were similar in both groups. In each group, out of 40 subjects, 20 were between 10th standard to graduates and 20 were post graduates or higher qualified. In each group number of subjects with age between 18 to 40 was 20 and age between 41 to 60 was 20. In each group all the subjects were working and all were having BMI above 25 Kg/m2.
The yoga group attended yoga training for 14 weeks and average attendance percentage was 66, 61, 53 and 49 at the completed weeks of 6, 8, 12 and 14 respectively. The control group continued their physical activities.
Anthropometric Parameters
The pre and post-data of the anthropometric parameters were compared. It was found that the weight of the yoga and control groups decreased after the intervention. The weight (wt) reduction in yoga group was significant (p<0.004) and reduction in control group was not significant.
The MACs of both left and right arm were reduced in both Yoga and Control groups. In yoga group left MAC change was significant (p<0.02) and in control group it was not significant. Similarly right MAC of yoga group was reduced and change was significant (p<0.02) and change in control group was not significant.
The WC, Right arm front side SKF, WHR and Percentage body fat based on SKF were not normally distributed. The Bicep SKF and the percentage body fat reduced in yoga group and WHR reduced in control group but were not significant.
The WC in both groups were significant (Yoga p<0.04 & Control p<0.001). The reduction HC was significant in both groups (Yoga p<0.001 and Control p<0.001).
The BMI was reduced in both groups but reduction was significant in yoga (p<0.01). The body shape index ABSI was also calculated based on WC height and BMI [35–37].
The change in cumulative skin fold thickness was significant in Yoga group alone (p<0.05). However, among the 4 separate measurements of SKF, in yoga group alone, suprailiac SKF change (reduction) was significant (p<0.002). In both groups all the 4 SKF values were reduced except that in control group the sub scapular skin fold thickness and Biceps Raf increased. Also, percentage body fat reduced only in Yoga group (p=0.051) and in control group it was increased but not significant.
Psychological Parameters
The PSS score improvement was significant (p<0.001) in Yoga group alone and in Control group score was improved but change was not significant.
In Yoga group, AAQW score improvement was significant (p<0.001) and in Control group score was improved but not significant.
Regarding relative improvements among the variables, weight was positively correlated with HC (r =0.234, p<0.02), WC(r=0.366, p<0.01), SKF suprailiac (r=0.12, p<0.16), PSS score (r= 0.18, p<0.07) and AAQW score (r=0.15, p<0.10). The left MAC was negatively correlated with PSS (r=-0.28, p<0.01) but there was no significant correlation with AAQW.
Also, right MAC was negatively correlated with PSS (r=-0.29, p<0.01) and there was no correlation with AAQW.
SKF suprailiac and SKF sub scapular had positive correlation (r=0.46, p<0.001), triceps and sub scapular skin fold had positive correlation (r=0.28, p<0.01). BMI and HC had positive correlation (r=0.23, p<0.03). PSS was correlated positively with AAQW scores (r=0.22, p<0.04).
In the between group analysis, changes in weight, HC, suprailiac, BMI, PSS and AAQW difference in scores were not significant. The left & right MAC, triceps skin fold thickness, sub scapular skin fold thickness, cumulative skin fold thickness were significant. All values of control group were lesser than yoga group except HC & PSS. None of the subjects reported adverse events during the intervention. This was asked during each session.
Discussion
Most of the anthropometric parameters and all the psychological parameters were improved in Yoga group. Also, in the control group there was improvement. The weight reduction in yoga group was significant (p<0.004) but not in control group. The MACs were reduced in both the groups but reduction was significant in yoga group (p<0.02). The WC (p<0.04) and HC (p<0.001) were reduced in yoga group.
In an earlier study of a two week residential yoga intervention, improvement was noted in the anthropometric parameters on obese male and female participants [38]. The BMI, WC, HC were reduced and reductions were significant. The WHR was not changed in this study and also in another short term yoga and diet change study, on obesity [38,39]. This showed that there was no difference in reduction of fat in the waist and hip. In the current study WHR showed increasing trend, but the change was not significant.
This shows that in the current study, the reduction of fat in Yoga group resulted in more reduction in hip area than in waist area and in Control group more reduction in waist than in Hip. The yoga practices were containing practices for reduction of fat in both waist and hip areas. This included warm up and suryanamaskara as given in the part 2a &2b of the 5 part IAYT yoga module intervention [Table/Fig-2]. The control group also continued to do physical activities which might have resulted in improvement in their anthropometric parameters. They were asked to continue their regular physical activities and also they were given their respective assessment readings and sample food plan details.
The reduction in MAC of both left and right upper arm was significant in Yoga group. The previous studies on obesity and yoga on adults also included the MAC measurement as a part of anthropometric parameters [39]. But in the current study both left as well as right MAC were measured.
In the current study control group MAC was reduced but not significant. In earlier study of short duration, found decrease in MAC and concluded that the reduction may be due to reduction in muscle or skin layer as muscle circumference was not measured separately [39]. In previous study the MAC reduction was significant in control group alone [38]. This could be due to the short duration of 2 weeks intervention among other factors if any. In the current study, in Yoga group for both left and right MACs were improved with significance which shows the effectiveness of the module of Asanas involving arms and shoulder.
In the current study the cumulative skin fold thickness SKF (involving 4 measurements) reduction was significant in yoga group and in Control group there was decrease but not significant. Further the SKF of biceps and triceps were reduced in yoga group but these values were not significant. In both groups all the 4 skin fold thickness values were reduced except in Control group sub scapular and biceps raf were increased. This may be due to lack of physical activities involving hand and shoulder muscles by the Control group. It is also noted that anthropometry and skin fold thickness are best predictors for obesity assessments [40]. SKF reduction was significant in suprailiac [stomach side] of Yoga group alone, out of all 4 SKFs. Also in Yoga group alone the percentage body fat reduced and with significance (p=0.051). This shows that the IAYT yoga intervention is effective in reducing the fat and also reduction at different sites for male.
In psychological instruments PSS and AAQW were used. There was difference in stress levels in PSS and AAQW base values of groups. The PSS is one of the widely used validated scales to assess the psychometric properties evaluated mostly using college students or workers [31]. In the current study all subjects were working. The PSS is used for measuring perception of stress [41]. In the current study the PSS reduced in both groups but reduction was significant in yoga group alone. The yoga practices were shown to reduce psychological distress in obese in earlier studies [26]. The current study is one of the earliest studies, combining components of anthropometric PSS and AAQW [33]. The AAQW is a 22 item questionnaire for assessing experience based avoidance and psychological inflexibility associated with obesity and obesity factors such as food. The score was reduced in both the groups. Earlier study (both male/female) of 24 weeks showed that greater decrease in weight related experiential avoidance was linked to more weight loss [42]. The current study of only male subjects, also confirms this point. In the current study, the decrease of AAQW score is significant in Yoga group. Hence after the IAYT intervention the experiential avoidance is reduced in Yoga group which also confirms the reduction of stress levels including acceptance of difficult emotions of obese.
Earlier studies showed that 10 days of short term yoga interventions involving Asana, Pranayama, Relaxation techniques give anxiety reduction [43]. Also, previous studies showed that the long term, 2 years yoga practices reduce the mood changes and stress related bio chemical indices [44]. Also, previous residential weight reduction yoga study did not show significance in mood disturbance, when assessed at 3 month follow-up [45]. In current study, improvement in scores in both PSS and AAQW were significant in Yoga group. This may be due to the effect of different relaxation techniques used in intervention namely MSRT (Mind Sound Resonance Technique), OM meditation Cyclic meditation and Savasana.
This is one of the studies exclusively on male population and more than 3 months in an urban setting. The psychological stress is found to increase cortisol secretion and abdominal fat in an exploratory RCT on female [46]. The mindfulness training improves the eating pattern and reduces the fat. The current study also support that the reduction of abdominal fat on male is consistent with reduction in perceived stress. The suprailiac skin fold (stomach front side fat) reduction was significant in yoga group but not in control group.
The between group analysis, (significance on cumulative SKF, triceps, sub scapular, MACs) showed the improvement in the fat reduction in the respective areas in yoga group.
It was found that PSS and weight related psychological inflexibility are positively correlated. In previous study with n=272 & both male and female, weight was positively correlated with HC (r=0.21, p<0.01) where as in current study (r =0.234, p<0.02) [26]. This supports that weight and HC in male alone also similarly correlated. The weight and WC are positively correlated WC (r=0.366, p<0.01) in current study whereas in earlier study correlation is (r=0.22, p<0.0001) [26]. This supports the higher positive correlations of body weight with HC & WC in male obesity similar to previous mixed studies. Also, it is found that there is positive correlation of weight with SKF suprailiac. The SKF suprailiac and sub scapular are positively correlated. This may be due to the similar increase in fat deposition in trunk portion.
Strengths Limitations and Future Scopes
This is an exclusive study on urban male obesity with psychological parameters. This study has compared the variable of anthropometric and scores of PSS and AAQW together. It is found that IAYT is effective for reducing obesity and problems related to avoidance and inflexibility among obese.
Large age variation of subjects was found as a limitation which was considered initially to get more sample size for the longer duration of intervention. However, the urban environment of life style such as easy availability of junk food, occupational stress (all subjects were working) etc., were common for all the subjects. Further both the groups were having similar age variation as minimization of co factors was done. Blinding on the intervention was not possible since the sample were mostly from same locality and once the intervention started the control group were aware of the yoga programme though subtle practical details were not known to them. Also the individual assessment parameters including the food log format and sample food plan were available with control group also. This might have also given them some motivation to do regular physical exercise and walking activities. This might have improved their anthropometric and psychological parameters.
In Yoga group dropouts were minimum due to interactions and lecture sessions as part of the IAYT module. Lecture was on the designated topics of IAYT module with chance for clarifying the doubts to participants.
It was reported that people with interest and some belief in benefit of yoga are more likely to join the yoga studies than who are indifferent to yoga [21]. This may be applicable In the current study also, since subjects were having initial interest and enthusiasm in joining yoga training.
There is scope for future research with different cross-sections of male obesity with adolescence, middle age and beyond, as separate groups. Also overweight and different grades of male obesity in the urban setting can be studied. In the current study on urban setting of Mumbai, the subjects had commonality of food habits, easy availability of junk food, and economic capability since all were working. The social economic and the city environment affects positively to obesity and different grades of obesity can be taken for different studies.
The maintenance of accurate food log plays a vital role in controlling eating. Food monitoring and control affect the obesity and the smart phone or web based such methods will be easier than hand written food log [47,48]. Earlier studies also shows keeping accurate food log is difficult even in web based systems [49]. In the current study we asked participants to write and maintain food log and reminded about that periodically in the class once in a week. More control on food log may give further weight reduction.
Current study confirms that the one and half hour IAYT is an effective alternative measure in this urban setting for different sectors of male obesity. The different sectors can be researched for the relative effectiveness and tailor made usability, in future.
Conclusion
The IAYT yoga training is effective in improving the anthropometric parameters of male obesity in urban setting. The weight, BMI, waist circumference and skinfold measurements were decreased. The psychological stress related to body weight difficulties and perceived stress was also reduced by practice of yoga for fourteen weeks. The findings suggest the usefulness of yoga for obesity treatment.
Trial Registration
The trial was registered with the Clinical Trials registry of India CTRI/2015/01/005433
a-Wilcoxon signed ranks test
b-based on positive ranks
c- based on negative ranks
*. Correlation is significant at the 0.05 level (1-tailed).
**. Correlation is significant at the 0.01 level (1-tailed).
WT: weight MACL: Mid arm circumference left
MACR: Mid arm circumference right
WC: Waist circumference
HC: Hip circumference
AF: Biceps skin fold thickness
RAB: Triceps skin fold thickness STOF: Suprailiac skin fold thickness
SHOB: Sub scapular skin fold thickness
BMI: body mass index WHR: Waist hip ratio
SKFT: Cumulative skin fold thickness
PFC: Percentage body fat
PSS: Perceived stress scale score
AAQW: Action and weight relayed difficulty score