Giant Cervical Osteophyte: An Unusual Cause of Dysphagia
Sudhir Kumar Srivastava1, Sunil Krishna Bhosale2, Tanvi Anoop Lohiya3, Rishi Anil Aggarwal4
1 Professor, and Head, Department of Orthopaedics, Seth GSMC and KEM Hospital, Parel, Mumbai, Maharashtra, India.
2 Assistant Professor, Department of Orthopaedics, Seth GSMC and KEM Hospital, Parel, Mumbai, Maharashtra, India.
3 Senior Registrar, Department of Ear, Nose and Throat, LTMMC and LTMGH, Sion, Mumbai, Maharashtra, India.
4 Senior Registrar, Department of Orthopaedics, Seth GSMC and KEM Hospital, Parel, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Tanvi Anoop Lohiya, Row House 4, Kanakia Spaces, Eternity, Teen Haath Naka Thane West - 400604, Maharashtra, India.
E-mail: tanvilohiya1987@gmail.com
Dysphagia due to skeletal causes is a rare entity. A large cervical osteophyte can cause mechanical compression of the pharyngo-oesophageal segment leading to dysphagia. Large cervical osteophytes can occur in cervical spondylosis, ankylosing spondylitis or Diffuse Idiopathic Skeletal Hyperostosis (DISH). A 60-year-old female came with progressive dysphagia due to a giant cervical osteophyte anterior to C4 and C5 vertebral bodies causing compression of the pharyngo-oesophageal segment. The patient was treated by surgical excision of the osteophyte by orthopaedic surgeons. The patient had complete relief of dysphagia following excision of the osteophyte.
Diffuse idiopathic skeletal hyperostosis, Pharyngo-oesophageal segment, Surgical excision
Case Report
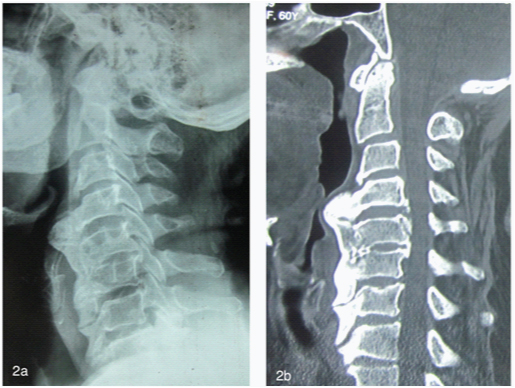
A 60-year-old female presented to the outpatient department with progressive dysphagia. Dysphagia to solids started 18 months back and gradually progressed to dysphagia to liquids 2 months prior to presentation. The patient had lost 7 kg over a period of 18 months. There was no history of odynophagia, breathlessness, noisy breathing or change in voice. Oesophagoscopy was performed, which revealed a well mucosalised mass on the posterior pharyngeal wall on the left side obstructing the pharynx [Table/Fig-1]. X ray showed a giant cervical osteophyte anterior to C4 and C5 vertebral bodies [Table/Fig-2a]. Computed tomography (CT) scan showed ossification of anterior longitudinal ligament from C4 to C7 [Table/Fig-2b]. Axial cuts revealed compression of the trachea with slight shift of trachea to the right [Table/Fig-3a]. The patient was referred to the orthopaedic department for further management.
An oesophagoscopy showing a predominantly left sided posterior pharyngeal wall mass, causing narrowing of the pharyngeal lumen.

(a) An X-ray showing giant cervical osteophyte anterior to C4 and C5 vertebral bodies along with feature suggestive of DISH. (b) CT scan showed ossification of anterior longitudinal ligament from C4 to C7.
(a) Axial cuts showing compression of the trachea with slight shift of trachea to the right. (b) Osteophyte exposed via anterior Smith-Robinson approach. Pharyngo-oesophageal segment is retracted medially after meticulous blunt dissection.
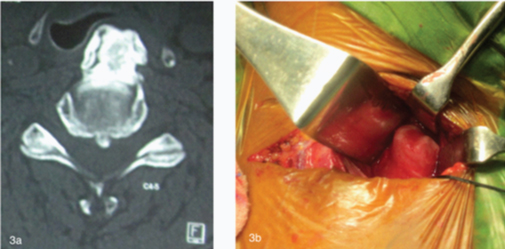
Patient was operated in supine position via anterior approach [Table/Fig-3b]. Complete excision of the osteophyte was done. No fixation was done as the disc space was kept intact and there was no instability. Patient was mobilized two days post-operative, following pain relief. At two-year follow-up, the patient was asymptomatic.
Discussion
Dysphagia due to skeletal causes is a rare entity. A large cervical osteophyte can cause mechanical compression of the pharyngo-oesophageal segment leading to dysphagia. Large cervical osteophytes can occur in cervical spondylosis, ankylosing spondylitis or Diffuse Idiopathic Skeletal Hyperostosis (DISH) [1]. Apart from pharyngo-oesophageal segment, cervical osteophytes can cause compression of vital structures like jugular foramen [2], sympathetic chain [3], vertebral artery [4] and trachea [5].
DISH is a condition characterized by calcification and ossification of soft tissues, mainly ligaments and enthesis. The classification criteria set by Resnick and Niwayama requires involvement of at least 4 contiguous vertebrae, preservation of the intervertebral disc space and absence of apophyseal joints or sacroiliac inflammatory changes. This case had ossification along anterior longitudinal ligament from C4 to T1 with preserved disc space and normal facet joint.
The prevalence increases with age and has been reported to be 2.8% and 2.6% in men and women aged ≥ 40 years, respectively [6]. DISH mainly involves the axial skeletal with thoracic involvement being the most common. Majority of the patients remain asymptomatic. In symptomatic patients, the most common complaints include pain and decreased range of motion. Neurologic symptoms may occur due to ossification of posterior longitudinal ligament or trivial trauma leading to fracture through the ossified ligaments [7].
The pharyngo-oesophageal segment lies in close proximity to the vertebral bodies. Cervical osteophytes can cause dysphagia due to mechanical compression of the pharynx/oesophagus or inflammation of para-oesophageal tissues [8]. Osteophyte at C3 or C3-4 disc level can cause abnormalities of tilt mechanism of epiglottis leading to dysphagia [9]. Even a small osteophyte at C6 level can lead to dysphagia, as this part of the oesophagus is narrow due to the presence of crico-pharngeal sphincter [10]. In our case, the cause was mechanical compression of oesophagus by large osteophyte anterior to C4 and C5 vertebral bodies, which was confirmed by an oesophagoscopy.
Excision of the osteophyte is the preferred choice of treatment. It may be done via anterior approach. However, one must be careful while excision of the osteophyte as the pharyngo-oesophageal segment may be adhered to the osteophyte and requires meticulous blunt dissection prior to excision otherwise, there may be oesophageal injury.
Conclusion
Giant cervical osteophyte due to DISH must be considered as one of the differential diagnosis of dysphagia. Surgical excision of the osteophyte via anterior approach is an effective method of treatment for such patients.
[1]. Angelos C, Dimitra A, Dysphagia due to anterior cervical osteophytes complicated with hypopharynx abscessBMJ Case Rep 2011 (2011) [Google Scholar]
[2]. Le AQ, Walcott BP, Redjal N, Coumans JV, Cervical osteophyte resulting in compression of the jugular foramen: Case reportJ Neurosurg Spine 2014 21(4):565-67. [Google Scholar]
[3]. Khurana KM, Hunter PJ, Horner’s syndrome produced by hypertrophic spurs from the cervical spineBr J Ophthalmol 1964 48:227-29. [Google Scholar]
[4]. Citow JS, Macdonald RL, Posterior decompression of the vertebral artery narrowed by cervical osteophyte: case reportSurg Neurol 1999 51(5):495-98. [Google Scholar]
[5]. Coutinho M, Freitas S, Malcata A, Tracheal stenosis by extrinsic compression: a case of anterior cervical hypertrophic osteophytosisActa Reumatol Port 2010 35(3):379-83. [Google Scholar]
[6]. Julkunen H, Heinonen OP, Knekt P, Maatela J, The epidemiology of hyperostosis of the spine together with its symptoms and related mortality in a general populationScand J Rheumatol 1975 4:23-27. [Google Scholar]
[7]. Sreedharan S, Li YH, Diffuse idiopathic skeletal hyperostosis with cervical spinal cord injury -a report of 3 cases and a literature reviewAnn Acad Med Singapore 2005 34(3):257-61. [Google Scholar]
[8]. Akhtar S, O’Flynn PE, Kelly A, Valentine PM, The management of dysphasia in skeletal hyperostosisJ Laryngol Otol 2000 114:154-57. [Google Scholar]
[9]. Suzuki K, Ishida Y, Ohmori K, Long term follow-up of diffuse idiopathic skeletal hyperostosis in the cervical spine: analysis of progression of ossificationNeuroradiology 1991 33:427-31. [Google Scholar]
[10]. Gupta M, Gupta M, Large osteophytes causing dysphagia: an interesting caseThe Internet Journal of Otorhinolaryngology 2009 11(2) [Google Scholar]