Unusual Presentation of Radial Nerve Entrapment with Lateral Humeral Condyle Fracture – A Case Report
Manoharan Muthulingam1, Swagat Mahapatra2
1 Assistant Professor, Department of Orthopaedics, Mahatma Gandhi Medical College and Research Institute, Pondicherry, India.
2 Assistant Professor, Department of Orthopaedics, Mahatma Gandhi Medical College and Research Institute, Pondicherry, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Swagat Mahapatra, Old MSR Quarters-21, JIPMER Campus, Pondicherry-605006, India.
E-mail: drswagat@gmail.com
Lateral humeral condyle fracture is the second most common fracture around the elbow in pediatric age group. Acute neurological deficit as a consequence of nerve injury associated with lateral humeral condyle fractures is very uncommon. We report a rare presentation of a case of lateral humeral condyle fracture in a 13-year-old boy with acute radial nerve palsy. Patient was operated through a modified anterolateral approach to the elbow with, exploration of the radial nerve and internal fixation of the fracture. Complete fracture union at 6 weeks with good range of movements and full neurological recovery at 12 weeks was seen.
We report this case due to rare combination of radial nerve injury and lateral humeral condyle fracture. Importance should be given to a thorough neurological examination during initial clinical examination and proper pre-operative planning.
Kirschner wires, Neurological deficit, Wrist drop
Case Report
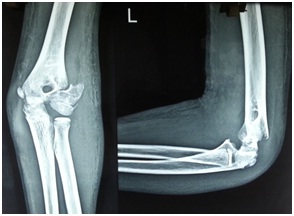
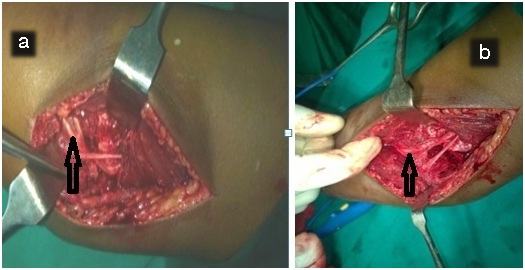
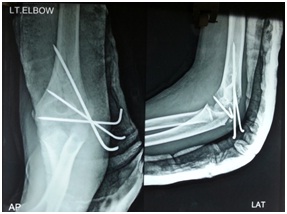
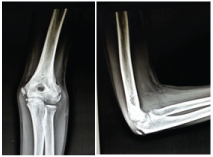
A 13-year-old boy presented to the Emergency department with acute onset pain and swelling around the left elbow joint following a fall on the outstretched hand. Immediately, following the fall, within 2 hours, the patient developed severe pain and swelling. After ruling out head, abdominal and chest and long bone fractures, detailed clinical examination of the elbow was undertaken. On examination, there were no open wounds. Swelling, tenderness and crepitus were observed around the lateral humeral condyle region and elbow movements were severely restricted. The injured elbow was unstable on doing a valgus stress test. On neurological examination, he was found to have wrist drop, thumb drop, finger drop and loss of sensation over the autonomous zone of the radial nerve. Distal pulse were well palpable. Median, and ulnar nerve examination was within normal limits. Clinically he was diagnosed as lateral humeral condyle fracture with radial nerve palsy. Radiographic examination confirmed our diagnosis as Milch type II lateral condyle fracture of the left humerus [Table/Fig-1]. After adequate pre-anaesthetic clearance, the patient was planned for surgery. The consent form was obtained from the patient parents after explaining them about the surgical procedure. Routinely lateral humeral condyle fractures are approached through a lateral approach to the elbow but in this case, a modified anterolateral approach to the elbow was adopted for better visualization and exploration of the radial nerve in the same sitting. Surgery was undertaken after adequate pre-anaesthetic clearance under regional block and tourniquet control. After the skin and subcutaneous incision, dissection was continued in the interval between the brachialis and brachioradialis muscles. On exploration, the radial nerve was found entrapped at the fracture site [Table/Fig-2]. It was carefully released and inspected under loupe magnification. The radial nerve was found to be minimally contused, but its continuity was maintained. After isolating and retracting the radial nerve medially fracture site was exposed completely, fracture hematoma evacuated and reduction was achieved under direct vision and was stabilized with three Kirschner wires (K-wire). One K-wire was passed through the epiphysis to fix the intra-articular fracture and two K-wires through the physis to hold the metaphyseal fragment [Table/Fig-3]. After confirming reduction and wire placement under image intensifier wound closure was done in layers. Post-operatively above elbow splint and dynamic cock up splint was given. Skin sutures were removed on 10th post-operative day. By six weeks, Kwires were removed, and mobilization was started but wrist drop was persistent [Table/Fig-4]. By three months, fracture had completely healed and the wrist drop had completely recovered [Table/Fig-5]. The patient had a good range of elbow movement (5-120 degree) [Table/Fig-6]. According to Mayo elbow score, our patient had an excellent outcome.
Pre-operative radiograph of left elbow anteroposterior and lateral view.
Intraoperative. (a) Entrapment of nerve. (b) Released from fracture site.
Immediate post-operative radiograph showing the reduction and K-wire fixation.
Clinical picture at six weeks showing persistence of wrist drop.

12 weeks post-operative radiograph showing complete fracture healing.
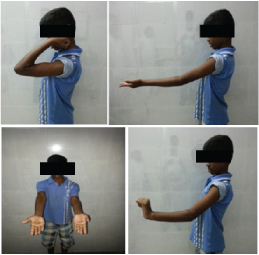
Clinical picture of the patient at 12 weeks showing range of movements and complete radial nerve recovery.
Discussion
Lateral condyle fracture is the second most common fracture around the elbow joint in the pediatric age group [1]. Lateral condyle fractures have the propensity to progress to non-union and due to epiphyseal growth arrest develop cubitus valgus deformity and consequently in later life Tardy Ulnar nerve palsy. Hence, it is termed as fracture of necessity and needs anatomical reduction and surgical fixation [1]. Acute nerve injuries are not described classically with lateral humeral condyle fractures. In current medical literature databases including Pubmed central only one acute radial nerve palsy with lateral humeral condyle fracture have been described till date and no acute median or ulnar nerve palsy have been reported. This result was obtained on searching the keywords lateral humeral condyle and acute nerve palsy. We report a similar case with the rare presentation of lateral humeral condyle fracture with acute radial nerve palsy. Radial nerve palsy is very common in shaft of humerus and more common in distal 1/3 fractures. As per common knowledge, any nerve palsy results from traction injury, contusion, laceration and entrapment at the fracture site. In our case, it was entrapped at the fracture site. As per recent medical literature only one case of radial nerve palsy with lateral humeral condyle fractures has been published till date by Tetsuya Nemoto et al., [2]. Our discussion mainly concentrates on studies involving the anatomical intricacies of the involved region and various rare cases involving the lateral humeral condyle. Gangadharan et al., reported radial nerve injury in a case of supracondylar fracture humerus during insertion of lateral k-wire [3]. A cadaveric study was conducted and showed that the proximal lateral K-wire should be placed posterolaterally within 2 cm from the lateral humeral epicondyle to avoid injury to the radial nerve [3]. In our case, the fracture was extending proximally beyond 2cm from the lateral epicondyle and may explain the radial nerve involvement. Carlan D et al., in their cadaveric study found that in the anterior compartment, the radial nerve has minimal mobility as it lies between the obliquely oriented lateral intermuscular septum and the lateral aspect of the humerus. On distal exploration, the nerve lies anterior to the humerus and is protected by brachialis muscle at the level of the proximal aspect of the lateral metaphyseal flare [4]. Abu-Jayyab Z et al., reported a case of fracture dislocation of the lateral humeral condyle and medial epicondyle of the humerus associated with complete radial nerve transection. They managed it with open reduction of fracture and radial nerve exploration and repair. Neurological function improved completely in six months [5]. Few reports have shown iatrogenic injuries to the radial and posterior interosseous nerves at the elbow. Smith and Joyce reported two patients with posterior interosseous nerve injury after open reductions of the lateral humeral condylar fragment, both of whom recovered spontaneously [6]. Another very rare case was reported by Friedman and Smith when the tip of a screw applied for a lateral humeral condyle fracture caused a delayed radial nerve injury 26 years after surgery [7].
Conclusion
Although, lateral humeral condyle fractures are very common in childhood but their association with acute neurological deficits is almost unheard. However, our case and few other rare cases published in medical literature throw light on this rare possibility. Hence, a very detailed neurological examination should be performed in every case so as not to miss these rare injuries. This case is the 2nd case of lateral condyle fracture with radial nerve palsy reported till date in medical literature.
[1]. Canale S. Terry, Beaty James H, Fractures and Dislocations in ChildhoodCampbell’s Textbook of Operative Orthopaedics 2013 12th editionElsevier Mosby:1393-94. [Google Scholar]
[2]. Nemoto T, Tajiri Y, Iijima J, A case of radial nerve paralysis associated with lateral humeral condyle fracture in a childJ Orthop Sci 2015 Nov 18 :piiS0949-2658(15)00091-93 [Google Scholar]
[3]. Gangadharan S, Rathinam B, Madhuri V, Radial nerve safety in Dorgan’s lateral cross-pinning of the supracondylar humeral fracture in children: a case report and cadaveric studyJournal of Pediatric Orthopaedics B 2014 23(6):579-83. [Google Scholar]
[4]. Carlan D, Pratt J, Patterson JM, Weiland AJ, Boyer MI, Gelberman RH, The radial nerve in the brachium: an anatomic study in human cadaversJ Hand Surg Am 2007 32(8):1177-82. [Google Scholar]
[5]. Abu-Jayyab Z, Abu-Zidan F, Marlovits S, Fracture dislocation of the lateral condyle and medial epicondyle of the humerus associated with complete radial nerve transactionJ Pak Med Assoc 2011 61(9):920-21. [Google Scholar]
[6]. Smith FM, Joyce JJ III, Fracture of lateral condyle of humerus in childrenAm J Surg 1954 87:324-29. [Google Scholar]
[7]. Friedman RJ, Smith RJ, Radial nerve laceration 26 years after screw fixation of a humeral fractureJ Bone Joint Surg Am 1984 66:959-60. [Google Scholar]