Why Should Viral Markers Be Mandatory in Ocular Surgeries: A Hospital Based Retrospective Study
Anita Ambastha1, Rakhi Kusumesh2, Gyan Bhasker3
1 Assistant Professor, Department of Ophthalmology, Regional Institute of Ophthalmology, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India.
2 Associate Professor, Department of Ophthalmology, Regional Institute of Ophthalmology, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India.
3 Additional Professor, Department of Ophthalmology, Regional Institute of Ophthalmology, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rakhi Kusumesh, Associate Professor, Department of Ophthalmology, Regional Institute of Ophthalmology, Indira Gandhi Institute of Medical Sciences, Patna, Bihar, India.
E-mail: drkrakhi@yahoo.com
Introduction
Hepatitis B Virus (HBV), Hepatitis C Virus (HCV) and Human Immunodeficiency Virus I, II (HIV-I,II) are serious global and public health problem. Knowledge of the seroprevalence would enable early diagnosis, treatment of patients and also help in prevention of horizontal spread of infection by application of universal infection control measures.
Aim
To determine the seroprevalence of HBV, HCV and HIV I, II infection in patients undergoing ocular surgery.
Materials and Methods
A retrospective review of 560 patients who had undergone ocular surgery between Dec 2014 to June 2015 at Regional Institute of Ophthalmology, Patna, India, was done. Blood samples of patients were tested for the presence of Hepatitis B Surface Antigen (HBsAg) and anti-HCV antibodies by Enzyme Linked Immunosorbent Assay (ELISA) method, while HIV I, II was tested by ELISA and Western Blot as per National AIDS Control Organization (NACO), India guidelines. The number of patients with positive viral serology, age, sex ratio and nature of surgery were analysed.
Results
Out of 560 patients, 27 (4.8%) patients were found to be positive for viral serology. HBsAg was positive in 22 patients (3.92%). Out of these 14 patients (2.5%) were male while 8(1.4%) were females. Anti- HCV was positive in 3 (0.53%) patients. Out of these 2(.35%) were male and 1 (.17%) was female. HIV was positive in 2 patients (0.35%), both of whom were males.
Conclusion
Keeping in view the number of cases of seropositivity in our study and various studies showing the presence of these viruses in aqueous and tears, we suggest that screening for viral markers should be made mandatory before ocular surgery so that early detection and treatment of patients can be done and risk of horizontal spread is minimized.
Elective ocular surgeries, Horizontal spread, Screening
Introduction
According to a 2015 survey, the government of India estimates that the national adult prevalence of HIV is 0.26% [1]. For HBV, the Indian subcontinent is classified as an intermediate endemic zone and has the second largest global pool of chronic HBV infection burden with a prevalence of 3-4.2% [2,3]. The HBV infection leads to chronic carrier state in 60% of affected individuals [2,3]. HCV has a low to moderate (1–1.5%) prevalence in India but India accounts for a significant share of global HCV infections due to the large population [4].
HBV, HCV and HIV are bloodborne viruses transmitted primarily through direct contact with the blood of an infected person [5,6]. Some of these seropositive patients with ophthalmic problems could present risk of transmission to treating opthalmologists and caregivers [7].
Various factors like Operation Theatre (OT) procedures, cleaning and handling of sharp instruments during surgery and anaesthesia puts the health care workers at risk of exposure to these bloodborne infections [7]. In our scenario, screening of viral serology is not routinely done in patients who undergo ocular surgeries, bulk of which is made up of cataract surgery. Since, majority of carriers are asymptomatic [8–10], they pose a real threat by horizontal spread to health staff, surgeons and other patients. To the best of our knowledge, only a few Indian studies on screening of blood borne viral infections among patients for ocular surgery are available. Hence, we undertook this study to determine the prevalence of positive viral serology among patients who underwent ocular surgery.
Materials and Methods
We reviewed medical records of 560 patients who underwent ocular surgeries between Dec 2014 to June 2015 at Regional Institute of Ophthalmology, Patna for presence of positive viral serology for HIV I, II, HBV and HCV. Ethics approval was obtained. Symptomatic patients with history of jaundice and immunization were excluded. Of 560 patients, there were 312 male and 248 female patients. Mean age was 49.62 ± 19.91 years (range 0 .75–87 years). HBV was tested with ELISA test kit (Span Diagnostics) which is based on direct ELISA (Sandwich) technique. HCV was tested with ELISA Kit (Bio standard diagnostic pvt, Ltd) . It is an indirect sandwich ELISA test. For HIV, a serum sample was considered negative, if 1st ELISA report (immunodot test kit of SPAN, ARKRAY Healthcare Pvt Ltd) was so. If reactive, it was subjected to a second ELISA test (Enzaids HIV I, II Elisa test kit of SPAN, ARKRAY Healthcare Pvt Ltd) which utilized the principle of Heterogenous indirect antibody detection. It is reported reactive only if second test confirms the positive report of first. Discordant result of ELISA was tested with Western Blot. This is in accordance with NACO guidelines [11]. The confidentiality about the study patient’s name and their results were maintained. All seropositive cases were grouped as high risk cases for OT, operated with extra protocol and universal infection control measures were taken.
The statistical analysis was performed using the statistical package ‘R’3.2.4 Revised (2016-03-16 r70336) and the Confidence Intervals (CI) for viral serology (overall), HBV & HCV and HIV at 95% confidence level was calculated.
Results
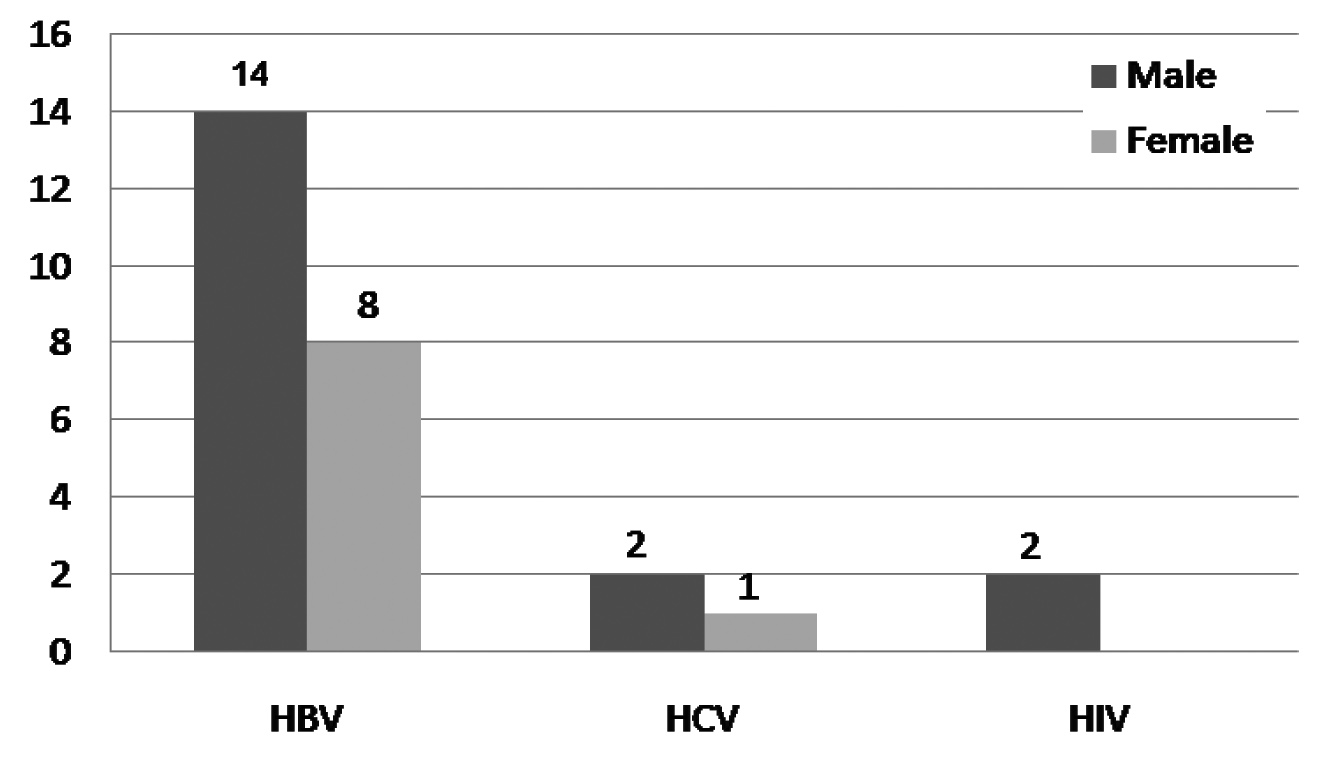
Out of 560 patients, 27 patients (4.8%) {95% CI (.0.0301 - 0.0657)} were found to be positive for viral serology. HbsAg was positive in 22 patients (3.92%) {95% CI, (0.023- 0.055)}. Anti HCV antibody was positive in 3 patients (0.53%) {95% CI, (0.0007 and 0.0113)}. HIV was positive in 2 patients (0.35%) {95% CI, (−0.0014 and 0.0084)}, both of whom were males [Table/Fig-1].
Frequency of positive serology in male and female patients.
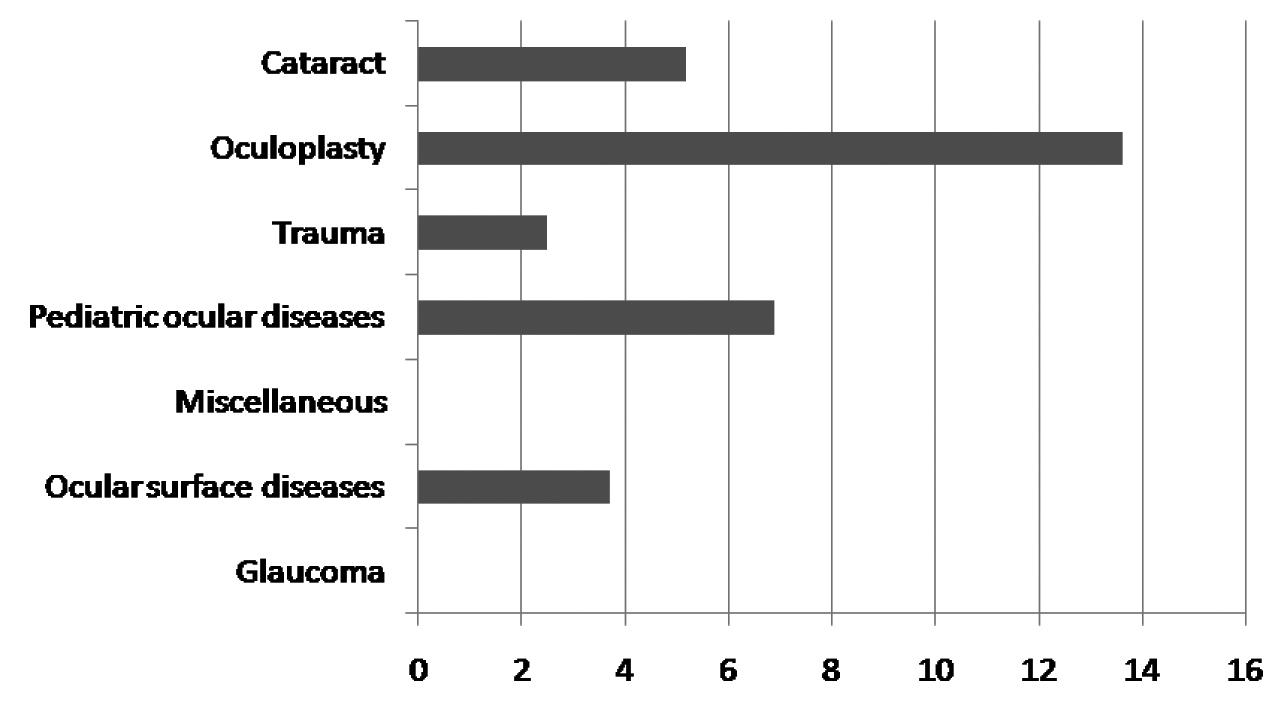
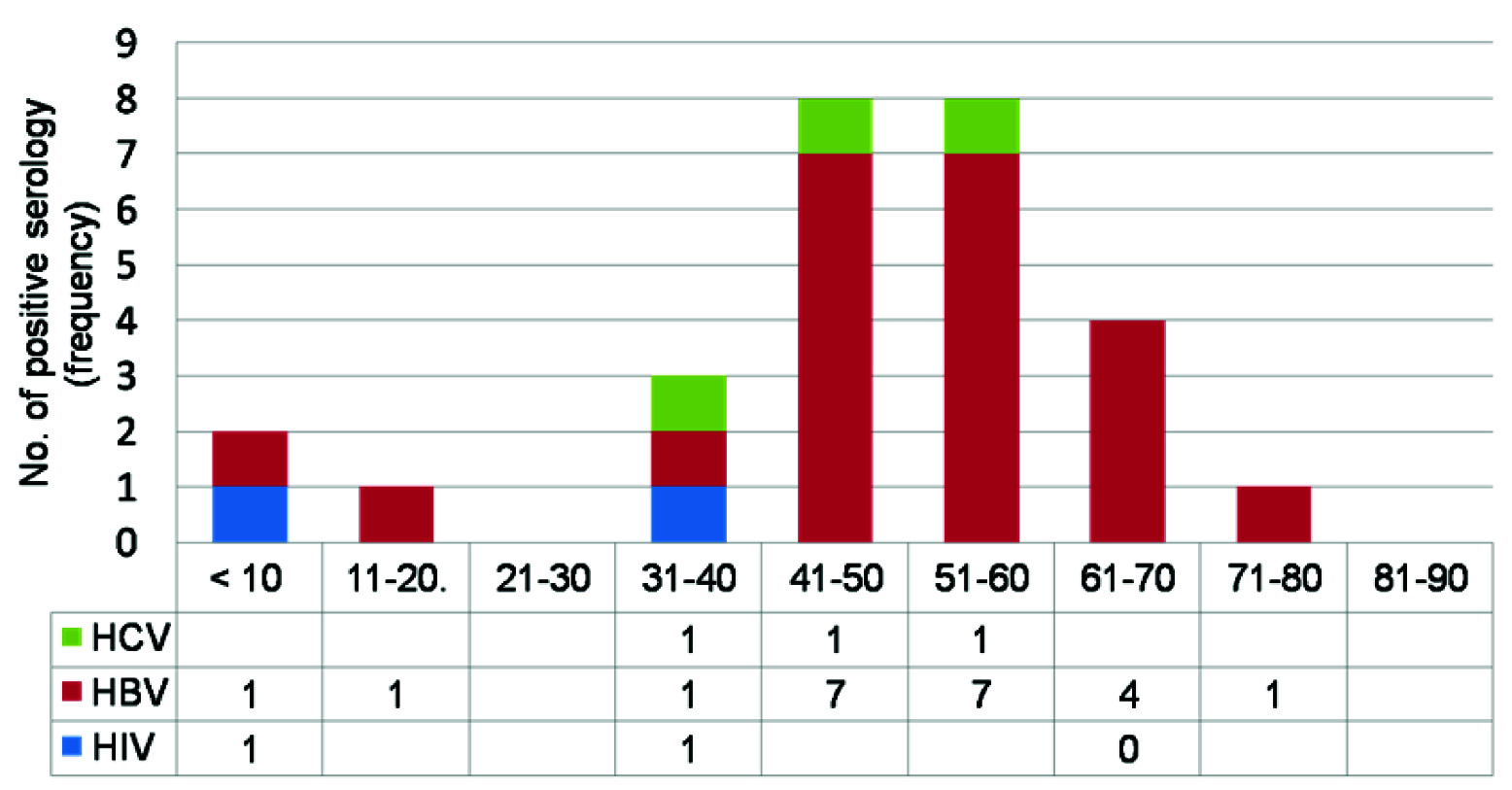
Oculoplasty was the most common surgery in which overall seropositivity of HIV, HBV and HCV was seen [Table/Fig-2]. HCV seropositivity was seen in one case each of cataract, trauma and oculoplasty surgery [Table/Fig-3]. Out of 22 HBsAg positive patients, 19 (86.6%) were between 40-70 years of age group. Two anti-HCV positive patients were between 40-60 years (66.6%). HIV was positive in one child less than 10 years (50%) and one person between 30-40 years (50%) [Table/Fig-4].
Percentage of seropositivity (HIV, HBV, HCV) in various ocular surgeries.
Frequency of positive serology in different indications of ocular surgeries.
| Indications of surgery | No. of cases | HIV | HBV | HCV |
|---|
| Cataract | 348 | 1 | 17 | 1 |
| Glaucoma | 41 | 0 | 0 | 0 |
| Trauma | 80 | 0 | 1 | 1 |
| Oculoplasty | 22 | 0 | 2 (DCR)* | 1(DCR)* |
| Ocular surface diseases | 27 | 0 | 1(OSSN)† | 0 |
| Miscellaneous | 13 | 0 | 0 | 0 |
| Pediatric ocular diseases | 29 | 1 (Cataract surgery) | 1(Cataract Surgery) | 0 |
* Dacryocystorhinostomy, † ocular surface squamous neoplasia.
Frequency of positive viral serology in different age groups.
Discussion
India is facing a huge burden of HIV, HBV and HCV infection [12–14]. Asymptomatic carriers with positive viral serology serve as reservoirs of infection within the community and the lack of routine screening prior to surgery may be one of the factors responsible for increased disease transmission [10,15,16]. Ophthalmologists are exposed to infectious disease via contact with tears and aqueous humor and by accidental needle pricks during surgery [7,17]. Although pubmed/ google search, did not show any case report published on disease transmission via tears and aqueous but several studies have reported the detection of these viral antigens in tears and aqueous of infected patients. Temel et al., and Koksal et al., noted that 70% and 85% HBsAg-seropositive patients also tested positive for HBsAg in tear and aqueous humor samples by Polymerase Chain Reaction (PCR) respectively [18,19]. Ching-Yao Tsai reported the case of an asymptomatic Taiwanese HBV patient in whom HBV was detected in aqueous humor using PCR [17]. Kobayakawa et al., reported that 50% of anti-HCV antibody positive patients also tested positive for HCV in aqueous humor as determined by PCR [20]. HIV viruses too have been isolated in tears, cornea, aqueous humor, conjunctiva, retinal vascular endothelium. Yang Han M et al., detected presence of HIV-1 viruses in tears of patients even under long-term Highly Active Anti-Retroviral Therapy [HAART] treatment [21].
In our study, the results show the rate of HBV infection is higher than HCV in this study, which is in line with other studies [22–24]. Sayeedul hasan arif et al., noted a prevalence of 4.47% (HBsAg) and 1.73% (anti-HCV) in hospitalized surgical patients [23]. The prevalence of HIV seroprevalence in our study was 0.35% which is close to other studies [24–26]. The seropositivity in patients was maximum among those who underwent oculoplasty surgery mostly dacrocystorhinostomy (13.64%). This could be because routine serological tests are mostly done in extraocular surgeries and if reactive they are referred to our regional instititute for management.
The prevalence of HBV and HCV infection in our study was found to be more in age group 40-70 and 40-60 years respectively. It could be due to most patients in present study being operated for senile cataract (62.1%). The highest number of positive cases of HBV and HCV in a study by Iftikhar et al., and Naeem et al., were reported in age group 50-85 and 55- 64 years respectively amongst cataract patients [22,27]. In our study, 2 patients were HIV-1 positive, out of which one patient was less than 10 years while another was between 40-50 years. In a previous study children (<1 yrs) accounted for 6.5% of all infections, while 88.7% were in age group 15-49 years [28].
In our study, male & female genders have no effect on viral serology diseases at 5% significance level. However, the greater frequency of HBV and HCV infection in males (2.5%, 0.35%, respectively) as compared to females (1.4%, 0 .17%, respectively) could be a reflection of more males coming for treatment and testing in our setting. Few authors have suggested that it could be due to more social mobility in males than females and thus greater vulnerability to be infected [29,30]. This finding is comparable to a study by Sayeedul hasan arif et al., who noted the seroprevalence of HBVand HCV to be significantly higher among males (6.4%, 2.7%, respectively) than females (4.9%, 1.9%, respectively) among hospitilized indoor patients [23].
Transmission of HBV, HCV and HIV to healthcare workers and other patients through horizontal spread at hospital is a matter of great concern. As per our knowledge, inadequate serological screening prior to ocular surgeries may be one of the factors reponsible for increased disease transmission.
Limitation
In this study, aqueous and tears were not screened for the presence of viral markers which should be considered as major limiation and it can be incorporated in future studies. Another limitation would be lack of screening for patients in window period which would have led to more patients being detected as seropositive.
Conclusion
Keeping in view the number of cases of seropositivity in our study and various studies showing the presence of these viruses in aqueous and tears, we suggest that screening for viral markers should be made mandatory and part of routine protocol before ocular surgery so that early detection and treatment of patients can be done and risk of spread is minimized.
* Dacryocystorhinostomy, † ocular surface squamous neoplasia.
[1]. India HIV estimates 2015 technical report, National AIDS Control Organization and National institute of medical statistics, Indian council of medical research, Ministry of Health & Family Welfare, Government of India [Google Scholar]
[2]. Global HIV/AIDS response, Epidemic update and health sector progress towards universal access. Hepatitis B Fact sheet 2015 WHO/UNICEF/UNAIDS (2011) [Google Scholar]
[3]. Acharya SK, Madan K, Datta Gupta S, Panda SK, Viral hepatitis in IndiaThe National Medical Journal of India, Special Series: Communicable Diseases 2006 2019 [Google Scholar]
[4]. Dhiman RK, Future of therapy for Hepatitis C in India: A matter of accessibility and affordability?Clin Exp Hepatol 2014 4(2):85-86. [Google Scholar]
[5]. Centre of Disease Control and Prevention. [HIV and Viral Hepatitis] (fact sheet). www.cdc.gov/hepatitis/populations/hiv.htm [Google Scholar]
[6]. Khatomy A, Prevalence and reporting of needle stick injuries: A survey of surgery team members in Kermanshah University of Medical Sciences in 2012Glob J Health Sci 2015 8(3):245-51. [Google Scholar]
[7]. Collins CH, Kennedy DA, Microbiological hazards of occupational needlestick and ‘sharps’ injuriesJ Appl Bacteriol 1987 62:385-402. [Google Scholar]
[8]. Raimondo G, Pollicino T, Cacciola I, Squadrito G, Occult hepatitis B virus infectionJ Hepatol 2007 46:160-70. [Google Scholar]
[9]. Rezaee-Zavareh MS, Hadi R, Karimi-Sari H, Occult HCV Infection: The current state of knowledgeIranian Red Crescent Medical Journal 2015 17(11):e34181 [Google Scholar]
[10]. Sahu GK, McNearney T, Evans A, Turner A, Weaver S, Transient or occult HIV infections may occur more frequently than progressive infections: changing the paradigm about HIV persistenceArch Virol Suppl 2005 (19):131-45. [Google Scholar]
[11]. Guidelines for HIV Testing. National AIDS Control Organization 2008:49-50 [Google Scholar]
[12]. National AIDS Control Organization. Ministry of Health and Family Welfare, Government of India. Available from: http://www.nacoonline.org/National_AIDS_Control_Program/ [Last accessed on 2012 Nov 28] [Google Scholar]
[13]. Batham A, Narula D, Toteja T, Sreenivas V, Puliyel JM, Systematic review and meta-analysis of prevalence of hepatitis B in IndiaIndian Pediatr 2007 44:663-74. [Google Scholar]
[14]. Overview of Hepatitis C Problem in Countries of the South-East Asia Region. Available from: http://www.searo.who.int/en/Section10/Section17/Section58/Section220_217.htm [Last accessed on 2012 Nov 28] [Google Scholar]
[15]. Raimondo G, Pollicino T, Cacciola I, Squadrito G, Occult hepatitis B virus infectionJ Hepatol 2007 46:160-70. [Google Scholar]
[16]. Recommendations for prevention and control of Hepatitis C virus(HCV) infection and HCV- related chronic disease. October 16, 1988/47(RR19);1-39. mmwrq@cdc.gov [Google Scholar]
[17]. Ching-Yao Tsai, Chih-LinLin Detection of Hepatitis B Virus in the Aqueous Humor of a Hepatitis B Virus CarrierOpthalmologica 2009 223:93-95. [Google Scholar]
[18]. Temel A, Seber E, Gunay M, Detection of hepatitis B surface antigen in aqueous humorActa Ophthalmol (Copenh) 1990 68:205-08. [Google Scholar]
[19]. Koksal I, Cetinkaya K, Aker F, Hepatitis B surface antigen in tears and aqueous humor: a comparative study of serum hepatitis B surface antigen levelsOphthalmologica 1992 204:19-22. [Google Scholar]
[20]. Kobayakawa S, Tochikubo T, Watanabe H, Nomura N, Hepatitis C in the aqueous humorNihon Ganka Gakkai Zasshi 1993 97:1061-64. [Google Scholar]
[21]. Han Y, Wu N, Zhu W, Li Y, Zuo L, Ye J, Detection of HIV-1 viruses in tears of patients even under long-term HAARTAIDS 2011 25(15):1925-27. [Google Scholar]
[22]. Ahmad I, Khan BS, Rehman UH, Khan HM, Anwar S, Frequency of hepatitis b and hepatitis c among cataract patientsGomal Journal of Medical Sciences 2006 4:61-64. [Google Scholar]
[23]. Arif SH, Afrose R, Khan AI, Akram M, Singh SK, Seropositivity Rates for Hepatitis B and C viruses in indoor patients of a tertiary care centre of northern IndiaInternational Journal of Current Microbiology and Applied Sciences 2015 1:243-47. [Google Scholar]
[24]. Sood S, Malvankar S, Seroprevalence of hepatitis B surface antigen, antibodies to the hepatitis C virus, and human immunodeficiency virus in a hospital-based population in Jaipur, RajasthanIndian J Community Med 2010 35:165-99. [Google Scholar]
[25]. Mahalakshmi B, Madhavan HN, Pushpalatha R, Margarita S, Seroprevalence of human immunodeficiency virus, hepatitis B virus and hepatitis C virus among eye donorsIndian J Opthalmol 2004 52(1):6162 [Google Scholar]
[26]. NACO. Annual Report 2013-14:6 [Google Scholar]
[27]. Naeem SS, Siddiqui EU, Kazi AN, Khan S, Abdullah FE, Adhi I, Prevalence of Hepatitis ‘B’ and Hepatitis ‘C’ among preoperative cataract patients in KarachiBMC Research Notes 2012 5:492 [Google Scholar]
[28]. India HIV estimates 2015 technical report, National AIDS Control Organization and National institute of medical statistics, Indian council of medical research, Ministry of Health & Family Welfare, Government of India [Google Scholar]
[29]. Khan AJ, Siddiqui TR, Prevalence and Importance of hepatitis B and C screening in cases undergoing elective eye surgeryPak J Ophthalmol 2007 23:39-44. [Google Scholar]
[30]. Khokar N, Gill ML, Malik GJ, General seroprevalence of hepatitis C and Hepatitis B virus infection in populationJ Coll Phys Surg Pak 2004 14:534-36. [Google Scholar]