Analysis of Fetal Palate to Assist Pre-natal Ultrasound
Anjali Shastry1, Yogitha Ravindranath2, Roopa Ravindranath3
1 Lecturer, Department of Anatomy, St Johns Medical College, Bangalore, Karnataka, India.
2 Associate Professor, Department of Anatomy, St Johns Medical College, Bangalore, Karnataka, India.
3 Professor, Department of Anatomy, St Johns Medical College, Bangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Anjali Shastry, Lecturer, Department of Anatomy, St John’s Medical College, Bangalore, Karnataka, India.
E-mail: anju_shas@yahoo.com
Introduction
Cleft palate is one of the major facial congenital malformation in newborns. Pre-natal detection of this malformation is limited to detection of clefting of hard palate but isolated soft palate clefting still remains challenge for sonologists. As Indian literature is limited present study was attempted to provide dimensions and position of fetal palate by digitized images.
Aim
To study dimensions, position and differences in parameters between second and third trimester fetuses.
Materials and Methods
Median sagittal section of 32 formalin fixed fetuses was selected from the Department of Anatomy, St John’s Medical College, Bangalore, Karnataka, India. Anatomical landmarks-The Nasion (N), Sellaturcica (S), Anterior Nasal Spine (ANS), Posterior Nasal Spine (PNS), tip of Uvula (U) were marked on sections. Length of hard palate (from ANS to PNS), Length of soft palate (from PNS to U), Hard palate/soft palate angle was defined. The anterior position of soft palate and its posterior position in relation to anterior cranial base were marked as N-S-PNS and N-S-U angle, respectively. The measurements were acquired directly from the digitized images using ImageJ software. Statistical analysis was done using SPSS 16.
Results
The mean values of ANS-PNS and PNS-U were 23.59±3.69mm and 14.39±2.70mm, respectively. The mean values of hard palate/soft palate angle, N-S-PNS and N-S-U angle were 144.720±11.11,51.150±9.09 and 93.370±9.58, respectively. Significant difference was noted between trimesters for length of hard and soft palate but not for palatal angles.
Conclusion
During Pre-natal assessment of cleft palate, it is important for sonologist to keep in mind that the dimensions of palate proportionately increased in last two trimesters while the position remains constant.
Cleft palate, Facial growth, Fetal development, Pre-natal diagnosis, Soft palate, Ultrasonography
Introduction
The palate forms the roof of the mouth. It is divisible into two regions, namely the hard palate in front and soft palate behind [1]. The primary palate includes the lips and jaw, nasal bone and secondary palate consists of hard palate, which runs behind and horizontally of the incisive foramen and soft palate or velum, which curves downwards and backwards from the posterior part of the hard palate and ends in the uvula [2]. Usually the clefting of the secondary palate is always in midline and results from failure of the palatine processes to elevate and grow [2]. Even with an isolated cleft lip there is an increased risk of chromosomal abnormality and over 250 syndromes are associated with clefting which necessitates appropriate genetic, surgical and psychological counseling [3–5]. The role of Pre-natal education and support is extremely important in the preparation of prospective parents. Only 0% to 22% of cases are being detected Pre-natally [5–7]. Visualization of soft palate is difficult. Angled insonation and 3D-ultrasound visualization helps to get better picture of fetal palate. The obstruction of viewing the palate is more caused by maxillary shadow which makes it necessary to study the morphometry of palate. The development of an ultrasound technique to view the fetal soft palate might have been impeded by sonographers’ lack of knowledge of the appearance of the fetal soft palate on 3D ultrasound examination [8]. With invention of in-utero surgeries, repair of cleft lip and palate has led to scarless repair since there is tremendous healing power in fetus. Information regarding dimensions and repair of cleft palate will help in these surgeries and reduce postnatal reconstruction which might result in scarring.
Considering above facts present study has been done to aid Pre-natal ultrasound visualization in fetuses of different periods of gestation.
Aim
To study morphometry, position of fetal palate and difference in these parameters between last two trimesters of pregnancy.
Materials and Methods
A cross-sectional observational study was done on median sagittal section of 32 formalin fixed fetuses (16-2nd trimester,16-3rd trimester) for 3 months from the collection of Department of Anatomy, St John’s Medical College, Bangalore over period of 10 years. Consent of the voluntary parental donors and the institutional ethical review committee was obtained prior to foetal study as per the norms of the Institute. These fetuses were donated following spontaneous abortion/delivered following intrauterine death/still birth reason of which is not known. Fetuses with congenital malformation and deformities were excluded. Sample size was calculated using mean and standard deviation from literature done by Captier G et al., using N master software [9].
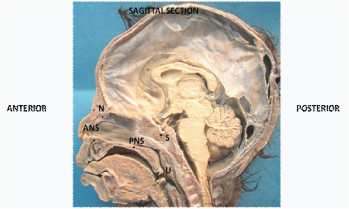
Anatomical landmarks-The Nasion (N), Sellaturcica (S), Anterior Nasal Spine (ANS), Posterior Nasal Spine (PNS), tip of Uvula (U) were marked on sections [Table/Fig-1].
Length of hard palate (from ANS to PNS), Length of soft palate (from PNS to U), Hard palate/soft palate angle was defined [Table/Fig-2].
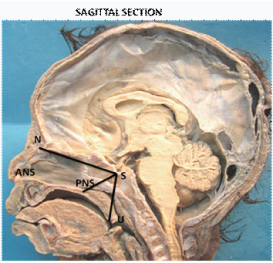
The anterior position of soft palate and its posterior position in relation to anterior cranial base were marked as N-S-PNS and N-S-U angle respectively [Table/Fig-3].
Digital photographs of sagittal section of all 32 formalin fixed fetuses were taken. To best of our knowledge this is a novel method of using digital photograph and ImageJ analyser. The sections were placed on osteometric board in such a way that its sagittal section was pointing upwards. A digital camera was fixed to stand of osteometric board for proper focus and centered along with sections on the board. A scale was placed near sections to convert it into pixels to obtain measurements.
The measurements were acquired directly from the digitized images using ImageJ software. ImageJ is a Java based application for analysing images. ImageJ runs either as an online applet or as a downloadable application which you’ll find here. ImageJ can display, edit, analyse, process, save and print 8-bit, 16-bit and 32-bit images and supports most major formats including TIFF, GIF, JPEG, BMP, DICOM, FITS and "raw". The main use of ImageJ is that it can calculate area and pixel values which may be useful for graphic designers. It does, however, go a little beyond that too, allowing you to measure distances and angles, create density histograms and also line profile plots. A single user can operate this software.
Anatomical landmarks defined on sagittal sections.
Measurement of hard palate (ANS-PNS), Soft palate (PNS-U), Hard palate/soft palate angle.

Measurement of N-S-PNS and N-S-U angle.
Statistical Analysis
Statistical analysis was done using SPSS version 16. Differences in trimesters were estimated using Independent sample t-test (p-value <0.05 considered significant).
Results
As seen in [Table/Fig-4] significant difference was noted between trimesters for length of hard and soft palate (p<0.05). There was no significant difference between last two trimestersin hard palate/soft palate angle, as well as N-S-PNS and N-S-U angle.
Mean, SD, p-value of the measured parameters of 2nd and 3rd trimester fetuses.
| Parameters | 2nd trimester | 3rd trimester | p-value |
|---|
| Mean ±SD | Mean ±SD |
|---|
| Hard palate length (mm) | 21.36±2.99 | 25.83±2.92 | .000 |
| Soft palate length(mm) | 13.02±2.32 | 15.71±2.43 | .003 |
| Hard palate/soft palate angle | 143.37°±11.21 | 146.07°±11.58 | 0.52 |
| N-S-PNS | 50.89°±8.74 | 51.42°±9.67 | 0.87 |
| N-S-U | 96.29°±6.27 | 90.45°±11.52 | 0.86 |
Discussion
In present study, done on formalin fixed fetuses dimensions of hard as well as soft palate proportionately increased in last two trimesters of pregnancy. This shows that there is rapid growth in measurements of both hard and soft palate with growth of facial skeleton. But position of soft palate with respect to hard palate (hard palate/soft palate angle) and anterior cranial base (N-S-U & N-S-PNS) remained same.
In a cadaveric study done by Captier G et al., on French population by digital images there is disparity in dimensions of palate as seen in [Table/Fig-5] [9,10]. Possible variation in values may be due to change in ethnicity or environmental factors. Hosapatna et al., studied sagittal sections of 24 formalin fixed Indian dead fetuses of second and third trimester by direct caliper method where hard palate length was higher and soft palate length was lower when compared with our study [Table/Fig-5] [9,10]. The change in dimensions may be due to adoption of different methodology. In study done by Captier G et al., and Hosapatna et al., there was significant difference in hard palate and soft palate length between second and third trimester fetuses. This is in correlation with present study, which indicates there is rapid growth in palatal length in last two trimesters of gestation [Table/Fig-5] [9,10].
Comparison of measurements of hard and soft palate with previous studies [9,10].
| Author /year/population/n* | Type of study | Hard palate length (mm) | Soft palate length (mm) |
|---|
| 2nd trimester | 3rd trimester | 2nd trimester | 3rd trimester |
|---|
| Captier G et al., 2008/ France n=18 [9] | Cadaver | 16.52 ± 0.34 | 27.44 ± 0.34 | 8.74 ± 0.15 | 15.83 ± 0.3 |
| Hosapatna et al.,2013 India /n=24 [10] | Cadaver | 29.7 ± 2 | 35.6± 3.7 | 12.5 ± 2.6 | 14 ± 2.3 |
| Present study 2016 India /n=32 | Cadaver | 21.36± 2.99 | 25.83± 2.92 | 13.02± 2.32 | 15.71± 2.43 |
* n is sample size
Captier et al., studied the anterior position of soft palate and its posterior position in relation to anterior cranial base which is in correlation with our study which reveals that position of soft palate with respect to cranial base does not alter with increase in period of gestation [Table/Fig-6] [9]. Hence, it can be taken as landmark for better visualization of anatomy and position of soft palate throughout the pregnancy.
Comparison N-S-PNS and N-S-U angle with previous studies [9].
| Author / year/ population /n* | Type of study | Hard palate length (mm) | Soft palate length (mm) |
|---|
| 2nd trimester | 3rd trimester | 2nd trimester | 3rd trimester |
|---|
| Captier G et al.,/ 2008/France/ n=18 [9] | Cadaver | 48.8°± 3.13 | 52.26°± 3.31 | 89.66°± 5.51 | 92.97°± 4.01 |
| Present study/2016 India /n=32 | Cadaver | 50.89°± 8.74 | 51.42°± 9.67 | 96.29°± 6.27 | 90.45°± 11.52 |
* n is sample size.
According to Captier et al., the hard palate/soft palate angle was found to be 150.33°±7.62, 150.20°±6.67 in second and third trimesters, respectively. A 3D ultrasound study done by Faure et al., (2007) calculated the velopalatal or Hard palate/soft palate angle at GA of 20 - 25 weeks which was 150° ± 7 [11]. In study done by Hosapatna et al., the angle was 141.75° ± 13.16, and 140.88° ± 11.72 in second and third trimester respectively which is in correlation with our study [Table/Fig-7] [9–11] indicating there was no significant change in angle with respect to gestational age.
Comparison of hard palate/soft palate angle with previous studies [9–11].
| Author / year/ population /n* | Type of study | Hard palate length (mm) |
|---|
| 2nd trimester | 3rd trimester |
|---|
| Captier G et al., 2008 Francen= 18 [9] | Cadaver | 150.33°± 7.62 | 150.20°±6.67 |
| Faure J.M. et al., 2008 France n= 15 [11] | Ultrasound | 150°±7 |
| Hosapatna et al., 2013 India /n=24 [10] | Cadaver | 141.75° ± 13.16 | 140.88° ± 11.72 |
| Present study /2016 /India (n=32) | Cadaver | 143.37°±11.21 | 146.07°±11.58 |
* n is sample size.
To best of our knowledge very few studies has been done on palate of cadaveric fetuses in Indian literature. With advent of in-utero and plastic surgeries more information regarding normal anatomy and embryology of fetal palate is necessary for surgeons to ensure scarless repair of cleft lip and palate.
Hence, present study can aid in prompt diagnosis of isolated cleft lip and palate which further helps to rule out syndromic association as well as screening of other congenital anomalies.
Conclusion
In last two trimester, fetuses position of palate remained constant but dimensions of palate proportionately increased. This should be considered during Pre-natal diagnosis of cleft palate as well as early intervention during fetal or postnatal period to prevent postnatal complications.
* n is sample size
* n is sample size.
* n is sample size.
[1]. Standring S, Ellis H, Healy JC, Williams A, Gray’s Anatomy 2008 40th editionElsevier Churchill Livingstone:502 [Google Scholar]
[2]. Campbell S, Pre-natal ultrasound examination of the secondary palateUltrasound Obstet Gynecol 2007 29(2):124-27. [Google Scholar]
[3]. Bianchi DW, Crombleholme TM, D’Alton ME, Cleft lip and cleft palateIn Fetology: diagnosis and management of the fetal patient, Bianchi DW, Crombleholme TM, D’Alton ME (eds) 2000 New YorkMcGraw-Hill:199-207. [Google Scholar]
[4]. Faure JM, Captier G, Bäumler M, Boulot P, Sonographic assessment of normal fetal palate using three-dimensional imaging: a new techniqueUltrasound Obstet Gynecol 2007 29(2):159-65. [Google Scholar]
[5]. Calzolari E, Pierini A, Astolfi G, Bianchi F, Neville AJ, Rivieri F, Associated anomalies in multi-malformed infants with cleft lip and palate: An epidemiologic study of nearly 6 million births in 23 EUROCAT registriesAm J Med Genet 2007 143(6):528-37. [Google Scholar]
[6]. Clementi M, Tenconi R, Bianchi F, Stoll C, Evaluation of Pre-natal diagnosis of cleft lip with or without cleft palate and cleft palate by ultrasound: experience from 20 European registries. EUROSCAN study groupPrenat Diagn 2000 20:870-75. [Google Scholar]
[7]. Cash C, Set P, Coleman N, The accuracy of antenatal ultrasound in the detection of facial clefts in a low-risk screening populationUltrasound Obstet Gynecol 2001 18:432-36. [Google Scholar]
[8]. Sohan K, Freer M, Mercer N, Soothill P, Kyle P, Pre-natal detection of facial cleftsFetal Diagn Ther 2001 16:196-99. [Google Scholar]
[9]. Captier G, Faure JM, Baumler M, Anatomy and Growth of the Fetal Soft Palate: A Cadaveric Study to Improve Its Ultrasonographic ObservationCleft Palate– Craniofacial Journal 2008 45(4):439-45. [Google Scholar]
[10]. Hosapatna M, Ankolekar VH, D’Souza A, A study on fetal palatal growth with respect to different anatomical landmarks and its clinical relevance: A cadaveric studyInt J Health Sci Res 2013 3(11):51-5. [Google Scholar]
[11]. Faure JM, Baumler M, Bigorre M, Pre-natal diagnosis of an isolated incomplete V-shaped cleft palate using a new three-dimensional ultrasound technique investigationSurg Radiol Anat 2007 29:695-98. [Google Scholar]