Scabies, known as the seven-year itch, is a contagious skin infestation by the mite Sarcoptes scabiei. In most of the rural communities of the developing world, the ectoparasitosis is endemic, where prevalence is up to 10% in the general population more so in children [1,2]. It affects both males and females of all socioeconomic status and race. Crowded living conditions such as those found in child care facilities, group homes and prisons increase the risk of spread [2].
As it is not possible to eliminate scabies, morbidity control is the only option to reduce the disease burden [3]. Morbidity is not only reflected by the degree of clinical pathology but also includes the emotional aspects of a skin disease. Both types of morbidity may reduce the quality of life. Over the past few years, there has been an increasing interest in assessing the quality of life of patients with skin diseases as well as in the development of methods of assessment [4]. Patients with skin diseases may have their lives affected in many ways. This was demonstrated in a study where majority of the patients reported itching and discomfort along with sleep disturbance [5]. It was also demonstrated that skin diseases can cause anxiety, depression, anger and embarrassment, which lead to social isolation and absenteeism at work and school [6]. This study was undertaken with the objective to find the demographic profile, clinical morphology and quality of life in patients suffering from scabies.
Materials and Methods
It was a non-interventional, cross-sectional study conducted at the Department of Dermatology, in a rural based tertiary care center.
We conducted the study for a period of 6 months from March to August 2015, after obtaining ethical clearance from the ethical committee of the hospital. It included all newly diagosed patients attending skin OPD with clinical features suggestive of scabies. All adults and children greater than 5 years of age with diagnosis of scabies were included in the study. Diagnostic criteria included itching, most severe in the night time, family history of itching, and characteristic lesions like papules, excoriations and burrows at classical sites like finger webs, genitals, etc. Patients with atypical and crusted scabies, pregnant and lactating women and children less than 5 years were excluded from the study. Patients simultaneously having other chronic cutaneous and systemic conditions like asthma, epilepsy, diabetes, hypertension, acne, psoriasis, etc were also excluded from the study. The diagnosis was made clinically. An informed consent was taken from all the patients. Data on demographic details, clinical findings, family history and past history was noted in predesigned proforma. Questionnaire about quality of life impairment was given to the patients to be filled and detailed analysis was done. Modified Dermatology Life Quality Questionnaire (mDLQI) for scabies by Worth et al., was modified slightly as per the requirement of Indian population [7]. We omitted one question from the list pertaining to the dressing pattern in patients of scabies as we did not find any relevance in our patients.
For children, the questionnaire was different from adults and was filled by either of their parent. In 10 patients, Questions were validated by giving them in local vernacular language at the start of study [Table/Fig-1].
Modified dermatological life quality questionaire.
| [A] Modified Dermatological Life Quality Questionaire In Adult Scabies Patients |
| During the last week did you feel embarrassed or ashamed because of your skin condition A/B/C/D |
| During last week did your skin condition affect your work activities A/B/C/D |
| During the last week did your skin condition cause problem in your sexual relationship A/B/C/D |
| During the last week did your skin condition affect your social contacts A/B/C/D |
| During the last week did u feel inferiority complexion or depressed A/B/C/D |
| [B] Modified Dermatological Life Quality Questionaire In Children Scabies Patients |
| During the last week did you feel embarrassed or ashamed because of your skin condition A/B/C/D |
| During last week did your skin condition affect your school work 4/3/2/1 |
| During last week did your skin condition affect your playing 4/3/2/1 |
| During the last week did you have trouble with other children calling you names or teasing you because of your skin condition 4/3/2/1 |
| During the last week did your skin condition affect your friendships 4/3/2/1 |
| 4 Very much3 Quite a lot2 Only a little1 Not at all |
We graded the effect on quality of life in patients of scabies. Total score was calculated by summing the score of each 5 question resulting in a possible maximum of 15 and minimum of 0. The higher the score, the more the quality of life is impaired. A score of 0-1 shows no effect at all on patients life, 2-5 translates to mild quality of life impairment, 6-10 indicates moderate impairment and 11-15 demonstrates severe impairment.
The descriptive statistics were used to describe the quantitative data and qualitative data was presented using frequency and analysed using Chi-Square test.
Results
Total of 102 new scabies patients attending skin OPD during 6 months duration were included in the study. Out of total 102 patients, 52(50.98%) were males and 50(49.01%) were females. The most common age group affected was 21-40 years in 45(44.11%) patients [Table/Fig-2].
| Age (y) | Number (%) |
|---|
| 5-12 | 40 (39.2%) |
| 13-20 | 4(4%) |
| 21-40 | 45(44.11%) |
| 41-60 | 12(11.76%) |
| 61-80 | 1(0.98%) |
| Sex |
| Males | 52(50.98%) |
| Females | 50 (49.01%) |
| Urban/Rural |
| Urban | 40(39.21%) |
| Rural | 62(60.78%) |
| Literacy |
| Literate | 68 (66.66%) |
| Illiterate | 34 (33.33%) |
| Occupation |
| Student | 42(41.17%) |
| Housewife | 21(20.58%) |
| Worker, farmer, labourer | 9(8.82%) |
| Business | 3(2.94%) |
| Professional | 2(1.96%) |
| Job | 13(12.74%) |
| Retired | 2(1.96%) |
| Others | 10(9.8%) |
Forty (39.21%) patients belonged to urban area and 62(60.78%) belonged to rural area. Total 68(66.6%) patients were literate. Total 42(41.17%) students were affected followed by 21(20.58%) housewives [Table/Fig-2].
Total 101(99%) patients presented with itching and 81(79.4%) patients had night aggravation of itching leading to sleep disturbance [Table/Fig-3].
Clinical profile of patients with scabies.
| Complaints | Number (%) |
|---|
| Itching | 101 (99%) |
| Night aggravation | 81(79.4%) |
| Skin lesions | 86 (84.3%) |
| Past history |
| Present | 10(9.8%) |
| Absent | 92(90.19%) |
| Family history |
| Present | 61(59.80%) |
| Absent | 41(40.19%) |
| Secondary infections |
| Present | 22(21.56%) |
| Absent | 80(78.43%) |
| Lymph node involvement |
| Present | 3(2.94%) |
| Absent | 99(97%) |
Ten (9.8%) patients presented with history of similar complain in the past. Sixty one (59.80%) patients gave positive family history of similar complaints. Secondary infections were present in only 22(21.56%) patients. Lymph node involvement was seen in 3(2.94%) cases [Table/Fig-3].
Multiple sites were affected in almost all patients. Most common site affected was interdigital cleft in 73.52% cases followed by hands in 61.76% and genitals in 40.19% cases [Table/Fig-4].
Topographic distribution of lesions.
| Sites | no. (%) |
|---|
| Interdigital cleft | 75 (73.52%) |
| Hands | 63 (61.76%) |
| Wrist | 29 (28.43%) |
| Arms | 31 (30.39%) |
| Forearms | 32 (31.37%) |
| Elbow | 12 (11.76%) |
| Axilla | 13 (12.74%) |
| Legs | 20 (19.60%) |
| Foot | 10 (9.8%) |
| Abdomen | 34 (33.33%) |
| Thorax | 8 (7.8%) |
| Nipple | 4 (3.9%) |
| Perimamillary | 15 (14.7%) |
| Back | 15 (14.7%) |
| Buttocks | 17 (16.6%) |
| Genitals | 41 (40.19%) |
| Inguinal | 10 (9.8%) |
| Face | 5 (4.9%) |
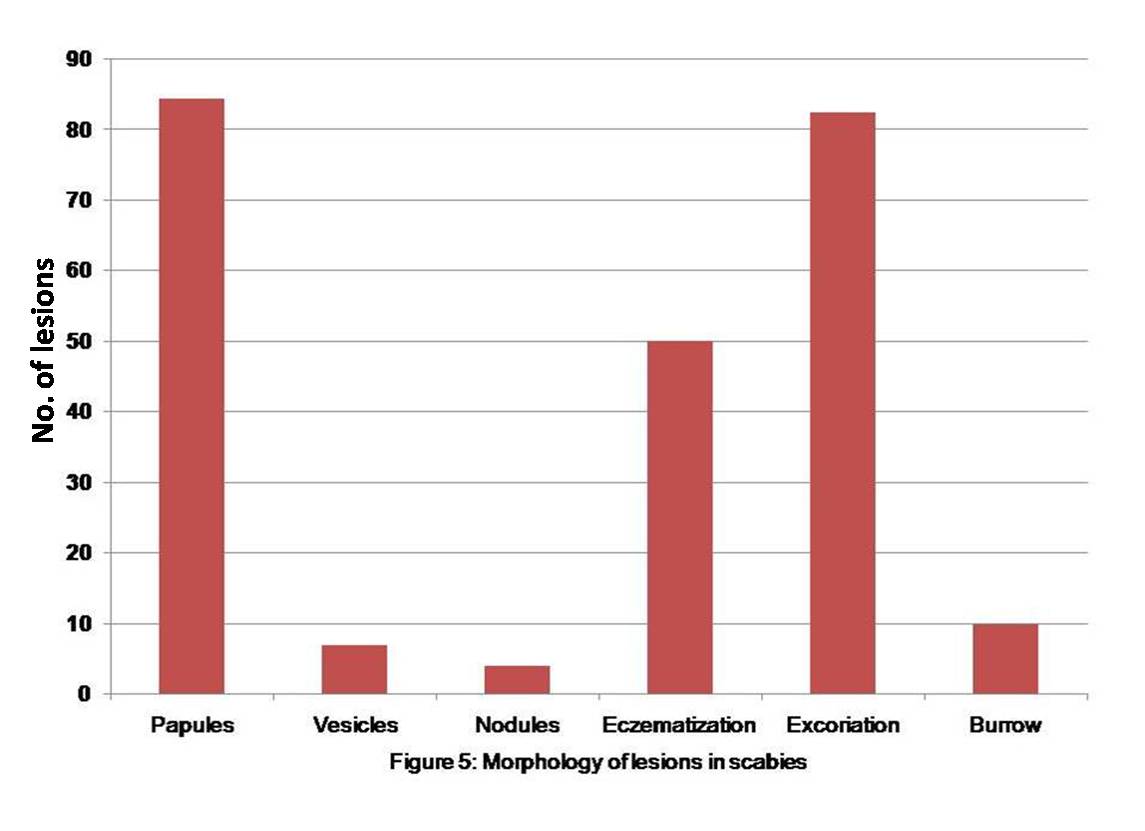
Most common lesion seen was papules in 86(84.3%) cases followed by excoriations in 84(82.3%) cases [Table/Fig-5].
Morphology of lesions in scabies.
In children the domain affected maximum was work at school in 15(37.5%) followed by play and feeling of embarrassment in 12(30%) cases each [Table/Fig-6]. In adults major domain affected was work in 46(74.2%) cases followed by feeling of embarrassment in 40(64.5%) patients [Table/Fig-7].
The impairment in the quality of life in children.
| Severity of Impairment in quality of life (n=40) | Sex wise distribution of impairment (n=40) |
|---|
| Questions | A (very much) | B (quite a lot) | C (only a little) | D (not at all) | Male (n = 22) | Female (n = 18) | Total (n = 40) | p-value |
|---|
| Feeling embarrassed | 0 | 2(5%) | 10(25%) | 28(70%) | 5(22.7%) | 7(38.8%) | 12(30%) | 0.104 |
| Affected school work | 1(2.5) | 3(7.5) | 11(27.5) | 25(62.5) | 9(40.9%) | 6(33.3%) | 15(37.5%) | 0.613 |
| Affected playing | 1(2.5% | 3(7.5) | 8(20%) | 28(70%) | 6(27.3%) | 6(33.3%) | 12(30%) | 0.678 |
| Experienced teasing | 0 | 2(5%) | 6(15%) | 32(80%) | 3(13.6%) | 5(27.7%) | 8(20%) | 0.495 |
| Affected friendship | 0 | 1(2.5%) | 3(7.5%) | 36(90%) | 1(4.5%) | 3(16.6%) | 4(10%) | 0.098 |
Impairment in the quality of life in adult.
| Severity of Impairment in quality of life (n=62) | Sex wise distribution of impairment (n=62) |
|---|
| Questions | A (very much) | B (quite a lot) | C(only a little) | D(not at all) | Male (n=30) | Female (n=32) | Total (n=62) | p-value |
|---|
| Feeing embarrassed | 1(1.6%) | 8(12.9) | 31(50%) | 22(35.4%) | 19(63.3%) | 21(65.6%) | 40(64.5%) | 0.809 |
| Affected the work activities | 1(1.6%) | 10(16.1%) | 35(56.4%) | 16(25.8%) | 24(80%) | 22(68.7%) | 46(74.2%) | 0.579 |
| Problem in sexual relationship | 0 | 7(11.3%) | 30(48.4%) | 25(40.3%) | 20(66.6%) | 17(53.1%) | 37(59.7%) | 0.545 |
| Affected social contacts | 0 | 10(16.1%) | 26(48.3%) | 26(41.9%) | 19(63.3%) | 17(53.1%) | 36(58.1%) | 0.621 |
| feeling depressed | 0 | 7(11.3%) | 31(50%) | 23(37.1%) | 21(70%) | 17(53.1%) | 38(61.3%) | 0.374 |
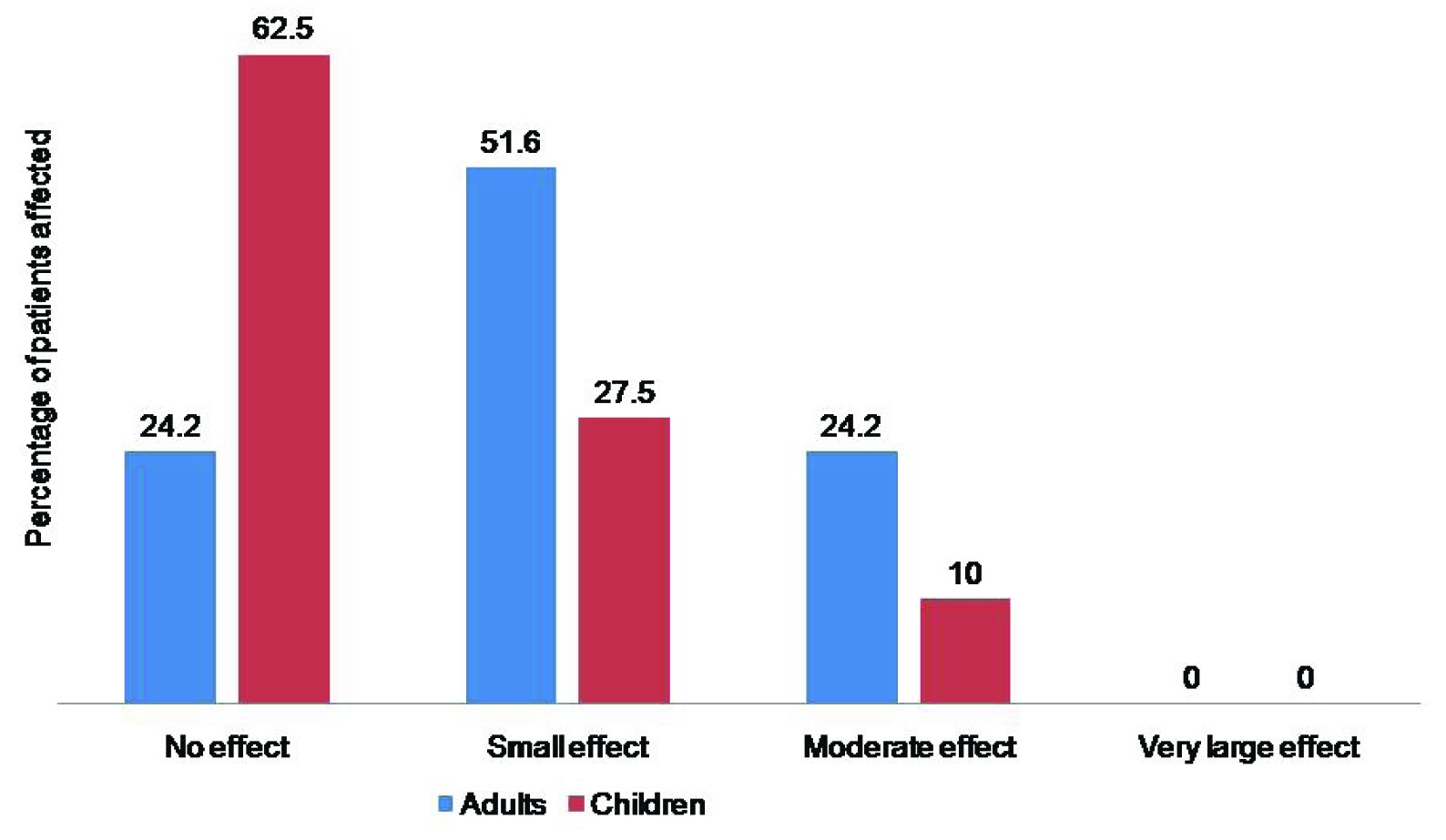
Maximum 32(51.6%) adults had small effect on quality of life while 25(62.5%) children reported no or minimal effect on quality of life. None of the patient had severely impaired quality of life [Table/Fig-8].
Effect on quality of life in adults and children due to scabies.
Discussion
Scabies is a common parasitic infestation globally with worldwide, estimation of 300 million cases occurring annually [8]. It has been considered to be a public health problem in the developing countries for decades; still, there has been little progress in the control on a global scale [9]. It occurs commonly in tropical climate, in poor people who live in crowded conditions and cannot adopt proper hygienic measures [1].
A person infested with mites can spread scabies even if he or she is asymptomatic [10–12]. Transmission of scabies occurs via skin-to-skin contact, which may take up to 20 minutes [13], so spread mainly occurs within families where children, share a sleeping space, or in the adult population via sexual contact.
A delayed-type hypersensitivity reaction to mite allergens causes skin inflammation resulting in papules and pruritus. Excoriation of the lesions leads to secondary bacterial infections, eczema and long-term health consequences in the form of post streptococcal glomerulonephritis [14].
The most common age group affected in our study was 21-40 years in 44.11% patients followed by 5-12 years of age group in 39.2% patients while Das S et al., study found 9% patients were in the 0-5 years age group, 22% in both 6-15 years and 16-30 years of age group [15]. Sambo et al., who mainly studied the prevalence of scabies in school going children, reported 55.8% patients were in the age 5–8 years, whereas 44.2% patients were in the age range from 9–12 years [8].
Maximum 60.78% patients in our study belonged to rural area where there is shortage of water. Water shortage or inadequate water supply leads to poor personal hygiene and thus increased risk of transmission of scabies [16].
Males were almost equally affected as females in our study in contrast to study by Das S et al., where males outnumbered females [15]. In a predominantly rural setup, males report more frequently than the conservative female population. Study by Sambo et al., reported almost equal male to female ratio of 1:1 [8].
Pruritus is particularly severe at night in scabies and thus sleep disturbances are common [17]. Total 79.4% patients had night aggravation of itching leading to sleep disturbance.
History of similar complain in past was given in 9.8% cases which was quite less than study by Das S et al., where previous affection with scabies was seen in 25% cases [15].
Lesions of scabies are due to allergic reaction to the mites and are usually bilateral, commonly seen on finger webs, side of fingers, flexor surface of wrist, along the waistline, elbow, anterior axillary fold, genitalia, buttocks, umbilicus and areola of female breast [11]. Most common lesion seen in our study was papules in 84.3% followed by excoriations in 82.3% cases. Complications in the form of eczematisation were seen in 50% cases and secondary infections were seen in 21.56% patients. Das S, et al., found papular lesions in 76%cases, papulovesicular and eczematous lesions in 23 and 24% cases respectively [15].
Multiple sites were affected in an individual. Most commonly affected site was interdigital cleft in 73.52% followed by hands in 61.76% and genitals in 40.19% cases whereas study by Das S et al., showed genitalia commonest site with 60%, followed by finger webs in 57% cases [15]. Study by Sunil Agrawal et al., showed generalized involvement in 25(60.97%), webs spaces in 07(17.07%), wrists in 04(9.75%), glans in 01(2.43%) and umbilicus in 01(2.43%) cases [18].
In the developing world, scabies has become an accepted part of everyday life. Infestation with scabies significantly affect the quality of life. Worth et al., have suggested that in many areas where scabies is endemic, quality of life is so poor that people do not consider scabies to be a problem and infestation is considered routine [7].
The itching has been found to cause moderate to severe sleep disturbance in the vast majority of sufferers [19] and as the scabetic skin characteristically include exposed areas of skin, social stigma is an issue. There has been an increasing interest in assessing the quality of life of patients with skin diseases as well as in the development of methods of assessment [4].
Patients with skin diseases may have their lives affected in many ways leading to anxiety, depression, anger and embarrassment, which lead to social isolation and absenteeism at work and school.
Scabies infestation has a negative impact on the quality of life for infected individuals (similar to that of psoriasis) resulting in substantial stigmatization and ostracism [20] as well as affecting social and sporting activities [20].
Data of Jin-gang et al., confirm that scabies patients frequently feel restrictions in their personal relationships [21].
Studies outside India have shown that scabies significantly impairs the quality of life, but in India this is the first study as per our literature search. In our study, the major domain affected in adults was work activity in 74.2% cases followed by feeling of embarrassment in 64.5% patients. In children, domain affected maximum was work at school in 37.5% followed by play and feeling of embarrassment in 30% each. Work is affected due to excessive itching and disturbance of sleep. In country like ours where majority of population is living on daily wages, major domain affected in the form of work activity is going to affect patient’s livelihood. It is very important to diagnose the condition at the earliest, improve hygienic conditions and educate and spread awareness about the disease.
Data collected at Xi’an Jiatong University (China) in 2008 using the DLQI Questionnaire indicated that the personal relationships domain was most affected by scabies infestation, with the symptoms and feelings domain scoring second highest [21]. A more recent study, in a Brazilian urban slum in Fortaleza found that the majority of female participants had a feeling of shame and 30% had social exclusion as a result of scabies infestation [7]. Therefore, the social impact of the disease should not be underestimated.
Skin diseases may cause problems in personal relationships and sexual partners may be repelled by the presence of skin lesions in the genital area. In our study sexual relation was affected in 11.3% cases.
Mild effect on quality of life was seen in 51.6%, moderate effect in 24.2% of adults suffering from scabies while none showed a large impairment on quality of life. In children 27.5% had mild and 10% had moderate impact on the quality of life.
As per Worth et al., categorization of mDQLI showed that about one-fifth of the patients did not feel any restriction. Scabies had a mild effect on quality of life in 28.1% (adults) and 39.7% (children). A moderate impact on quality of life was seen in 36.8% of adults and 25.9% of children and a large or very large effect on their quality of life was seen in 13.9% of patients with scabies [7].
Though it is a disease which gets cured if treatment is taken properly, it affects the quality of life though for less period of time. It is important to emphasise to patients about the need for treatment to all family members simultaneously to avoid recurrent infections. Assessing quality of life can help provide patients with better service, by acknowledging their real needs and interfering with treatment decisions.
Limitation
Small sample size was the limitation of our study as we had excluded children less than 5 years of age, pregnant and lactating mothers and patients of crusted and atypical scabies.
Conclusion
Embarrassment, shame, stigmatization and social exclusion were frequently perceived restrictions in adults compared to children. In this setting, scabies is an important health problem requiring action by healthcare providers.
Not only chronic conditions like vitiligo and psoriasis affects quality of life but infectious diseases like scabies also can affect quality of life. Importance of proper counselling regarding treatment and hygiene need to be emphasised to the patients.