A Rare Case of Pyogenic Granuloma with a Natal Tooth
Nidhi Agarwal1, Dipanshu Kumar2, Alaka Vaish3, Ashish Anand4
1 Professor and Head, Department of Pedodontics and Preventive Dentistry, IDST, Modinagar, Ghaziabad, Uttar Pradesh, India.
2 Reader, Department of Pedodontics and Preventive Dentistry, IDST, Modinagar, Ghaziabad, Uttar Pradesh, India.
3 Postgraduate Student, Department of Pedodontics and Preventive Dentistry, IDST, Modinagar, Ghaziabad, Uttar Pradesh, India.
4 Senior Lecturer, Department of Pedodontics and Preventive Dentistry, IDST, Modinagar, Ghaziabad, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Nidhi Agarwal, Professor and Head, Department of Pedodontics and Preventive Dentistry, IDST, Modinagar, Ghaziabad, Uttar Pradesh, India.
E-mail: doc.nagarwal@gmail.com
Natal teeth are teeth present in the oral cavity at the time of birth. It is extremely rare to find natal teeth in association with pathological conditions of the oral cavity. Pyogenic granuloma is a type of inflammatory hyperplasia that appears as an over exuberant connective tissue response to a stimulus or injury, in the present case the injurious agent is the natal tooth. The parents of the eight day old male infant brought the child with a natal tooth associated with a soft tissue lesion growing from the gum pad. A provisional diagnosis of pyogenic granuloma was made on behalf of the clinical findings which were confirmed by histopathology. The natal tooth was extracted and the lesion was surgically excised. Complete healing of the gumpad took place after excision of the lesion and extraction of the natal tooth and the child was able to feed normally within a week. The purpose of this case report is that Pediatric Dentist should be aware of this rare unusual clinical presentation and plan for an appropriate treatment modality in order to avoid any future complications.
Granulation tissue, Hypoplastic enamel, Infant, Predeciduous teeth, Supernumerary
Case Report
The parents of an eight-day-old male child reported to the Department of Pediatric and Preventive Dentistry with the chief complaint of a mobile tooth along with a growth in the gums in the lower jaw of their child. The tissue was small at the time of birth but gradually increased in size leading to difficulty in feeding and the infant exhibited pain during suckling, consistently decreasing the frequency of maternal breast feeding episodes. Medical history revealed a healthy infant born of a normal, uncomplicated, full term pregnancy. Dental history revealed that he was born with a natal tooth attached to a mass of soft tissue on the lower alveolar ridge in the central incisor region which was small at the time of birth but continuously increased in size to its present dimension. No abnormal extra oral finding was noted; however, intraoral examination revealed a solitary natal tooth with Grade-1 mobility present on the anterior mandibular alveolar ridge which was associated with an exophytic pedunculated growth of about 8mm in width and 5mm in height [Table/Fig-1]. The lesion was red in color, soft in consistency, smooth textured and was attached to the ridge by a narrow base with slight tenderness and bleeding was present from the base of the tissue on palpation. A provisional diagnosis of pyogenic granuloma associated with natal tooth was made on the basis of clinical findings. The differential diagnoses made was epulis, mesenchymal tumor, and gingival cyst of the newborn, pulp polyp or gingival hamartoma. Due to the appearance, extent of the lesion, age of the patient and increasing difficulty in feeding, it was decided to extract the natal tooth along with the soft tissue mass under local anesthesia.
The figure shows infant having natal tooth with pyogenic granuloma. Intraorally, the white conical structure on the left side is natal tooth while the yellowish raised structure is the granuloma.

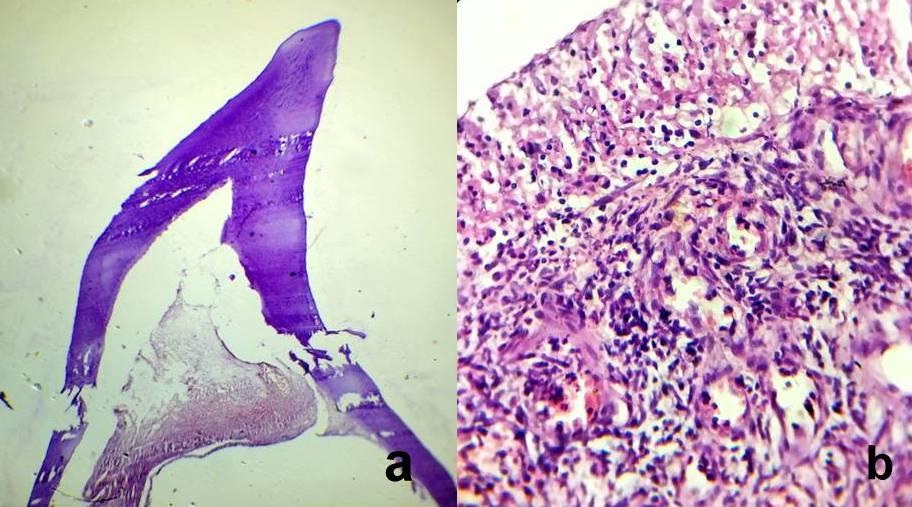
A Pediatrician was consulted and vitamin K was administered intramuscularly. Local infiltration was done with 2% xylocaine (with adrenaline) and the natal tooth was extracted without any complications followed by the excision of the tissue from its base. The tooth and the tissue both were sent for histopathological examination [Table/Fig-2]. The extracted tooth was hypo- mineralized, shell shaped and poorly fixed to the alveolus by gingival tissue with absence of any root formation. The histological finding of the tooth specimen showed formation of normal dentin and a large pulp chamber with inflamed pulp tissue [Table/Fig-3a]. The histological section of the granulomatous tissue revealed the presence of inflamed connective tissue stroma, with inflammatory cells, collagen fibers, fibroblasts and endothelium lined blood vessels [Table/Fig-3b]. Thus, the final diagnosis of pyogenic granuloma was confirmed. One week after procedure, the post-surgical site showed adequate healing with no signs of recurrence. At three month follow up visit of the patient the area had healed completely with the child feeding normally [Table/Fig-4].
Extracted natal tooth showing lack of root formation.

Photomicrographs (H&E, 40X) of the natal tooth and pyogenic granuloma.
Complete healing of the alveolar ridge at 3 months.

Discussion
Natal teeth are teeth present in the oral cavity at the time of birth. Majority of the natal teeth represent early eruption of normal dentition with only 1% to 10% present as supernumerary [1]. The most common site is the lower anterior region and the affected teeth are the lower primary central incisors [2]. Natal teeth may be similar to normal primary dentition in size and shape; though are smaller, conical, yellowish, and have hypoplastic enamel and dentin with poor or absent root formation [2]. Presence of natal teeth may cause complications such as excessive mobility, difficulty in sucking, injury to mother’s breast and sublingual ulceration (Riga-Fede disease). Peuch (1876) reported a prevalence of 1:30000 in a sample of 60000 children whereas Almeida and Gomide (1996) stated 1:21.6 in 1019 children [3]. The occurrence of a natal tooth in association with any pathology is even rarer with only few cases associated with pathological gingival growths such as pyogenic granuloma [4,5], reactive fibrous hyperplasia [6] and pulp polyp [7] have been reported in the dental literature.
Pyogenic granuloma is a type of inflammatory hyperplasia that appears as an over exuberant connective tissue response to a stimulus or injury [8]. It usually develops as a response to local injury or chronic irritants like calculus, foreign bodies or chronic biting of soft tissues. It is a special type of inflammatory hyperplasia in which the granulomatous stage appears dark red, is asymptomatic, soft and spongy on palpation and bleeds easily. The lesion is generally an elevated, pedunculated, or sessile mass with a smooth, lobulated surface which might become ulcerated, and can be enveloped by yellow-tan fibrinous exudates [9,10].
Pyogenic granuloma should be differentiated from other similar lesions such as epulis, mesenchymal tumors, gingival cysts of the newborn, pulp polyp or gingival hamartoma. Gingival cysts of the newborn are neither reactive lesion, nor they are associated with erupting teeth, and are smaller in diameter (about 1mm). Also they are normally sub-epithelial and whitish in color [8]. Eruption cysts generally resolve after the eruption of the involved tooth and no surgical intervention is needed [11]. Hemangiomas may also be considered as a possible diagnosis because of the color and vascular nature of the lesion. Although the sites of occurrence of most hemangiomas are the lips, tongue, buccal mucosa and palate [8].
The origin of pyogenic granuloma is related to chronic irritants [10] which in the present case was the natal tooth. The lesion was small at the time of birth but enlarged within a span of few days which might be due to the trauma that occurred during suckling in the presence of the natal tooth. The unsightly appearance and difficulty in feeding compelled the parents for medical consultation. Surgical removal of the pyogenic granuloma from the connective tissue from which the lesion arises with the elimination of the aetiological factors is indicated. Inflammatory hyperplasia may shrink considerably as the inflammation subsides on removing the aetiological factor, but if the insult is allowed to continue the granulomatous lesion will increase in size and show fibrosis in regions away from the areas being irritated. Therefore, sometimes if the fibrous component is larger, the lesion may not regress completely [12]. Moreover, in all the previously reported cases [4,5] the natal tooth were removed either at home by the parents or by a Pediatrician immediately after birth. It was seen that the soft tissue mass if left behind gradually increases in size even after removal of the tooth and had to be excised later. Hence, it was decided to treat this case by the extraction of natal tooth followed by the surgical excision of the lesion under necessary precautions. The wound healing was complete and no recurrence was observed after follow-up of three months.
Conclusion
Natal tooth can be a source of trauma in the oral cavity of a new born child resulting in the development of inflammatory hyperplastic conditions. It is important for the Pediatric Dentists to be aware of these special cases and plan for an appropriate treatment modality in order to avoid any future complications.
[1]. Kates G A, Needleman H L, Holmes L B, Natal and neonatal teeth: a clinical studyJ Am Dent Assoc 1984 109(3):441-43. [Google Scholar]
[2]. Anegundi RT, Sudha P, Kaveri H, Sadanand K, Natal and neonatal teeth: A report of four casesJ Indian Soc Pedo Prev Dent 2002 20:86-92. [Google Scholar]
[3]. Cunha RF, Boer FA, Torriani DD, Frossard WT, Natal and neonatal teeth: Review of the literaturePediatr Dent 2001 23:158-62. [Google Scholar]
[4]. Muench MG, Layton S, Wright JM, Pyogenic granuloma associated with a natal tooth:Case reportPediatr Dent 1992 14:265-67. [Google Scholar]
[5]. Sanjuan KV, Álvarez AL, Ricardo JH, Teliangectaticum granuloma associated to a natalRev Odont Mex 2016 20:29-32. [Google Scholar]
[6]. Singh S, Subba Reddy VV, Dhananjaya G, Patil R, Reactive fibrous hyperplasia associated with a natal toothJ Indian Soc Pedod Prev Dent 2004 22:183-6. [Google Scholar]
[7]. Vergotine RJ, Hodgson B, Lambert L, Pulp polyp associated with a natal tooth: Case ReportJ Clin Pediatr Dent 2009 34:161-163. [Google Scholar]
[8]. Shafer WG, Hine MK, Levy BM, Bacterial, Viral and Mycotic Infections, in A Textbook of Oral Pathology 1983 4thedPhiladelphiaWB Saunders:359-61. [Google Scholar]
[9]. Regezi JA, Scuibba JJ, Red-Blue Lesions in Oral Pathology: Clinical-Pathologic Correlations 1989 PhiladelphiaWB Saunders:131-132. [Google Scholar]
[10]. Shafer WG, Hine MK, Levy BM, Bacterial Infections of the Oral Cavity, in Shafer’s Textbook of Oral Pathology 2006 5th edElsevier:459-60. [Google Scholar]
[11]. Peters RA, Schock RK, Oral cysts in newborn infantsOral Surg Oral Med Oral Pathol 1971 32:10-14. [Google Scholar]
[12]. Wood NK, Goaz PW, Peripheral Oral Exophytic Lesions, In Differential Diagnosis Of Oral Lesions 1989 3rd edMosby:150-52. [Google Scholar]