Ameloblastic Carcinoma: A Report of Three Cases
Sravya Kodati1, Sumit Majumdar2, Divya Uppala3, Madhurya Namana4
1 Postgraduate Student, Department of Oral Pathology and Microbiology, GITAM Dental College and Hospital, Visakhapatnam, Andhra Pradesh, India.
2 Professor and Head, Department of Oral Pathology and Microbiology, GITAM Dental College and Hospital, Visakhapatnam, Andhra Pradesh, India.
3 Reader, Department of Oral Pathology and Microbiology, GITAM Dental College and Hospital, Visakhapatnam, Andhra Pradesh, India.
4 Postgraduate Student, Department of Oral Pathology and Microbiology, GITAM Dental College and Hospital, Visakhapatnam, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Divya Uppala, Department of Oral Pathology and Microbiology, GITAM Dental College and Hospital, Visakhapatnam, Andhra Pradesh, India.
E-mail: uppala.divya@gmail.com
Malignant odontogenic tumours are rare and represent approximately 1% of all oral malignancies. Ameloblastic carcinoma is a rare odontogenic tumour, which is aggressive in nature with extensive local bone destruction that has retained the features of ameloblastic differentiation and also exhibits cytological features of malignancy. It occurs primarily in the mandible in a wide range of age groups. It may arise de-novo or in pre-existing ameloblastoma or odontogenic cyst. The purpose of this report is to present three cases of ameloblastic carcinoma with varying presentations as central and peripheral entities.
Ameloblastoma, Extraosseous, Intraosseous, Mandible
Case 1
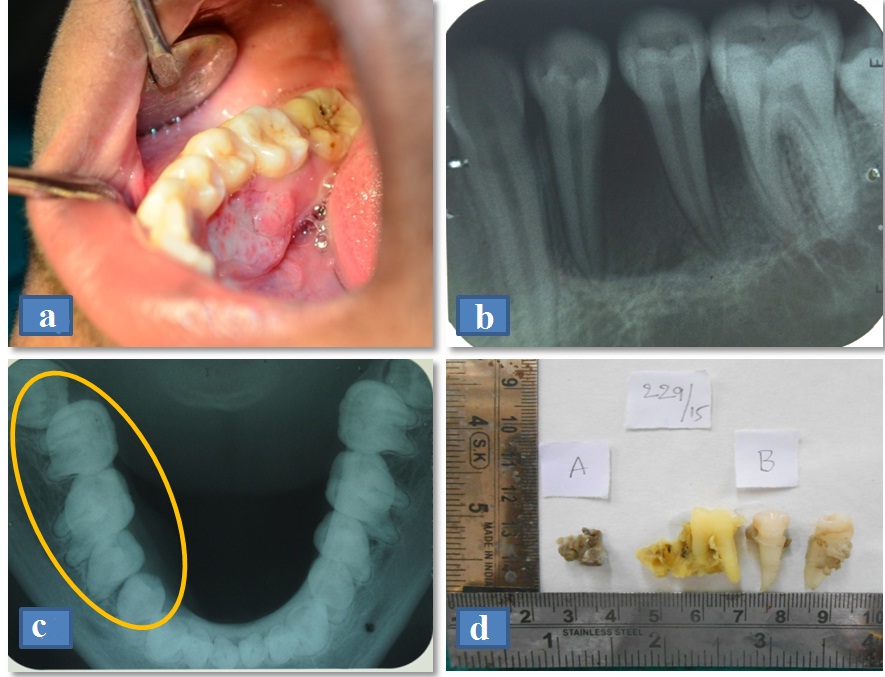
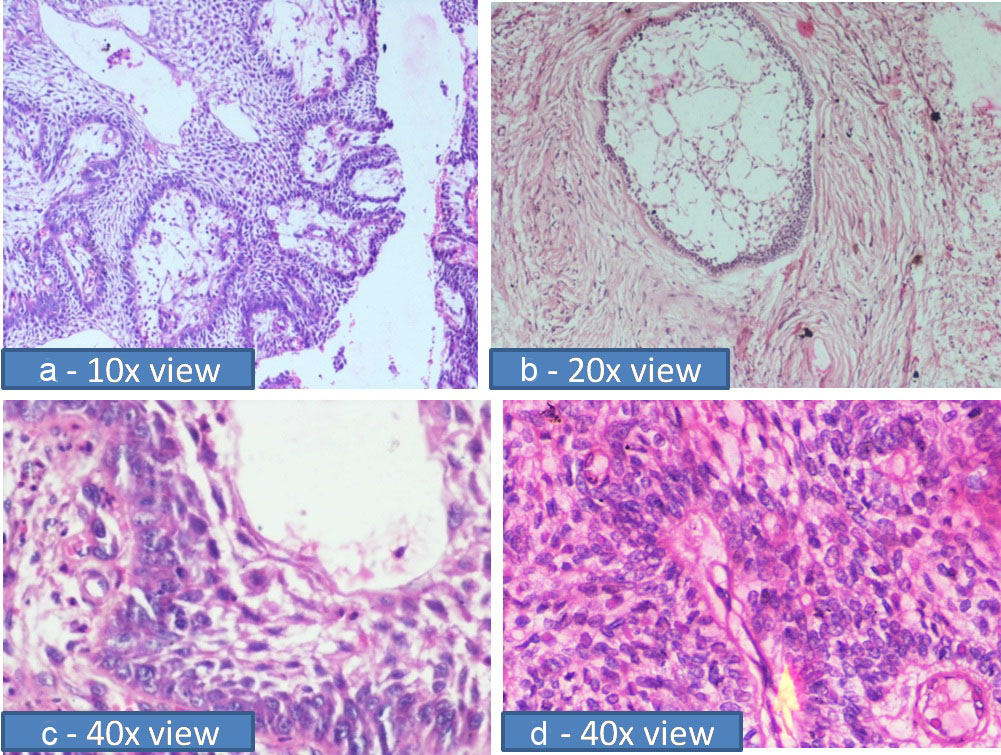
A 16-year-old male patient reported to the hospital with a chief complaint of slow growing mass in the gums since 3 months. There was no significant past medical and dental history. On Intraoral examination there was an oval shaped, solitary, sessile, ill-defined growth on the lingual gingiva of tooth # 44, 45, 46 region, measuring 3 × 2cm in size with ulceration on its surface [Table/Fig-1a]. On palpation, the growth was ill-defined, tender and soft to firm in consistency. A provisional diagnosis of fibroma was made. Radiographic investigations including Intra-Oral Periapical Radiograph (IOPA), occlusal view revealed saucerization of the alveolar bone [Table/Fig-1b,c] and an incisional biopsy of the soft tissue growth was taken under local anesthesia. Excisional biopsy was performed and the gross specimen is shown [Table/Fig-1d]. The Haematoxylin and Eosin stained soft tissue sections revealed odontogenic epithelium arranged in the form of islands with peripherally arranged columnar cells with central stellate reticulum like cells. Loss of polarization, hyperchromatic nuclei, increased mitotic activity were seen [Table/Fig-2]. The final diagnosis was follicular ameloblastic carcinoma.
a) Clinical picture shows solitary, sessile, ill-defined growth on the lingual gingiva of tooth # 44, 45, 46; b) Intraoral periapical radiograph shows ill-defined radiolucency; c) Occlusal radiograph shows saucerization of alveolar bone; d) Excisional biopsy – gross specimen.
(a&b): Photomicrograph showing ameloblastic epithelial islands arranged in the form of strands and follicles (H&E, 10x & 20x magnification); (c&d): Photomicrograph showing vesicular, hyperchromatic nuclei, increased nuclear cytoplasmic ratio (H&E, 40x magnification).
Case 2
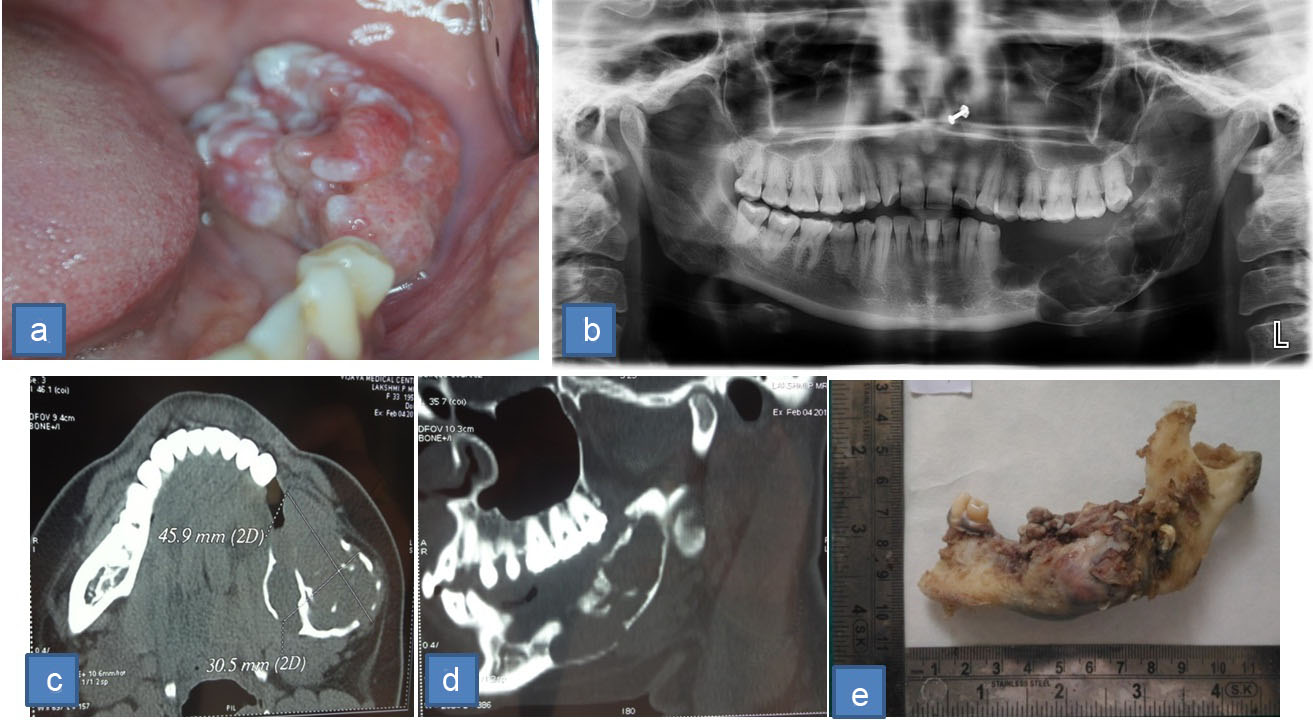
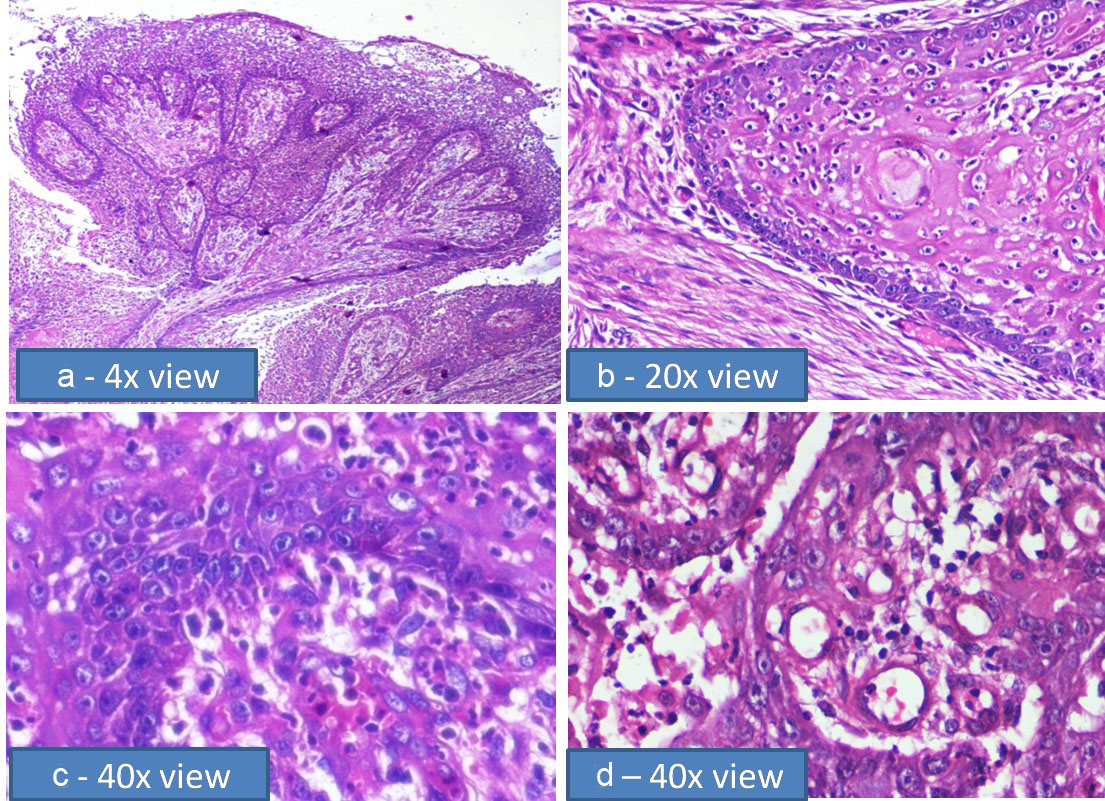
A 33-year-old female patient reported to the hospital with the chief complaint of growth on the left side of posterior mandible since 2 years. Her past dental history revealed extraction of third molar 5 years back and subsequent removal of first and second molar in a span of one year due to mobility. One year after extraction, a growth started in the same region associated with occasional bleeding and difficulty in mouth opening. Earlier biopsy done in the same region diagnosed the growth as ameloblastic carcinoma. But, the patient neglected her condition, only to report after a year with a bigger and painful swelling. On examination, there was a well-defined solitary proliferative growth of 2 x 1cm size in the left alveolar ridge extending from tooth # 45 to retromolar area [Table/Fig-3a]. A solitary right submandibular lymph node of 0.5 x 1cm size, firm in consistency was palpable. Orthopantamogram (OPG) revealed multilocular radiolucency involving the body, ramus, coronoid process of the mandible [Table/Fig-3b]. CT scan depicted the size of the lesion as 45.9 x 30.5mm [Table/Fig-3c], thinning of inferior border of the mandible [Table/Fig-3d]. Incisional biopsy was again performed which confirmed the previous diagnosis. Hemimandibulectomy was done with free surgical margins [Table/Fig-3e]. The Haematoxylin and Eosin stained soft tissue section demonstrated hyperproliferative epithelium in plexiform pattern [Table/Fig-4a], loss of polarization in the peripheral cells, acanthomatous changes in the central cells, hyperchromatic nuclei and keratin pearl formation [Table/Fig-4b]. Higher magnification exhibited increased nuclear cytoplasmic ratio, increased and abnormal mitotic figures and dyskeratosis [Table/Fig-4c,d].
a) Intraoral picture depicting well-defined solitary proliferative growth; b) OPG depicts multilocular radiolucency involving ramus & body of the mandible; (c&d): CT scan depicting a homogenous mass in the left mandible; e) Excisional biopsy – gross specimen.
a) Hyperproliferative epithelium in plexiform pattern (H&E, 4x magnification); b) Dysplastic features seen in the central cells of the epithelial island such as hyperchromatic nuclei, keratin pearl formation (H&E, 20x magnification); (c&d): Malignant features – vesicular nuclei, increased nuclear cytoplasmic ratio (H&E, 40x magnification).
Case 3
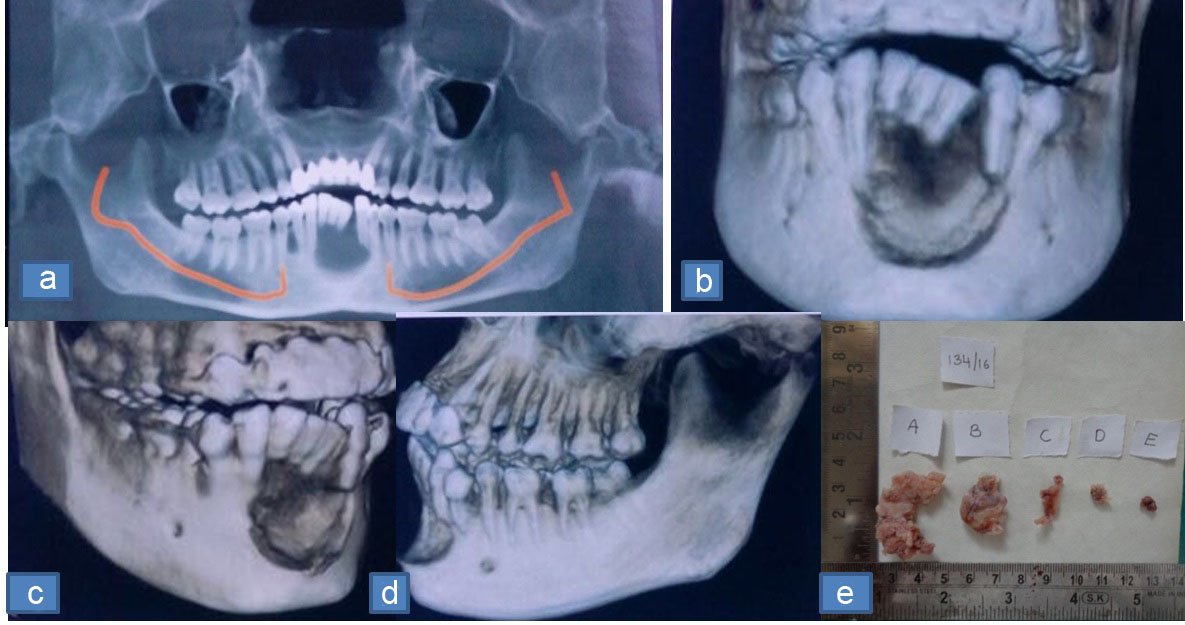
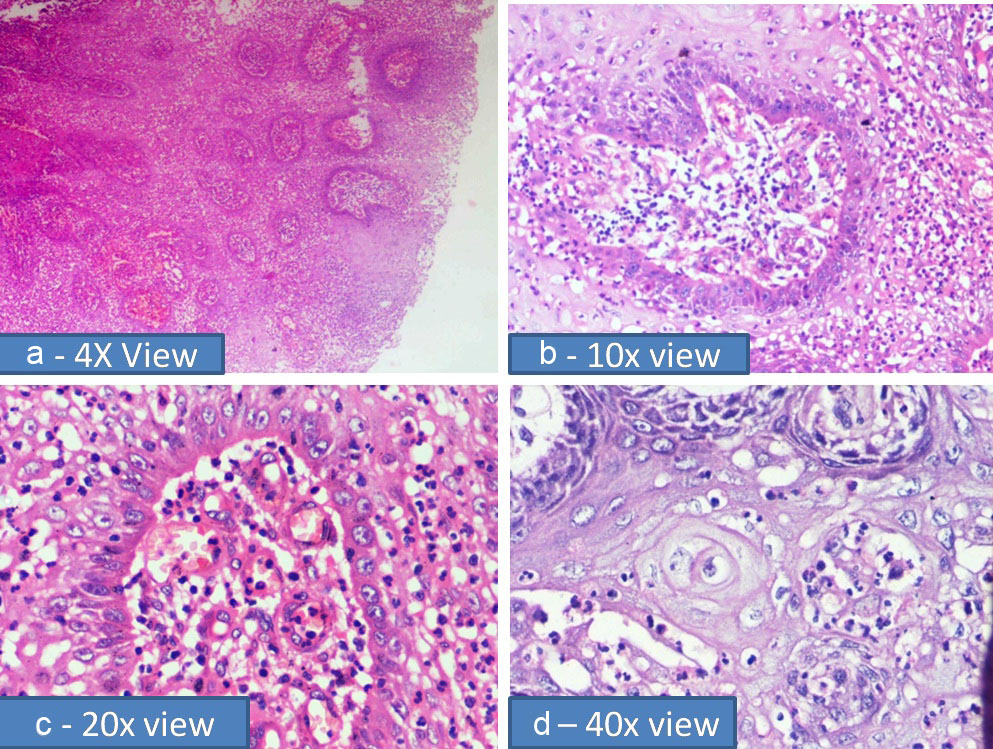
A 25-year-old male patient reported with a chief complaint of swelling in the anterior mandible since 3 months. The swelling extended from mesial aspects of tooth # 34 to 44, firm in consistency, mobility of the anterior teeth and associated with obliteration of the labial vestibule. OPG revealed well circumscribed destructive lesion in the anterior mandible associated with root resorption of tooth # 31, 32, 41, 42 [Table/Fig-5a-d]. Incisional biopsy [Table/Fig-5e] was performed under local anaesthesia and microscopic examination revealed odontogenic epithelial islands with peripheral columnar cells and central stellate reticulum like cells. The epithelium exhibited loss of polarization, increased nuclear cytoplasmic ratio, increased bizarre mitotic figures, dyskeratosis, hyperchromatic and vesicular nuclei [Table/Fig-6a-d]. The final diagnosis was follicular ameloblastic carcinoma.
a) CT scan depicts well defined radiolucency surrounded by sclerotic border; (b-d): 3-Dimensional CT scan depicts the extent of the lesion; e) Biopsy - gross specimen.
(a&b): Epithelial islands arranged in the form of follicles (H&E, 4x & 10x magnification); (c&d): Ameloblastic features: peripheral tall columnar cells with reverse polarization and central stellate reticulum like cells, malignant features :open faced nuclei, Increased mitotic activity, areas of haemorrhage, increased nuclear cytoplasmic ratio and binucleated cells (H&E, 20x & 40x magnification).
Discussion
Ameloblastic carcinoma is a rare malignant odontogenic tumour, which accounts for 1% of all the jaw tumours and it may arise as de-novo or from a pre-existing ameloblastoma [1]. It is generally aggressive and locally destructive in nature. It is usually an incidental finding as it mimics various odontogenic cysts and tumours. In 1972, World Health Organization (WHO) in its classification recognized malignant ameloblastoma as a malignant counterpart of benign ameloblastoma. In 1983, Shafer introduced the term "Ameloblastic Carcinoma" [2]. According to WHO 2005 classification, carcinomas derived from ameloblastomas are designated as: 1) Metastazing malignant ameloblastoma; 2) Ameloblastic carcinoma (a) Primary, (b) Secondary (dedifferentiated) intraosseous, (c) Secondary (dedifferentiated) extraosseous. Malignant ameloblastoma histologically shows the features of benign ameloblastoma, but it metastasizes to the other sites such as lung. Ameloblastic carcinoma will have the features of cytological atypia along with the histological features of benign ameloblastoma in the primary tumour, irrespective of the presence or absence of metastases [2].
Central (intraosseous) ameloblastic carcinoma has a wide age range of occurrence and the mean age of occurrence is the third decade with a slight male predilection [3]. It occurs most commonly in mandible than in maxilla, especially in the posterior region. It may be associated with rapid growth, pain, swelling, trismus, dysphonia and expansion of the jaws. Clinical presentation may vary from a cystic lesion to a large asymmetric mass with indurated ulcers, destruction of underlying bone and mobile teeth [4]. Perforation of cortical plate and extension into the surrounding soft tissue, multiple recurrent lesions and metastasis to the lymphnodes are commonly associated with this tumour [5].
Peripheral Ameloblastic Carcinoma (PAC) is defined as an extraosseous ameloblastoma with histological evidence of malignant transformation. It arises from the extraosseous remnants of dental lamina or basal cells of oral epithelium. It usually grows in the soft tissues overlying the posterior portion of mandible and presents clinically as a sessile or pedunculated mass of gingiva with smooth or irregular papillomatous surface, of approximately 1–2 centimeters in size. Histologically, both central and peripheral ameloblastic carcinoma shows the features of cytological atypia such as high mitotic index, necrosis, neural and vascular invasion, squamous metaplasia and keratin pearl formation along with the features of benign ameloblastoma such as follicular pattern with peripheral palisading ameloblasts [6]. The chances of recurrence are high, and it might be due to the surgical mismanagement of the lesion rather than any inherent malignant properties. Differential diagnosis includes acanthomatous ameloblastoma, kerato-ameloblastoma, primary intra-alveolar epidermoid carcinoma, squamous cell carcinoma arising in the lining of an odontogenic cyst, squamous odontogenic tumour, basaloid squamous cell carcinoma [7].
Wide local excision with 2-3 centimeters of wide margins is the treatment of choice with selective regional lymph node dissection and close post-operative periodic follow-up. There are no definitive recommendations regarding radiotherapy and chemotherapy reported in literature [8]. BRAFV600E mutation can be used as a potential diagnostic marker in the work-up of odontogenic tumours and it is specific for ameloblastic tumours [9].
Conclusion
In the present case series the age range was observed between 16-33 years; mean age of occurrence was 30-50 years. Peripheral ameloblastoma/peripheral ameloblastic carcinoma is a rare variant, in the present case; it was seen in a 16-year-old, which could raise a few doubts on the environment/any genetic mutation/the cause, which has to be verified. It is one of the first few case reports in which the two variants have been described and reported from the same geographical location.
[1]. Prashad KV, Ramesh V, Balamurali PD, Premalatha B, Ameloblastic Carcinoma. A case report highlighting its variations in histologyJ Int Oral Health 2011 3(6):37-42. [Google Scholar]
[2]. Lu SY, Huang SC, Huang Huang CH, Huang CC, Recurrent peripheral ameloblastic carcinoma with lung metastases case reportJ Dent Sci 2006 1(3):140-45. [Google Scholar]
[3]. Kumaran SP, Anuradha V, Gokula Krishnan S, Thambiah L, Ameloblastic carcinoma: A case seriesJ Pharm Bioall Sci 2014 6(1):208-11. [Google Scholar]
[4]. Kar IB, Subramanyam RV, Mishra N, Singh AK, Ameloblastic carcinoma: Report of two casesAnn Maxillo fac Surg 2014 4(1):70-77. [Google Scholar]
[5]. Kishore M, Panat SR, Aggarwal A, Upadhyay N, Agarwal N, Ameloblastic carcinoma: A case reportJ Clin Diagn Res 2015 9(7):ZD27-ZD28. [Google Scholar]
[6]. Ramesh M, Sekar B, Murali S, Mathew S, Chacko J, Paul G, Ameloblastic carcinoma – review and histopathology of 5 casesOral and Maxillofacial Pathology Journal 2011 2(2):154-60. [Google Scholar]
[7]. Kallianpur S, Jadwani S, Misra B, Sudheendra US, Ameloblastic carcinoma of the mandible: Report of a case and reviewJ Oral Maxillo Fac Patho 2014 18(S1):96-102. [Google Scholar]
[8]. Reddy SV, Maheshwar G, Reddy K, Reddy A, Ameloblastic carcinoma presenting clinically and histologically as plexiform ameloblastoma – A rare and interesting case report and reviewIndian Journal of Medical Case Reports 2013 2(3):60-63. [Google Scholar]
[9]. Brown NA, Betz BL, Ameloblastoma: A review of recent molecular pathogenetic discoveriesBiomark Cancer 2015 7(S2):19-24. [Google Scholar]