Breast Cancer with Synchronous Renal Cell Carcinoma: A Rare Presentation
Ravi Arjunan1, Durgesh Kumar2, K V Veerendra Kumar3, C S Premlatha4
1 Associate Professor, Department of Surgical Oncology, Kidwai Memlorial Institute of Oncology, Bangalore, Karnataka, India.
2 Senior Resident, Department of Surgical Oncology, Kidwai Memlorial Institute of Oncology, Bangalore, Karnataka, India.
3 Professor, Department of Surgical Oncology, Kidwai Memlorial Institute of Oncology, Bangalore, Karnataka, India.
4 Associate Professor, Department of Pathology, Kidwai Memlorial Institute of Oncology, Bangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Durgesh Kumar, Room no 102, Married Doctors Accomadation, Shanthidhama First Floor, Kidwai Memlorial Institute of Oncology, Bangalore-560029, Karnataka, India.
E-mail: dr.durgesh06@gmail.com
Primary cancer arising from multiple organs is a well known fact. Synchronous tumours have been most commonly associated with kidney cancer. Bladder, prostate, colorectal and lung cancer are the most common synchronous primaries with Renal Cell Carcinoma (RCC) identified till date. We found metachronous tumours of breast with RCC in literature search which included both metastatic tumours as well second primaries. Overall, 25 cases of metastatic breast tumours and eight cases of second primary in previously treated RCC have been reported in the literature. Here, we are reporting a case of synchronous presentation of carcinoma breast with RCC which is very rare because most of the multiple malignancies reported in the literature are metastatic tumours or metachronous breast malignancy with RCC.
Dual malignancy, Metachronous cancer, Metastasis, Synchronous cancer
Case Report
A 45-year-old female patient presented to Department of Surgical Oncology with chief complaints of pain abdomen and loss of appetite for last six months which was relieved on oral analgesics. There is no relevant past or family history. Clinically per abdomen and pelvic examination was normal. During general examination we found 2x2 cm mobile, hard lymph node in right axilla and the ipsilateral breast showed 8x6cm mobile lump in upper outer quadrant. Contra lateral breast and axilla were normal. Considering this as a carcinoma right breast stage III A, further routine and metastatic workup in the form of ultrasound abdomen and pelvis, X-ray of chest and bone scan as per our institute protocol was done.
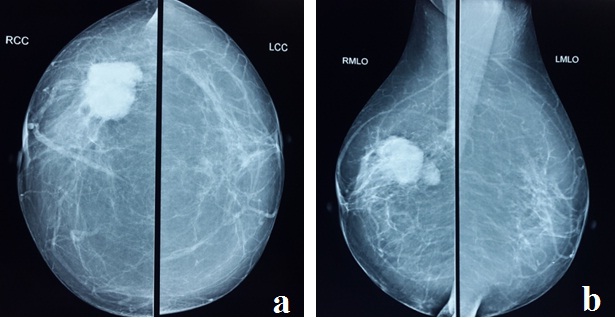
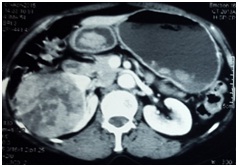
Mammogram showed nodular, irregular, homogenous density with tail like extension of size 2.9 cm x 2.8 cm, with a satellite lesion in the right axillary tail of size 1.6 cm x 1.3 cm, highly suggestive of malignancy, (BIRADS V category; [Table/Fig-1a&b]). Multiple axillary nodes were present with largest size of 1.2 cm x 0.8 cm. FNAC from breast mass was suggestive of ductal carcinoma. FNAC of axilla is not required and indicated only if no lump is palpable clinically to rule out metastasis. Preoperative staging of axilla was clinical. Ultrasound abdomen showed a mass in upper pole of the right kidney. Other metastatic work up in the form of X-ray chest, bone scan and routine haematological tests were within normal limit. In order to evaluate the renal mass contrast enhanced computed tomography scan of abdomen was done, which showed heterogeneously enhancing mass lesion in upper and mid pole of the right kidney abutting the liver and ascending colon with focal loss of fat planes, renal vein and IVC was normal [Table/Fig-2]. Preoperative FNAC of renal mass was done as per the institute protocol because of very low sensitivity and diagnostic yield. On the basis of all available clinical and pathological details, we considered this as a case of synchronous malignancy of breast stage III A and kidney.
(a) Cranio - caudal view. (b) Mediolateral view.
Mammogram showing nodular irregular homogenous density present in upper outer quadrant of right breast (BIRADS V – highly suggestive of malignancy).
Computed tomography scan showing heterogeneously enhancing mass lesion in upper and middle pole of the right kidney.
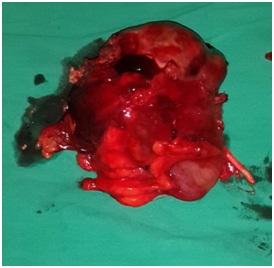
Right modified radical mastectomy [Table/Fig-3] with right radical nephrectomy [Table/Fig-4] was performed in single setting after informed consent and proper counseling of the patient about the nature of the disease. Intraoperatively, right kidney mass of size approximately 6.5 cm x 4 cm was found with maintained fat planes with colon, IVC, and liver. No enlarged nodes seen. She withstood the procedure well with uneventful postoperative period.
Right modified radical mastectomy specimen with axilllary nodes.

Right nephrectomy specimen.
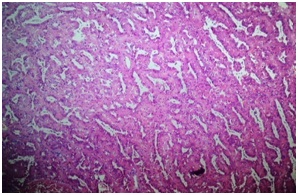
Final histopathology report of kidney showed features of papillary Renal Cell Carcinoma (RCC) with aggregates of foamy macrophages, Fuhrman nuclear grade III. Capsule was intact with tumour free margins [Table/Fig-5]. Breast specimen showed grade III invasive ductal carcinoma (no special type) with tumour free margins [Table/Fig-6], Seven out of 12 right axilllary lymph nodes showed metastatic deposits from ductal carcinoma of right breast. Hormonal receptor analysis showed estrogen receptor positivity in breast specimen but not in kidney specimen which ruled out the chances of metastasis to the kidney or vice-versa [Table/Fig-7]. So, with this histopathological result along with the other clinical and radiological parameters, we made a final diagnosis of carcinoma right breast pT2N2Mx (stage III a) with synchronous renal cell carcinoma pT1N0M0 (stage I). She was further planned for adriyamycin, cyclophosphamide and 5 -fluorouracil based adjuvant chemotherapy for the breast cancer with regular 3 monthly follow-up.
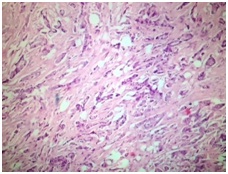
Kidney specimen showing papillary renal cell carcinoma (haematoxylin and eosin staining, x100 magnification).
Histopathology slide with showing ductal carcinoma (haematoxylin and eosin staining, x100 magnification).
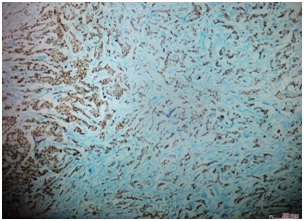
Histopathology slide with immunoperoxidase stain showing ductal carcinoma with estrogen receptor positivity (100x magnification).
Discussion
The aetiology of multiple primary malignant tumours is complex, and it includes not only environmental factors like tobacco, occupation, pollution, and ultraviolet light but also genetic predisposition and medical treatment in form of radiotherapy or chemotherapy, gender-specific factors, hormonal factors, and interactions of these factors with host environment [1]. Other primary may not be symptomatic and detected in routine metastatic work up of the patient. When another primary malignancy is detected in the same patient or within 6 month of the diagnosis of primary cancer is known as synchronous cancer. Association of breast cancer synchronous renal cell cancer is very rare and very few cases have been reported [2].
Synchronous malignancies are defined as malignant tumours that presents simultaneously or within six months of the diagnosis of the primary tumour. According to the literature, prevalence of multiple primary malignancies is about 4.5-11.7% [3]. To label a case of dual malignancy as synchronous following criteria must be fulfilled: 1) Both the tumour must be pathologically distinct from each other; 2) There should be definite features of malignancy; and 3) the possibility metastasis must be ruled out [4,5]. In our case, estrogen receptor analysis was done to rule out the metastasis from breast to kidney after final histopathology report of RCC by immunohistochemical analysis. Aetiology of synchronous malignancies is multiple. Depending of the aetiology these factors are divided in to three groups: 1) Treatment related example – second malignancy after chemotherapy or radiation; 2) Related to genetic mutations; and, 3) Due to common environmental factors [1].
In a population based study done by Jiao F et al., eight cases of synchronous breast primaries with RCC was reported with prevalence of 13.1% [2], which was less than the previous studies i.e., 26% which was reported by Christian B et al., [6]. Piccinini L in 1996 has reported 2 cases of breast primaries with synchronous RCC [7]. Metachronous tumours of breast with renal primary have been reported in literature with both metastatic as well second primaries. Christian B had reported 8 cases of carcinoma breast in RCC patients during a follow-up period of 1987-2002, in his population based study of multiple malignancies in Norway [6].
Metastasis to the breast from RCC is a rare occurrence and takes place in 3% of all metastatic RCC [8]. Overall 25 such cases have been reported in the literature: 11 cases presented with breast metastasis as the initial sign of the disease and 14 (two were bilateral) as metachronous lesions [9–14]. Recently in 2014, Falco et al., has reported a case of breast metastasis from renal primary [15]. In 2014, one more case of carcinoma breast with synchronous RCC has been reported [16].
Sato et al., reported that other primaries at the time of nephrectomy for RCC was an independent prognostic factor for overall survival after the operation. Furthermore patients with localized RCC with coexistent cancer had poorer overall survival than those with localized RCC alone [17]. Treatment of RCC in patients with multiple primary tumours should be based not only on the stage and operability of the kidney tumour, but also on an evaluation of the disease status of the other malignant disease.
Because of limited therapeutic and diagnostic option synchronous malignancies whenever found causes a lot of problems to both clinicians and patients [18].
Conclusion
The study of synchronous malignancies may provide important evidences not only for clinical evaluation and further treatments of these tumours, but also provide clues for the aetiology, pathogenesis and the future management of cancer including the development of effective screening and surveillance protocols, with the goal to treat patients effectively.
[1]. Takalkar U, Asegaonkar BN, Kodlikeri P, An elderly woman with triple primary metachronous malignancy: A case report and review of literatureInt J Surg Case Rep 2013 4:593-96. [Google Scholar]
[2]. Jiao F, Yao LJ, Zhou J, Hu H, Wang LW, Clinical features of multiple primary malignancies: a retrospective analysis of 72 Chinese patientsAsian Pac J Cancer Prev 2014 15:331-34. [Google Scholar]
[3]. Irimie A, Achimas-Cadariu P, Burz C, Puscas E, Multiple primary malignancies - epidemiological analysis at a single tertiary institutionJ Gastrointestin Liver Dis 2010 19:69-73. [Google Scholar]
[4]. Aydiner A, Karadeniz A, Uygun K, Multiple primary neoplasm at a single institution: differences between synchronous and metachronous neoplasmAm J Clin Oncol 2000 23:364-70. [Google Scholar]
[5]. Derwinger K, Gustavsson B, A study of aspects on gender and prognosis in synchronous colorectal cancerClin Med Insights Oncol 2011 5:259-64. [Google Scholar]
[6]. Christian B, Olaug T, August B, Jarle N, Multiple primary malignancies in patients with renal cell carcinoma: a national population-based cohort studyBJU International 2006 97:698-702. [Google Scholar]
[7]. Piccinini L, Luppi G, Zoboli A, Torricelli P, Occasional diagnosis of synchronous renal cell carcinoma during staging of other primary tumoursTumouri 1996 82(5):488-90. [Google Scholar]
[8]. Alzaraa A, Vodovnik A, Montgomery H, Saeed M, Sharma N, Breast metastases from a renal cell cancerWorld J Surg Oncol 2007 5:25 [Google Scholar]
[9]. Mahrous M, Al Morsy W, Al Hujaily A, Al Sulimani S, Breast metastases from renal cell carcinoma: rare initial presentation of diseases recurrence after 5 yearsJ Breast Cancer 2012 15:244-47. [Google Scholar]
[10]. Hairulfaizi H, Rohaizak M, Naqiyah I, Yahya ML, Tan GC, Zainuddin Z, Breast and axillary lymph nodes metastases five years after radical nephrectomy for renal cell carcinoma. A case report and review of literatureLib J Med 2009 4:120-22. [Google Scholar]
[11]. Bortnik S, Cohen JD, Leider-Trejo L Ron IG, Breast metastases from a renal cell carcinomaIMAJ 2008 10:736-37. [Google Scholar]
[12]. Lee WK, Cawson JN, Hill PA, Hoang J, Rouse H, Renal cell carcinoma metastases to the breast: mammographic, sonographic, CT and pathologic correlationBreast J 2007 3:308-17. [Google Scholar]
[13]. Álvarez M, García D, Tomás N, Calvo J, Breast metastases as initial presentation of renal cell carcinomaActas Urol Esp 2010 34:288-303. [Google Scholar]
[14]. Ganapathi S, Evans G, Hargest R, Bilateral breast metastases of a renal carcinoma: a case report and review of the literatureBMJ Case Rep 2008 [Google Scholar]
[15]. Falco G, Buggi F, Sanna PA, Dubini A, Folli S, Breast metastases from a Renal Cell Carcinoma. A case report and review of the literatureInt J Surg Case Rep 2014 5(4):193-95. [Google Scholar]
[16]. Kurlekar UA, Rayate AS, Synchronous primary malignancies in breast and kidney: A rare case reportIndian J Surg 2014 [Google Scholar]
[17]. Sato S, Shinohara N, Suzuki S, Harabayashi T, Koyanagi T, Multiple primary malignancies in Japanese patients with renal cell carcinomaInt J Urol 2004 11:269-75. [Google Scholar]
[18]. Jung EJ, Lee JH, Jeon K, Treatment outcomes for patients with synchronous multiple primary non-small cell lung cancerLung Cancer 2011 73:237-42. [Google Scholar]