Successful Pregnancy Outcome in a Patient with Solitary Kidney Affected by Angiomyolipoma: A Rare Case
Vineet Vashistha Mishra1, Kavita Mistry2, Sakshi Nanda3, Sumesh Choudhary4, Khushali Gandhi5
1 Head of Department and Professor, Department of Obstetrics and Gynaecology, Institute of Kidney Diseases and Research Centre, Institute of Transplantation Sciences, Ahmedabad, Gujrat, India.
2 Assistant Professor, Department of Obstetrics and Gynaecology, Institute of Kidney Diseases and Research Centre, Ahmedabad, Gujrat, India.
3 Clinical Fellow, Department of Obstetrics and Gynaecology, Institute of Kidney Diseases and Research Centre, Ahmedabad, Gujrat, India.
4 Assistant Professor, Department of Obstetrics and Gynaecology, Institute of Kidney Diseases and Research Centre, Ahmedabad, Gujrat, India.
5 Assistant Professor, Department of Obstetrics and Gynaecology, Institute of Kidney Diseases and Research Centre, Ahmedabad, Gujrat, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vineet Vashistha Mishra, Head of Department and Professor, Department of Obstetrics and Gynaecology, Room No: 31. Institute of Kidney Diseases and Research Centre, Institute of Transplantation Sciences (IKDRC - ITS), B.J. Medical College, Civil Hospital Campus, Ahmedabad – 380016, Gujrat, India.
E-mail: vineet.mishra.ikdrc@gmail.com
Renal angiomyolipoma is a rare benign tumour and its occurrence during pregnancy is even rare. It is usually diagnosed incidentally. It can increase in size during pregnancy and can present acutely as rupture with retroperitoneal haemorrhage, mechanism of which is still unclear. We present a case of successful pregnancy outcome in a patient with congenital solitary kidney affected by angiomyolipoma, diagnosed incidentally at 19 years of age. The patient had conceived twice. Her antenatal and post partum period was uneventful both the times.
Antenatal, Pregnancy, Post-partum
Case Report
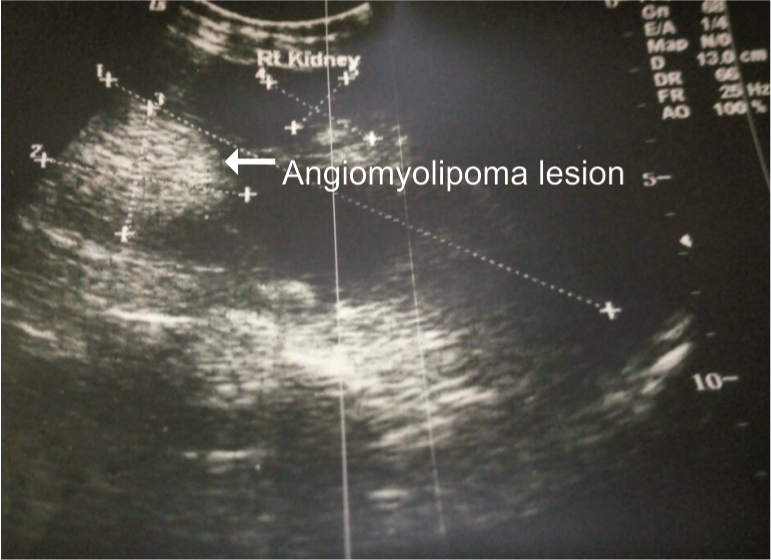
A 24-year-old second gravida female, with previous history of lower segment caesarean section for intrauterine growth retardation 2 years back, presented in OPD with two and half month of amenorrhea. She was known case of right sided congenital solitary kidney affected by angiomyolipoma, diagnosed incidentally 5 years back. Her previous postpartum period was uneventful. She had regular follow-up in Nephrology and Urology Department for renal angiomyolipoma. She was asymptomatic with haemoglobin 9.8gm%, WBC count 6300/cumm, platelet count 1,22,000/cumm, serum creatinine 0.62mg/dl, RBS 92mg/dl and normal urine routine and microscopy examination. Her obstetric ultrasound revealed single intrauterine live pregnancy with 10 weeks 3 days of gestation, with right ovary showing corpus luteal cyst and left ovary normal. Her Ultrasound Kidney Ureter Bladder (USG KUB) showed right kidney 15.1×7.3cm in size with normal echo pattern and preserved cortico-medullary differentiation [Table/Fig-1]. There was mild hydronephrosis, with multiple cysts in all poles largest measuring 4×3.2cm in size and multiple echogenic lesions of variable size largest 5.5×3.3cm. Left kidney was absent with normal urinary bladder. Patient was counselled about possible risks of spontaneous rupture of tumour leading to retroperitoneal haemorrhage, thromboembolism and possible management options in case of such emergency. But she continued her pregnancy with all due risks. Detailed anomaly scan was done and fetal 2D echo at 22 weeks of gestation were normal. She had regular antenatal follow- up monthly till 20 weeks, every fortnight till 28 weeks, thereafter weekly till term. Her serum creatinine, urinary albumin and renal ultrasonography were done twice monthly.
USG KUB showed right kidney affected by angiomyolipoma.
Elective caesarean section at 38 weeks of gestation was planned as she had previous caesarean delivery and there was a theoretical risk of rupture during intrapartum period. A healthy baby of 2.5kg was delivered. Immediate and 6 months post-partum period was uneventful.
Discussion
Renal angiomyolipoma is a benign mesothelial tumour, which consist of mature adipose tissue, blood vessels and smooth muscle cells [1]. It is most commonly found in the kidney but can occur in other organs too. The incidence of renal angiomyolipoma in the general population is 0.3% and it accounts for 3% of all solid renal masses [1]. There are two types of renal angiomyolipoma- one which can be, isolate in occurrence and others which are associated with tuberous sclerosis. Most of the time renal angiomyolipoma is asymptomatic but when it is associated with pregnancy, there is a risk of rupture.
Renal angiomyolipoma is a rare renal tumour and pregnancy with it is a rare entity. About 80% renal angiomyolipoma are solitary, with the mean age of presentation is around 43 years. It is four times more common in men and most commonly involves the right kidney [2]. In our case too patient had right solitary kidney which was affected by angiomyolipoma. About 20% cases are associated with tuberous sclerosis, an autosomal dominant disease, with mean age of presentation 20-30years [2]. In these patients lesions are multiple, bilateral, small and often complicated with haemorrhage [2]. Most of renal angiomyolipomas are asymptomatic and found incidentally on imaging. Palpable abdominal mass, haematuria or flank pain are the main symptoms. Patient may present with acute abdominal pain or even shock as a result of spontaneous rupture of this tumour.
Renal mass diagnosed in initial ultrasound examination, MRI should be performed, as it is safe for both mother and fetus. MRI can provide clinical information on local spread of tumour, nodal and venous involvement [3]. As our patient was already a diagnosed case, we followed her up with periodic ultrasound.
These tumours have tendency to grow during pregnancy because muscle cells of this tumour contains oestrogen and progesterone receptors, also due to increase in circulating blood volume and renal blood flow [4]. Patients during pregnancy are always at risk of tumour rupture. Hence, these patients, need to be closely monitored during antenatal period.
The management of renal angiomyolipoma is widely discussed. Asymptomatic tumours < 4cm should be managed conservatively, with regular ultrasound or CT-scan every 6 monthly [5]. Symptomatic, bilateral lesions should be treated with selective arterial embolization or partial nephrectomy [6]. An ideal time for surgical management, if required is during second trimester of pregnancy [7]. The average gestation period when renal angiomyolipoma can rupture is around 26-28 weeks [8]. If tumour ruptures before 32 weeks and patient is haemodynamically stable, then patient can be managed conservatively. Radical nephrectomy is required when the patient is haemodynamicaly unstable, due to retroperitoneal haemorrhage. However, treatment for each patient should be individualized [8].
Although there is a theoretical risk of fatal bleeding due to variation in blood pressure during labour and valsalva maneuvers, but there are no evidences to prove a higher incidence of bleeding during a vaginal delivery as compared to caesarean section [7]. Renal angiomyolipoma, itself has no effect on fetal well-being except in emergency cases of rupture of tumour with haemodynamic instability [8].
There are 26 cases of angiomyolipoma during pregnancy are reported out of which 21(81%) had rupture of tumour and 4(15%) were uneventful during pregnancy [9]. In our case, patient had good pregnancy outcome even in presence of solitary kidney with renal angiomyolipoma.
Conclusion
Patients whenever incidentally diagnosed with renal angiomyolipoma, need to be counseled about complications and management options during pregnancy. Renal angiomyolipoma as such does not have any adverse effect on fetus, but mother may have to undergo intervention due to its complications. They can have good pregnancy outcome by closely monitoring them. They require multidisciplinary team approach to have successful pregnancy outcome.
[1]. Steiner MS, Goldman SM, Fishman EK, Marshall FF, The natural history of renal angiomyolipomaJ Urol 1993 150:1782-86. [Google Scholar]
[2]. Rakowski SK, Winterkorn EB, Paul E, Steele DJ, Halpern EF, Thiele EA, Renal manifestations of tuberous sclerosis complex: Incidence, prognosis, and predictive factorsKidney Int 2006 70:1777-82. [Google Scholar]
[3]. Putra LGJ, Minor TX, Bolton DM, Appu S, Dowling CR, Neerhut GJ, Improved assessment of renal lesions in pregnancy with magnetic resonance imagingUrology 2009 74:535-39. [Google Scholar]
[4]. Morales JP, Georganas M, Khan MS, Dasgupta P, Reidy JF, Embolization of a bleeding renal angiomyolipoma in pregnancy: case report and reviewCardiovasc Intervent Raqdiol 2005 28:265-68. [Google Scholar]
[5]. Tanaka M, Kyo S, Inoue M, Kojima T, Conservative management and vaginal delivery following ruptured renal angiomyolipomaObstet Gynecol 2001 98:932-33. [Google Scholar]
[6]. Oesterling JE, Fishman EK, Goldman SM, Marshall FF, The management of renal angiomyolipomaJ Urol 1986 135:1121-24. [Google Scholar]
[7]. Molina Tl, Montes JM, Cecilia EC, Muñiz MM, González AG, Martínez MAH, Angiomiolipomas, esclerosis tuberosa y gestación: casoclínicoGinecol Obstet Mex 2009 77(8):380-86. [Google Scholar]
[8]. Zapardiel I, Delafuente-Valero J, Manuel Bajo-Arenas J, Renal angiomyolipoma during pregnancy: review of the literatureGynecol Obstet Invest 2011 72:217-19. [Google Scholar]
[9]. Çetin C, Büyükkurt S, Demir C, Evrüke C, Renal angiomyolipoma during pregnancy: Case report and literature reviewJ Turk Soc Obstet Gynecol 2015 2:118-21. [Google Scholar]