Modified Distal Shoe Appliance for Multiple Loss of First and Second Primary Molars
Yogesh Indrajit Somwanshi1, Amar Narayan Katre2, Ashwin Murlidhar Jawdekar3
1 Senior Lecturer, Department of Paediatric and Preventive Dentistry, MIDSR Dental College, Latur, Maharastra, India.
2 Professor, Department of Paediatric and Preventive Dentistry, YMT Dental College Kharghar, Navi Mumbai, Maharastra, India.
3 Professor and Head, Department of Paediatric and Preventive Dentistry, YMT Dental College Kharghar, Navi Mumbai, Maharastra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Yogesh Indrajit Somwanshi, C/O C-10 Yashwant Housing Society, B.N. Pai Marg/Nagar, Ghatkopar (E), Mumbai-400077 Maharastra, India.
E-mail: yogesh.somwanshi9@gmail.com
Multiple deciduous molars, Permanent first molar, Premature loss, Space maintainer
A 4.5-year-old boy reported to the Department of Pedodontics and Preventive Dentistry complaining of pain and recurrent swelling in lower right back region of the jaw since five days. The patient was well oriented and did not have any contributory medical history. No abnormality was detected in the general and extra-oral examinations. Intra-oral examination revealed that both the mandibular first and second primary molars on the right side (FDI teeth No. 84,85) and the mandibular second primary molar on the left side (FDI tooth No. 75) had deep carious lesions and were judged to be non-restorable. The teeth were tender to palpation. The mandibular first primary molar on the left side (FDI tooth No. 74) had a multi-surface carious lesion not involving the pulp [Table/Fig-1]. The gingival tissue surrounding the first and second primary molars on the right side (FDI teeth No. 84,85) was inflamed and the buccal vestibule slightly obliterated. Radiographic examination revealed a radiolucency involving the furcation of both the mandibular first and second primary molars of the right side (84,85) and the mandibular second primary molar of the left side (75) along with external root resorption. A multi-surface carious lesion, not approaching pulp, was seen on mandibular left primary first molar (74). The mandibular first permanent molars on both sides showed Nolla’s Stage V of tooth development [Table/Fig-2]. In addition, smooth surface caries were seen on upper and lower anteriors. Based on clinical and radiographic examination a diagnosis of apical periodontitis was made and extraction of mandibular left second molar (75) and mandibular right first and second molar (84,85) followed by fabrication of a space maintainer was planned. Parental consent for the same was taken. Study models were obtained and a space analysis (using Huckaba’s method) revealed approximately 2mm of space available per side. The mandibular left primary first molar (74) was restored using a pre-formed stainless steel crown. A 125X0.04mm band was adapted around the mandibular right primary canine. Impressions were made in alginate and models obtained along with the crown and the band on the respective teeth. A 1mm (19 G) Hard Round Stainless Steel (HRSS) wire was used for fabrication of the appliance. The extension of the horizontal and vertical arms was determined using radiographs (after adjusting for the radiographic error). A vertical slit of the desired depth was made on the model and the wire was adapted accordingly. Following adaptation, the wire was soldered to the crown and the band respectively. The mandibular molars indicated for extraction were extracted under local anaesthesia and the appliance was seated in place. Radiographs were taken to check the horizontal and vertical extension of the appliance [Table/Fig-3] and the appliance was then cemented using Type I Glass Ionomer Cement on the same appointment following haemostasis [Table/Fig-4]. The patient was recalled after three days to assess wound repair and stability of appliance. Subsequently the patient was placed on a monthly recall. The recall after 10 months showed erupted permanent first molars [Table/Fig-5,6]; the space maintainer was well accepted by the child and we were satisfied and optimistic about the future of his dentition. This appliance would be eventually replaced with a bilateral fixed space maintainer like lingual arch following complete eruption of the permanent first molars and incisors.
Pre-operative photograph (indirect vision) showing grossly carious non-restorable deciduous mandibular molars (75, 84 and 85).

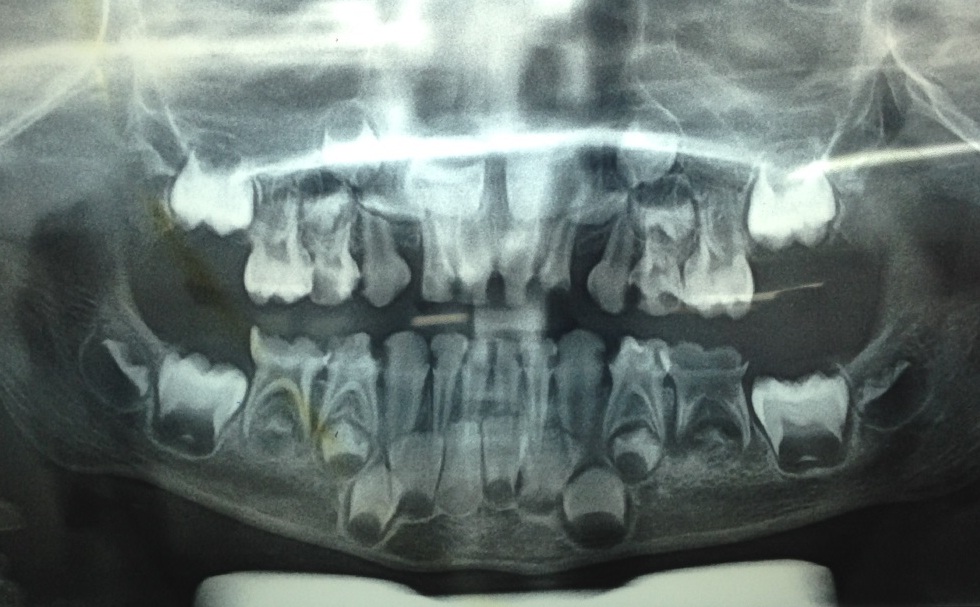
Pre-operative OPG showing grossly destructed 75, 84 and 85 and multisurface caries on 74.
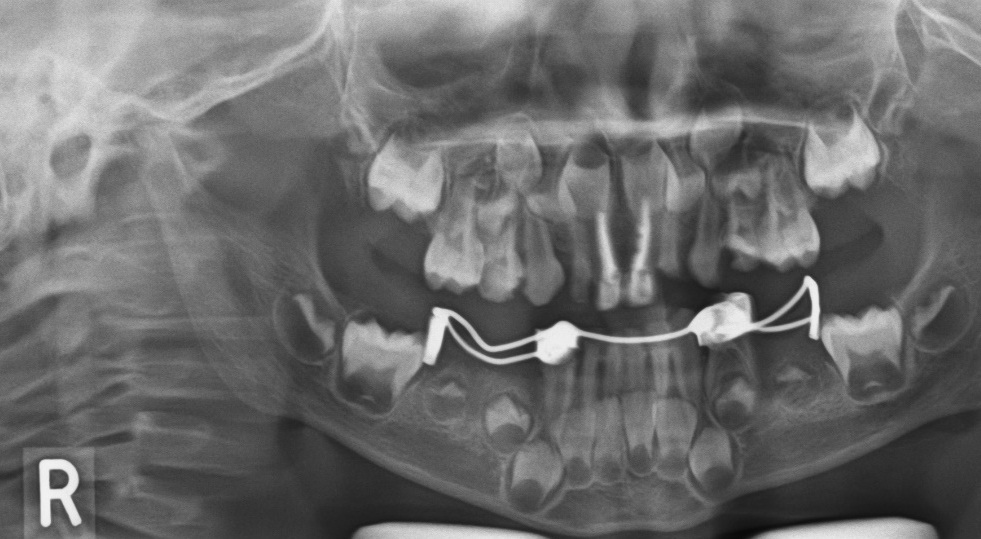
OPG for assessment of appliance adaptation before final cementation.
Post-operative (indirect vision) photograph after cementation of the appliance.

Photograph (indirect vision) of the modified distal shoe appliance after eruption of permanent first molar (10 months after placement).

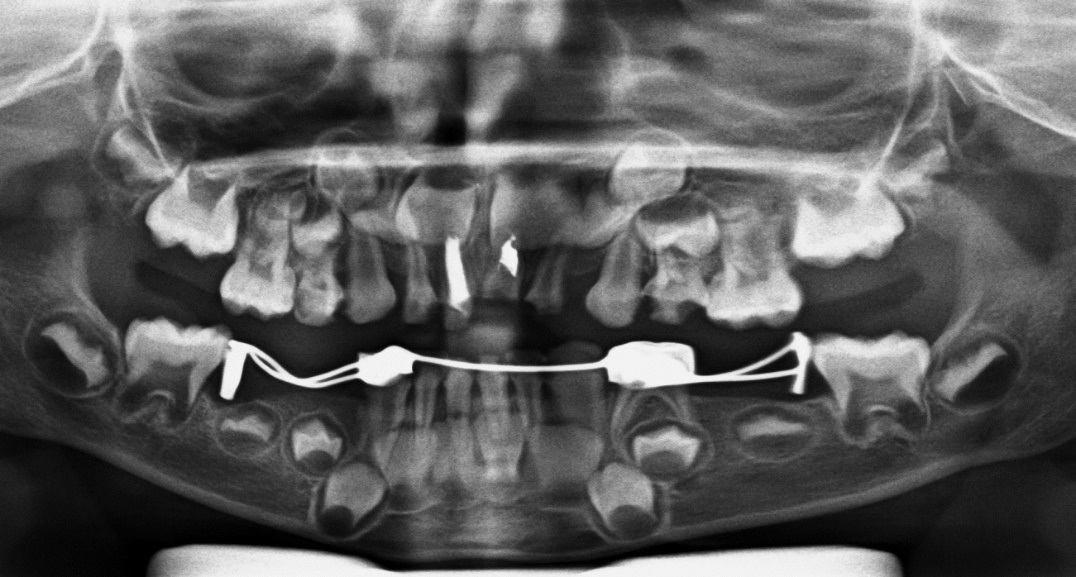
OPG for assessment of appliance after eruption of permanent molar.
Discussion
The mixed dentition period is the most important phase in the development of a normal physiological occlusion in a child. Premature loss of primary teeth without appropriate corrective measures being taken for space maintenance is one of the major factors leading to malocclusion. In such cases, use of a space maintainer is indicated after radiographic and clinical confirmation on the necessity of the same. The type of space maintainer to be used will depend on the number of teeth lost, the location of the teeth lost, overall health status of the individual, caries risk etc. An ideal space maintainer should present the following qualities [1] –
Maintain the desired mesiodistal dimension of the space
Provide mesiodistal space opening when it is required
Maintain individual functional movement of teeth
Should be hygienic
Have good durability
Have low cost
At the same time, the protocol for the management of dental caries cannot be overlooked [2]. In addition, it has been stated that endodontic treatment is not the ultimate remedy for teeth, especially in those that cannot be restored to function [3], as in the current reported case, wherein a history of chronic inflammation coupled with a non-restorable (following caries removal) 84 was best treated with extraction and suitable space maintenance. Similar treatment strategies have also been adopted in the literature wherein restoration of function has been given its due importance [4,5].
The tooth which is erupting adjacent to an edentulous area has a greater potential for space loss than fully erupted ones, indicating that clinical intervention should be considered [6]. Traditionally, the distal shoe space maintainer remains an acceptable standard of care in case of premature loss of primary second molars prior to eruption of the first permanent molars [7]. The subgingival extension serves as a guide for the erupting first molar, and prevents mesial “drifting” of that tooth [8].
In certain clinical situations, the conventional designs may have to be modified to meet patients’ needs. The conventional design of the distal shoe may not be effective wherein there is a loss of both the primary mandibular molars, unilaterally or bilaterally. Stability of the appliance would have been a major issue in this case, if we had given distal shoe space maintainer separately on both sides. Croll suggested the use of modifications like prefabricated lingual arch wire embedded in acrylic [9] and Gegenheimer proposed the use of an acrylic pressure ridge [10]. However, poor retention and patient compliance was a major drawback with these appliance designs [10]. Earlier for getting more stability banding on canine on one side and other on second primary molar on another side has been used by Bhatt PK in case of multiple loss of primary molars on one side [11]. A similar design as used in this case has been given previously by Dhindsa et al., wherein the primary canine and the first molar were only banded [12]. However, in our case, the mandibular primary left first molar had multi-surface caries and hence, was restored with a preformed steel crown. The appliance has inherent limitations in the design as it is non-functional, fabrication has to be precise and it cannot be given in medically compromised and uncooperative patients. Also, it being a bilateral appliance, it may interfere with the eruption of the permanent mandibular incisors [9]. Thus, this appliance needs to be monitored regularly for the eruption of permanent mandibular incisors, both radiographically and clinically.
To conclude, this modified bilateral distal shoe appliance should be used judiciously for those cases where there is a premature loss of multiple primary molars prior to the eruption of the first permanent molars. However, further clinical studies are needed to establish its feasibility and usefulness in paediatric dentistry.
[1]. Ak G, Sepet E, Pinar A, Aren G, Turan N, Reasons for early loss of primary molars. Oral healthPrev Dent 2005 3:113-17. [Google Scholar]
[2]. White BA, Maupome G, Clinical decision-making for dental caries managementJ Dent Ed 2001 65(10):1121-25. [Google Scholar]
[3]. Anusavice K, Management of dental caries as a chronic infectious diseaseJ Dent Ed 1998 62(10):791-802. [Google Scholar]
[4]. Downer MC, Azli NA, Bedi R, Moles DR, Setchell DJ, How long do routine dental restorations last? A systematic reviewBrit Dent J 1999 187(8):432-39. [Google Scholar]
[5]. Hickel R, Kaaden C, Paschos E, Buerkle V, García-Godoy F, Manhart J, Longevity of occlusally-stressed restorations in posterior primary teethAm J Dent 2005 18:198-211. [Google Scholar]
[6]. Dhull K S, Bhojraj N, Yadav S, Prabhakaran SD, Modified distal shoe appliance for loss of primary second molar: A case reportQuint Int 2011 42(10):829-33. [Google Scholar]
[7]. Willet RC, Preventive orthodonticsJ Am Dent Assoc 1936 23:2257-70. [Google Scholar]
[8]. Gegenheimer R, Donly KJ, Distal shoe: A cost-effective maintainer for primary second molarsPaediatr Dent 1992 14:268-69. [Google Scholar]
[9]. Croll TP, Johnson R, The stainless steel crown welded sheet and wire loop for posterior space maintaincePed Dent 1980 2:56-58. [Google Scholar]
[10]. Gegenheimer Donly KJ, Distal shoe: A cost-effective maintainer for primary molarsPed Dent 1992 14:268-69. [Google Scholar]
[11]. Bhatt PK, Navin HK, Idris M, Christopher P, Rai N, Modified distal shoe appliance for premature loss of multiple deciduous molars: A case reportJ Clin Diagn Res 2014 8(8):ZD43-45. [Google Scholar]
[12]. Dhindsa A, Pandit IK, Modified Willet’s appliance for bilateral loss of multiple deciduous molars: A case reportJ Ind Soc Pedod Prev Dent 2008 26(3):132-35. [Google Scholar]