The dental arch perimeter and transpalatal width are the most significant arch dimensions in the developing individuals. Its management during the primary, mixed and early permanent dentition are greatly important for the normal development of the dental arches and significantly improve the occlusion in adulthood. Malocclusion is a constant source of threat to the facial appearance. Severe anterior crowding and narrow maxillary arches adversely affect the smile, facial profile and consequently patient becomes handicapped socially as well as psychologically. Maxillary expansion has been used in resolving the problems of crowding, constricted arches and allow for forward growth of the mandible in growing children. This case report describes the use of a customized modified Haas appliance in intercepting the maxillary anterior crowding and gain the transpalatal width and arch perimeter of the maxilla, enhance the smile and facial profile and to allow the forward mandibular growth without any anterior occlusal interferences.
Arch perimeter, Crowding, Expansion screw, Mandibular growth, Transpalatal width
Case Report
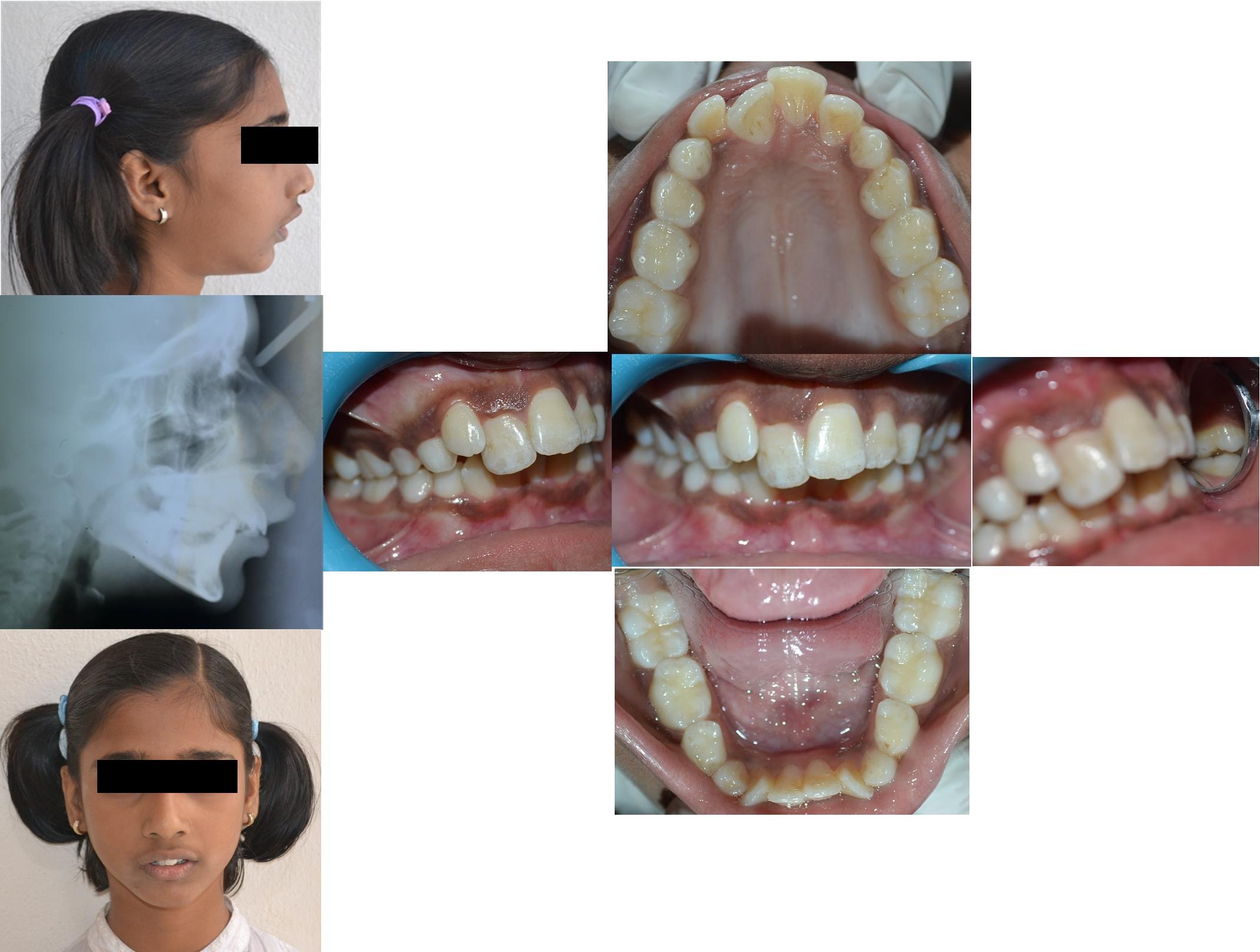
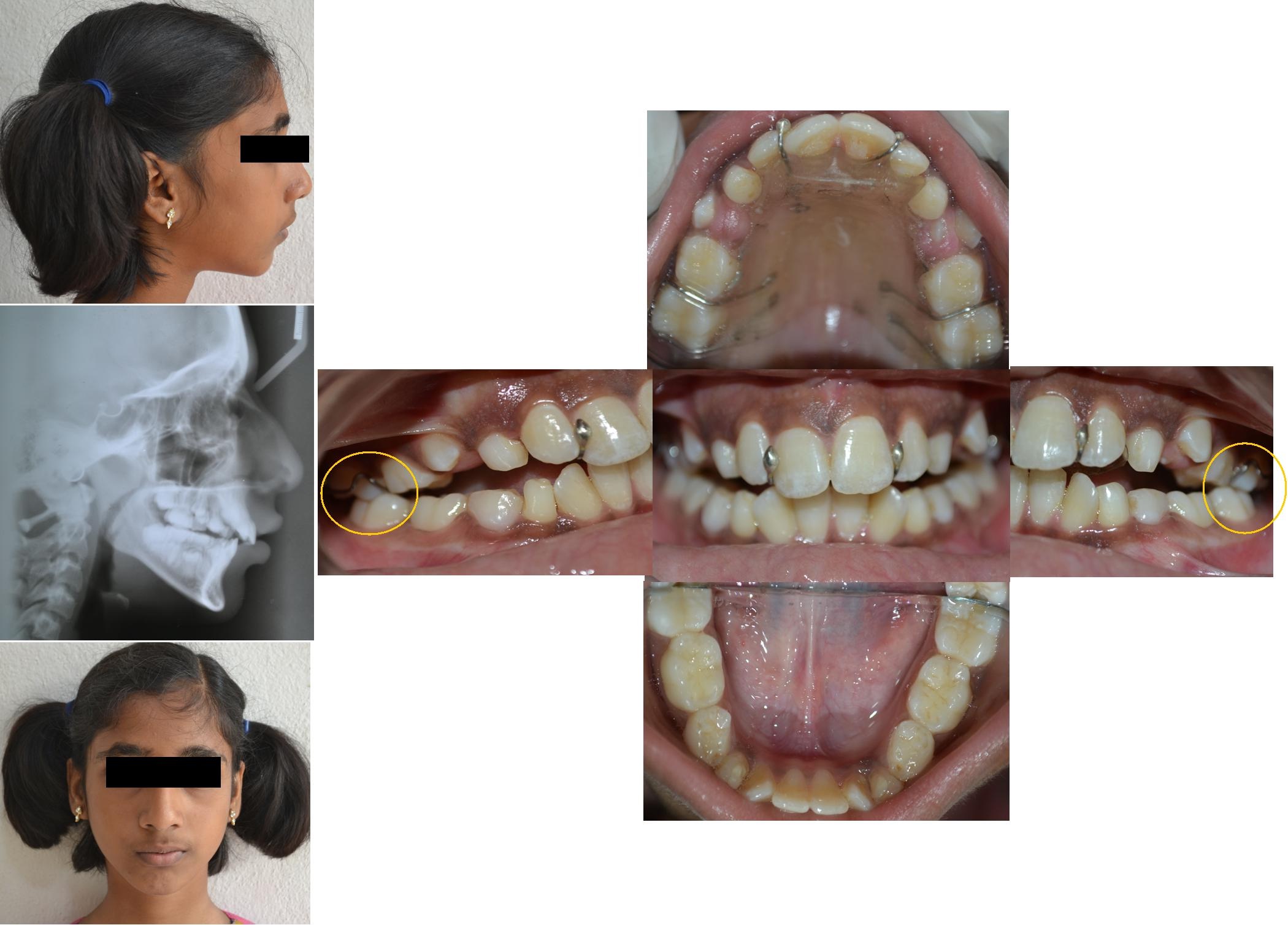
A 10-year-old female patient accompanied by her mother reported to the Department of Pedodontics and Preventive Dentistry with the chief complaint of unaesthetic appearance and irregularly placed upper front teeth. Clinical examination revealed the following features: Convex facial profile, incompetent lips and lower lip trap. On intra-oral examination, she presented a mixed dentition stage, labially placed 12, 21, disto-palatal rotation of 11, mesio-labial rotation of 32, 42, V-shaped maxillary arch. The patient exhibited an increased overbite, overjet, midline shift towards the patients right side and end on molar relationship on both sides [Table/Fig-1]. The patient’s medical and family history was non-contributory.
Pre-treatment extra and intra-oral photographs.
Tanaka Jonson Model analysis was performed as it is a non radiographic method and used patient’s models, in which 6mm arch discrepancy was observed. Pre-expansion measurements of arch perimeter, inter canine, inter molar and arch width were traced on the working cast [Table/Fig-2]. Pre-expansion measurements were recorded [Table/Fig-3].
Pre-expansion measurements traced on the cast.
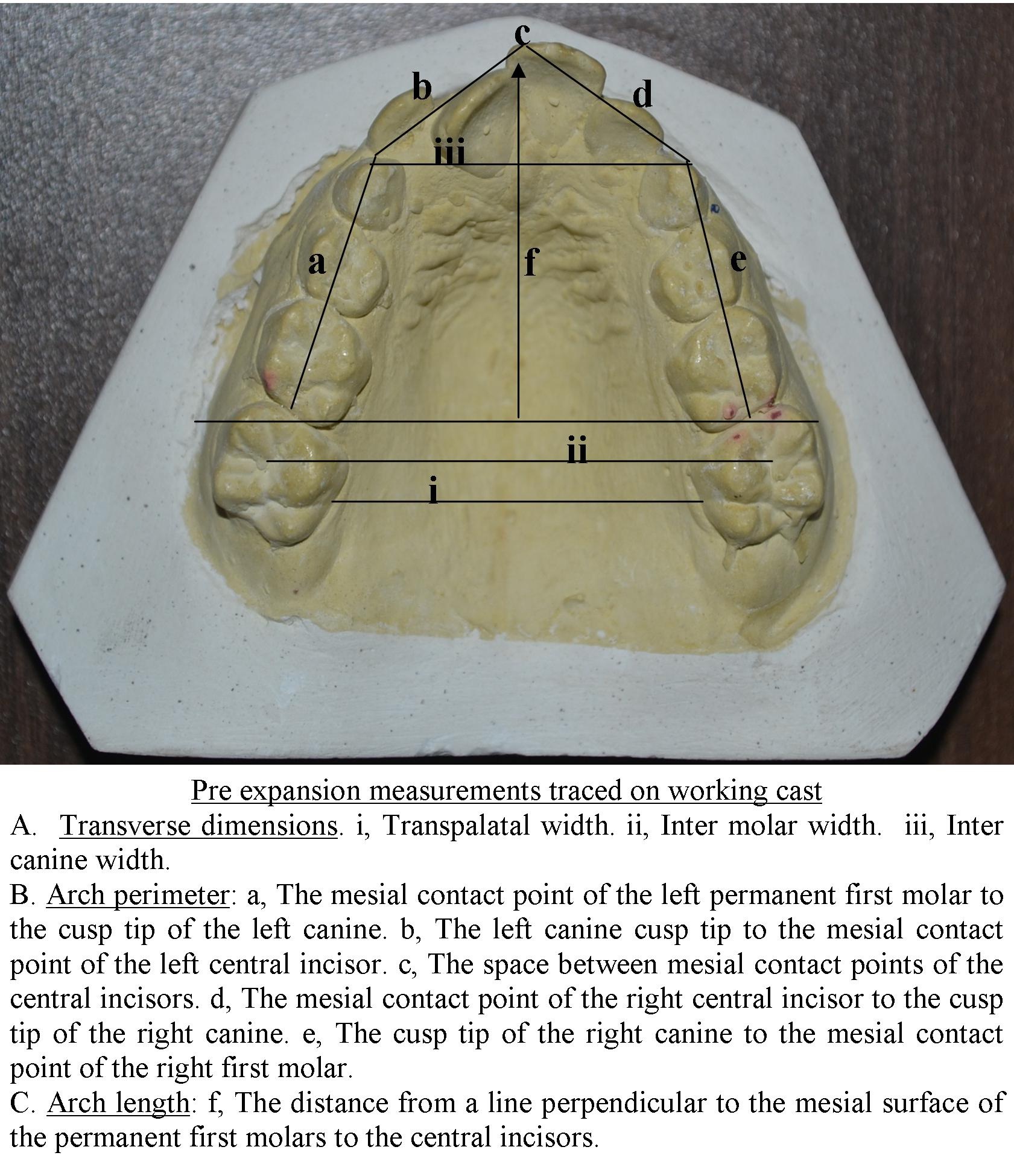
Pre-expansion measurements.
| S. No | Parameter | Pre-expansion |
|---|
| 1 | A) Transverse dimensions | Inter-canine width | 20mm |
| Inter-molar width | 29mm |
| Transpalatal width | 28mm |
| 2 | A) Arch perimeter | 78mm |
| 3 | B) Arch length | 29mm |
| 4 | Tanaka Johnston Model analysis | a) Prediction space: 84b) Available space: 78c) 6mm discrepancy |
Pre-expansion soft tissue and hard tissue cephalometric analysis were performed on the lateral cephalogram and measurements were recorded [Table/Fig-4].
Pre-expansion cephalogram measurements.
| S. No. | Parameter | Pre-treatment | Average values |
|---|
| 1 | <SNA | 81° | 80°- 82° |
| 2 | <SNB | 74° | 80° |
| 3 | ANB | 6° | 2° |
| 4 | Facial angle | 80° | 82-95° |
| 5 | Mandibular plane angle | 35° | 17-28° |
| 6 | Occlusal plane angle | 15° | 14° |
| 7 | Upper incisor to N-A Angle | 22° | 22° |
| 8 | Upper incisor to N-A linear | 5mm | 4mm |
| 9 | Lower incisor to N-B angle | 25° | 25° |
| 10 | Lower incisor to N-B linear | 3mm | 4mm |
| 11 | Inter-incisor angle | 127° | 130° -131° |
| Soft tissue analysis |
| 1 | Naso-labial angle | 70° | (102°±8°) |
| 2 | Cant upper lip | 18° | (14°±8°) |
| 3 | Steiner’s S-Line | Convex | |
On the basis of model analysis and radiographic findings, the diagnosis was confirmed as skeletal Class II with a deficiency in mandibular growth, arch perimeter and transpalatal width. Informed consent was taken from the parent’s prior to treatment. The case was undertaken for maxillary expansion for space gaining with customized modified Haas appliance.
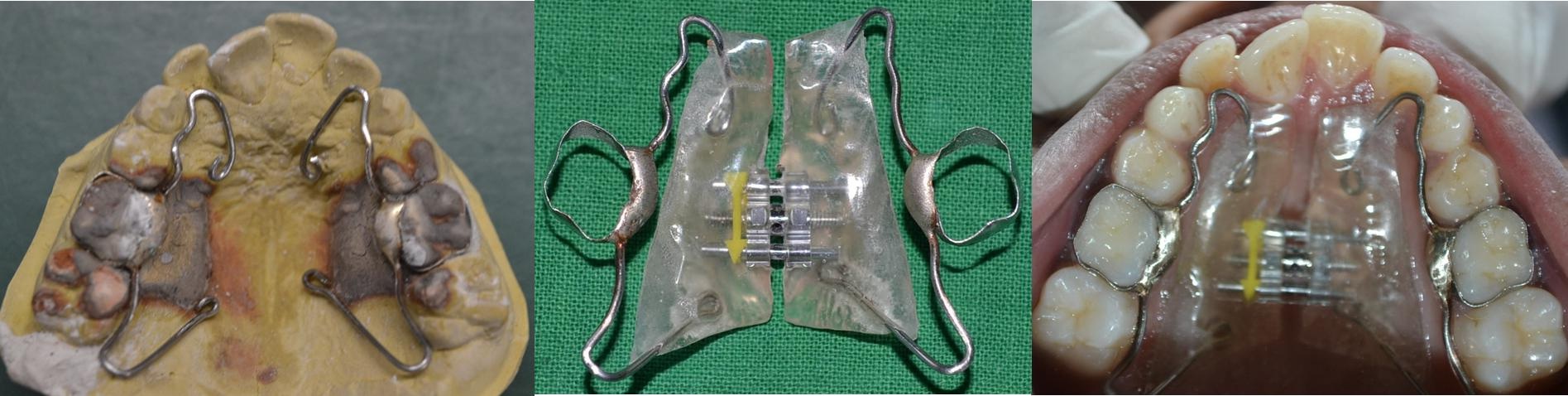
Appliance Design [1]: Molar separation was achieved with orthodontic separators (3M). Bands were selected according to the mesiodistal measurement of 55, 65 and placement was done. An alginate impression was made, bands were transferred in the alginate impression and the working cast was prepared. A 20 gauge (0.08 inch, Konark, India) stainless steel orthodontic wire was adapted on the palatal aspect of 16, 55, 54, 53 and contra lateral 26, 65, 64, and 63. The wire component was soldered to the molar bands on the palatal surface of 55, 65. A jack screw was placed in the center of the hard palate and the free ends of wire components were stabilized in the self-cure acrylic resin [Table/Fig-5].
Clinical Management: Prior to cementation, the appliance was tried intraorally for optimal fit. In the first week following the insertion of the appliance, it was not activated thereby allowing the child to adapt to the appliance. On the subsequent recall visits, initially the jack screw was activated two quarter turns in a day (90°) for first week and subsequently activated one quarter turn in a day for six weeks [2,3]. The same appliance was used for retention and the patient was scheduled for the next appointment. After four months retention, the appliance was removed and the removable retainer was placed. The patient was asked to visit every 1, 3, 6, 12, 18 months for follow-up. After one and a half year follow-up the patient had an acceptable facial profile and aesthetics. The end on molar relation came into Class I molar relation on both sides and the lips were competent. Post-expansion measurements of arch perimeter, inter-canine, inter-molar and arch width were traced on the cast [Table/Fig-6]. Pre-expansion measurements were recorded [Table/Fig-7]. Soft and hard tissue cephalometric analysis was done [Table/Fig-8]. Post-treatment intra-oral photograph is shown in [Table/Fig-9].
Post-expansion measurements traced on the cast.
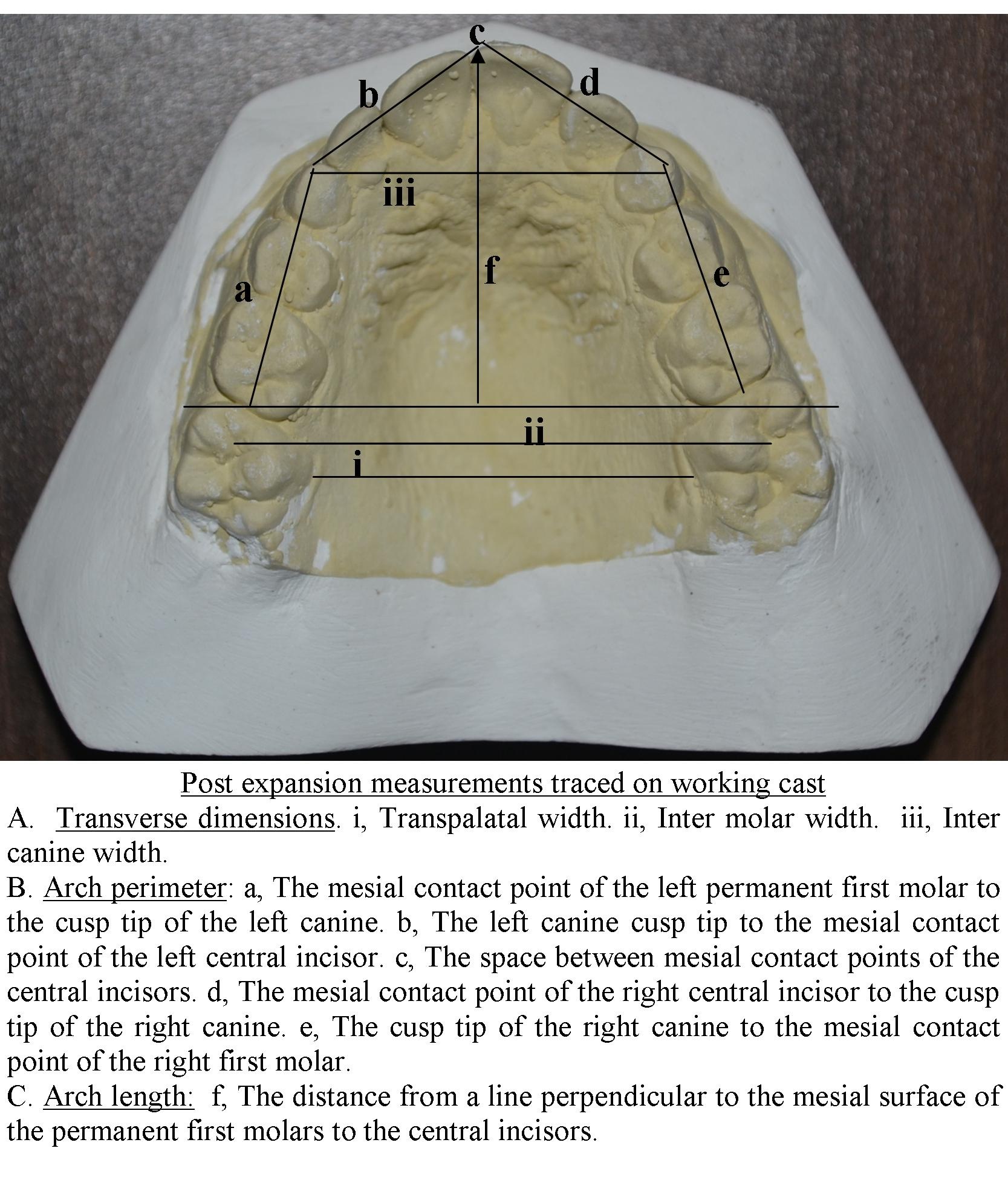
Post-expansion measurements.
| S. No | Parameter | Pre-expansion |
|---|
| 1 | A) Transverse dimensions | Inter-canine width | 25mm |
| Inter-molar width | 33mm |
| Transpalatal width | 32mm |
| 2 | A) Arch perimeter | 85mm |
| 3 | B) Arch length | 31mm |
| 4 | Tanaka Johnston Model analysis | d) Prediction space: 84e) Available space: 85f) 1mm more space available |
Post-expansion cephalogram measurements.
| S No | Parameter | Post-expansion |
|---|
| 1 | <SNA | 82° |
| 2 | <SNB | 78° |
| 3 | ANB | 4° |
| 4 | Facial angle | 83° |
| 5 | Mandibular plane angle | 38° |
| 6 | Occlusal plane angle | 17° |
| 7 | Upper incisor to N-A angle | 23° |
| 8 | Upper incisor to N-A linear | 5 mm |
| 9 | Lower incisor to N-B angle | 25° |
| 10 | Lower incisor to N-B linear | 5 mm |
| 11 | Lower incisor to N-Pog linear | 3 mm |
| 12 | Inter-incisor angle | 126° |
| Soft tissue analysis |
| 1 | Naso-labial angle | 110° |
| 2 | Cant upper lip | 16° |
| 3 | Steiner’s S-Line | Straight |
Post-expansion extra and intra oral photographs.
Discussion
The interceptive orthodontic treatment has a vital role in the treatment of developing malocclusion. The treatment of developing malocclusion has to be ideally understood as early intervention, using easy, minimal duration and able to completely or moderately correcting a malocclusion or preventing it from becoming worse [4]. Early treatment involves correction of anterior crossbite, crowding, and ectopic eruption of anterior teeth. Problems associated with dental arches are the lack of space, space loss, malposition and malalignment of teeth. All such problems could be treated with space gaining and simultaneous alignment of the teeth [5].
The removable jack screw appliance can serve this purpose in early mixed dentition when the midpalatal suture is less tortuous and their added advantage is the simple laboratory procedure and cost effectiveness. However, their main problem with the use of the removable appliance is noncompliance on the part of the patient as most of the patients fail to wear them regularly. There are many advantages of fixed appliances over the removable appliances including reduced need for patient cooperation and lesser discomfort [6]. Many fixed appliances have been described to resolve the problems associated with transverse discrepancy [2]. The rapid maxillary expansion appliance is one of the most efficient to treat transverse discrepancy. Usually, rapid maxillary expansion appliance anchored premolars and permanent molars, and the expansion causes a buccal tipping of these teeth [7]. Anchoring teeth may exhibit exostosis, pulp stones, root resorption and clinical evidence of periodontal damage to the anchoring teeth has been reported, with on the occurrence of gingival recession three times more than in control [8,9]. To avoid these undesirable effects on permanent teeth, rapid maxillary expansion in mixed dentition can be achieved by using primary teeth to anchor the appliance [10]. Various studies reported the advantage of primary teeth to be used as anchor for the palatal expansion appliance; it avoids the undesirable effects on permanent teeth [11–14].
The following case report describes the use of a customized modified Haas appliance in intercepting the maxillary anterior crowding, gain the arch perimeter, transpalatal width, and enhance the smile and facial profile and to allow the mandibular growth without any anterior occlusal interferences.
Reichenbach and Taatz used the example of a foot and shoe principle, with the foot representing the mandible and the shoe representing the maxilla. If the shoe is too narrow, it is impossible for the foot to slide fully into the shoe. By widening the shoe, the foot slides forward into its usual position. From an orthopedic standpoint, the widening of the maxilla allows for the spontaneous repositioning of the mandibular jaw into a more forward position [15]. Kingsley emphasizes this phenomenon, how the palatal expansion could favor mandibular advancement [16]. This example, allows to understand how the transpalatal expansion solves spontaneous mandible repositioning in a forward position, solving or improving sagittal malocclusion [17].
In the present case, we have adapted this concept, correcting the maxillary occlusal problem allows for the spontaneous repositioning of the mandible into a more forward position. In patients with a Class II malocclusion and a reduced transpalatal width, i.e., <31mm it is recommended to widen the maxilla using maxillary expansion [15]. The patient monitored on a regular basis. In the present case, we observed the transpalatal width less i.e., 28mm, this was one of the reasons for early intervention. Evidence suggests that rapid maxillary expansion has been shown to have additional benefits including facilitation of correction of Class II and Class III malocclusion spontaneously. A spontaneous correction of the Class II malocclusion sometimes occurs in the early mixed dentition, during the retention period [18]. Comparison of different palatal expansion appliances is shown in [Table/Fig-10].
Comparison of different palatal expansion appliances.
| Hyrax appliance | Haas appliance | Customized modified Haas appliance |
|---|
| Anchorage | Permanent teeth
| Permanent teeth
| Primary teeth, permanent teeth Advantages of the use of the primary teeth to anchor the appliance: It avoids the undesirable effects on permanent teeth
|
| Type | Tooth borne | Tooth and tissue borne | Tooth and tissue borne |
| Advantages | Hygienic appliance
| More efficiently counteract the centripetal forces present during the retention phase. Maintaining basal expansion
| The appliance has more stability Least expansive (Jack screw) Least side effects on anchoring teeth Easy to fabricate More efficiently counteract the centripetal forces present during the retention phase. Maintaining basal expansion
|
| Disadvantages | Expansive Expansion causes a buccal tipping of anchoring teeth Root resorption, periodontal damage
| Expansive Expansion causes a buccal tipping of anchoring teeth Root resorption, periodontal damage
| Further clinical research is required
|
In the present case it was observed, that after subsequent appointments the patient displayed a Class I molar relation and the shift in molar relation occurred before the transition from the mandibular second primary molar to the second premolar, this was presumable. The mandibular growth subsequently makes this early postural change stable. Anterior occlusal interferences should be intervened at an earlier stage for proper development of maxillary and mandibular jaws, and for the establishment of the class I molar relationship.
Conclusion
The customized modified Haas appliance is effective to treat transpalatal discrepancies and anterior maxillary crowding in the mixed dentition using primary second molars as an anchorage and this appliance being cost effective and easy to fabricate, could be used as a substitute for Hyrax or Haas expanders in mixed dentition. Proper diagnosis, timely intervention is important for such mixed dentition occlusal problems. Further clinical research is required with a larger sample to assess the success of the appliance.
[1]. Kennedy D B, Osepchook M, Unilateral posterior crossbite with mandibular shift: A reviewJ Can Dent Assoc 2005 71(8):569-73. [Google Scholar]
[2]. Sylvia Ng, Minjie Li, Yanqi Yang, Orthopedic treatment of maxillary expansion: A review of the literatureInt J Dentistry Oral Sci 2015 2(1):39-41. [Google Scholar]
[3]. Romanyk D L, Lagravere M O, Toogood R W, Major P W, Carey J P, Review of maxillary expansion appliance activation methods: engineering and clinical perspectivesJ Dent Biomech 2010 2010:1-7. [Google Scholar]
[4]. Ghafari J, Early treatment of dental arch problemsQuintessence Int 1986 17(7):423-32. [Google Scholar]
[5]. Mutinelli S, Cozzani M, Arch dimension with anchorage on deciduous teethEur J Paediatr Dent 2015 16(2):115-22. [Google Scholar]
[6]. Mohammad Z, Cheruku S R, Penmetcha S, Bagalkotkar A, Kumari S, A novel approach to regain anterior space using modified 2 by 3 fixed appliance: A report of two casesJ Clin Diagn Res 2015 9(10):23-25. [Google Scholar]
[7]. Haas AJ, Palatal expansion: Just the beginning of dentofacial orthopedicsAm J Orthod 1970 57:219-55. [Google Scholar]
[8]. Cozzani M, Guiducci A, Mirenghi S, Mutinelli S, Siciliani G, Arch width changes with a rapid maxillary expansion appliance anchored to the primary teethAngle Orthod 2007 77(2):296-02. [Google Scholar]
[9]. Mutinelli S, Manfredi M, Guiducci A, Denotti G, Cozzani M, Anchorage onto deciduous teeth: Effectiveness of early rapid maxillary expansion in increasing dental arch dimension and improving anterior crowdingProg Orthod 2015 16(22):2-7. [Google Scholar]
[10]. Barber AF, Simms MR, Rapid maxillary expansion and external root resorption in man: A scanning electron microscope studyAm J Orthod 1981 79:630-52. [Google Scholar]
[11]. Vanarsdall RL, Periodontal/orthodontic interrelationships. In: Graber TM, Swain BF, edsOrthodontics, Current Principles and Techniques 1994 St Louis, MoMosby:715-21. [Google Scholar]
[12]. Vardimon AD, Graber TM, Voss LR, Lenke J, Determinants controlling iatrogenic external root resorption and repair during and after palatal expansionAngle Orthod 1991 61:113-22. [Google Scholar]
[13]. Cozzani M, Rosa M, Cozzani P, Siciliani G, Primary dentition- anchored rapid maxillary expansion in crossbite and non-crossbite mixed dentition patients: Reaction of the permanent first molarProg Orthod 2003 4:15-22. [Google Scholar]
[14]. Sari Z, Uysal T, Usumez S, Basciftci FA, Rapid maxillary expansion. Is it better in the mixed or in the permanent dentition?Angle Orthod 2003 73:654-61. [Google Scholar]
[15]. McNamara JA Jr, Treatment of tooth size/arch size discrepancy problemsOrthodontic and Orthopedic treatment in the mixed dentition 1993 United States of AmericaNeedham Press:67-93. [Google Scholar]
[16]. Maspero C, Galbiati G, Giannini L, Farronato G, Sagittal and vertical effects of transverse sagittal maxillary expander (TSME) in the three different malocclusion groupsProg Orthod 2015 16(6):1-9. [Google Scholar]
[17]. Bishar SE, Hoppens BJ, Jakobsen JR, Kohout FJ, Changes in molar relationship between the deciduous and permanent dentition: A longitudinal studyAm J Orthod DO 1988 93:19-28. [Google Scholar]
[18]. McNamara JA, Early intervention in the transverse dimension: Is it worth the effort?Am J Orthod DO 2002 121(6):572-74. [Google Scholar]