Oral cancer is an important cancer globally with incidence of over 3, 00,000 cases per year [1]. It is amenable to primary as well as secondary prevention. In India cancer registries have confirmed a high incidence of oral cancer. Case-control and cohort studies have established that the high incidence is due to widespread habits of tobacco chewing and smoking [1].
Pathological changes accompanying oral cancer can be observed by the patients themselves. Symptoms arise in organs responsible for day to day functions viz. speech, swallowing, eating and respiration. The disease itself along with the treatment leads to aesthetic damage and loss of function [2].
Patients are under great stress due to fear of death, treatment course and its side effects, social, family and economical constraints. Various studies have been done to evaluate the psychological problems faced by these patients during the treatment period [2–4]. The aim of our study was to assess the quality of life of oral cancer patients, during the pre-operative period. In our region, convincing cancer patients for treatment is a big challenge as mostly the patients are uneducated, superstitious and belong to low socioeconomic status. Majority of them believe that cancer is untreatable, few who believe in treatment expect high functional and aesthetic outcome, which can’t be promised. Considering the above factors pre-operative period was selected as this will help the treating doctors to understand and interpret the psychological needs of such patients thereby providing them with the much needed emotional support.
Materials and Methods
A total of 206 patients scheduled to undergo treatment for oral cancer; aged above 18 years and who could be interviewed were selected from various cancer centres in South India. Patients undergoing treatment for mental disorder or those who had a previous history of mental disorder were excluded from the study. Out of 206, 171 patients gave informed consent after knowing the purpose of the study. These 171 patients were analysed during the study period i.e. March 2013 to March 2016.
This study was carried out with the approval of Institutional Board of Ethics, Ultra’s Best Dental Science College, Madurai, Tamil Nadu, India. Interviews were conducted after explaining the purpose of the study to the patients and obtaining their written consent. We conducted the following surveys at 1-7 days before surgery (pre-operative): (1) FACT-G version 4; and (2) (FACT-H&N, as a quality of life (QOL) survey [2]. All the assessments were translated in Tamil. Medical information, population data, and statistical data were obtained from the patients’ medical records.
Questionnaires: The psychological needs of oral cancer patients are complex and require a multi-dimensional evaluation [3]. So, we selected the FACT-G questionnaire to evaluate general QOL, and the FACT-H&N questionnaire to evaluate the aspects of QOL specific to pre-operative patients with Head and Neck cancer.
1. FACT-G, version 4: The FACT-G is a self administered questionnaire used to assess QOL, comprising of a total of 29 items as follows: 7 physical-related items (Physical Well-Being; PWB), 7 society- and family-related items (Social/Family Well-Being; SWB), 6 psychology related items (Emotional Well-Being: EWB), and 7 function-related items (Functional Well-Being; FWB). Each item is rated on a scale of 0-4, where higher scores indicate higher QOL [2].
2. FACT-H&N, version 4: The FACT-H&N consists of additional 11 items over FACT-G. These 11 items are related to aspects of QOL specific to patients of Head and Neck cancer such as eating, swallowing, speech and aesthetics [2].
Statistical Analysis
Statistical analysis was done using Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, version 22.0 for Windows). Using this software, range, frequencies and percentages were calculated for qualitative variables. Means and standard deviations were calculated for quantitative variables. Student’s t-test and ANOVA were used to test the significance of difference between “well-being scores” and demographic variables. The relationship of well being scores with the age and sex has also been studied.
The grading system used to assess the qualitative scores of well-being is given in [Table/Fig-1].
The following grading system was used to assess the qualitative scores of well-being.
| Variable | Physical well-being | Social/Familywell-being | Emotionalwell-being | Functionalwell-being |
|---|
| Total questions | 7 | 7 | 6 | 7 |
| Minimum total score | 0 | 0 | 0 | 0 |
| Maximum total score | 28 | 28 | 24 | 28 |
| Scoring Grade |
| Good | 0 - 7 | 0 - 7 | 0 - 6 | 0 – 7 |
| Satisfactory | 8 – 14 | 8 - 14 | 7 – 12 | 8 – 14 |
| Poor | 15 - 21 | 15 - 21 | 13 - 18 | 15 -21 |
| Very Poor | >21 | < 21 | < 18 | < 21 |
Results
The demographics of the subjects were as follows. Participants consisted of 122 men and 49 women, with mean age of 50.2±10.4 (age range: 31-78) [Table/Fig-2]. More than half of the subjects had received post-secondary education. Cancer on the tongue was the most common (102 cases), followed by the mandibular alveolus (31 cases), buccal mucosa (23 cases) and retromolar trigone (15 cases).
Characteristics of studied cases.
| Variable | Unit | Value |
|---|
| Cases studied | Number | 171 (100%) |
| Sex | Male | 122 (71.3%) |
| Female | 49 (28.7%) |
| Age Group | 31- 40 yrs | 41 (24% |
| 41- 50 yrs | 50 (29.2%) |
| 51 – 60 yrs | 51 (29.8%) |
| < 60 yrs. | 29(17.0) |
| Age (years) | Range | 30 -69 yrs |
| Mean | 50.2 yrs |
| S.D. | 10.4 yrs |
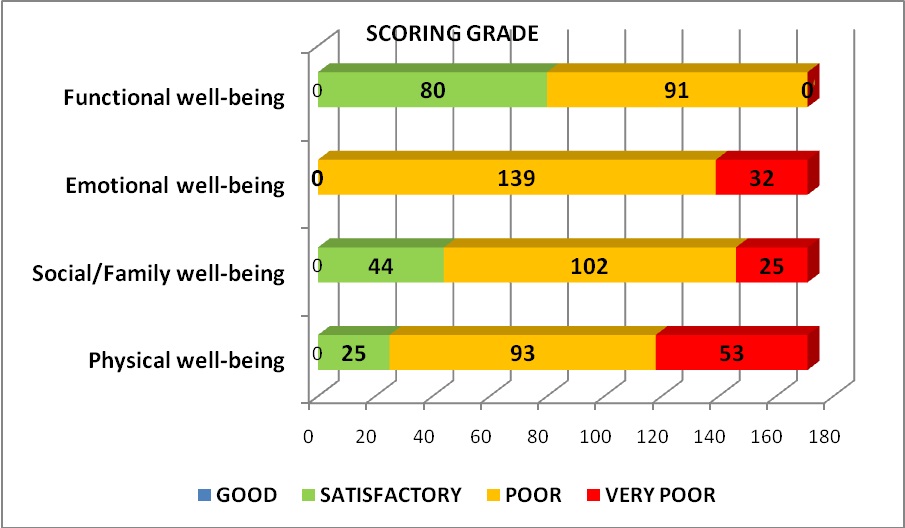
With regard to the clinical (TNM staging), histological and radiographic evaluation, it was observed that 132 cases were in the early stages (Stage 1 and 2) and 39 cases (Stage 3 and 4) were in the advanced stages. Physical, social, family, emotional and functional well-being grades were calculated and tabulated [Table/Fig-3].
Physical, social, family, emotional and functional well-being grades.
Association between well-being scores and age was calculated and displayed in [Table/Fig-4]. The relationship between age and physical, social and functional well being showed a statistical significance, while there was no statistical significance in emotional well being between different age groups.
Association between well-being scores and age.
| Age Group | Scoring Grade regarding |
|---|
| Physicalwell-being | Social/Familywell-being | Emotionalwell-being | Functionalwell-being |
|---|
| Mean | S.D. | Mean | S.D. | Mean | S.D. | Mean | S.D. |
|---|
| 31 – 40 yrs | 18.3 | 3.1 | 18.3 | 3.0 | 17.6 | 2.6 | 13.1 | 2.9 |
| 41 – 50 yrs | 19.0 | 2.9 | 16.6 | 2.9 | 16.4 | 2.4 | 14.3 | 2.7 |
| 51 – 60 yrs | 20.2 | 2.4 | 16.2 | 2.5 | 17.1 | 2.3 | 14.7 | 3.0 |
| >60 yrs | 21.8 | 0.8 | 16.0 | 2.7 | 16.9 | 1.0 | 17.2 | 2.0 |
| ‘p’ | < 0.0001Significant | 0.0012Significant | 0.0958Not Significant | < 0.0001Significant |
Association between well-being scores and sex has been calculated and shown in [Table/Fig-5]. There was no statistical significant difference in all the parameters between different age groups.
Association between well-being scores and sex.
| Sex | Scoring Grade regarding |
|---|
| Physicalwell-being | Social/Familywell-being | Emotionalwell-being | Functionalwell-being |
|---|
| No. | % | No. | % | No. | % | No. | % |
|---|
| Male | 19.5 | 2.9 | 16.8 | 2.9 | 16.9 | 2.3 | 14.6 | 3.0 |
| Female | 20.0 | 2.6 | 16.7 | 2.9 | 17.1 | 2.3 | 14.7 | 3.2 |
| ‘p’ | 0.3171Not significant | 0.7082Not significant | 0.7016Not significant | 0.8586Not significant |
Discussion
Various studies have been done earlier to evaluate the psychological changes associated with oral cancer patients during peri-operative period [2,5,6]. Both the disease and adverse reactions during treatment of cancer are emotionally, psychologically and functionally challenging to the patients [2,3]. All the above mentioned studies prove that the quality of life definitely affects oral cancer patients.
We conducted FACT-G and FACT-H&N, as a quality of life (QOL) survey. All the assessments were translated in Tamil. The data showed that males were affected more than the female patients. It shows the association of tobacco use with oral cancer incidence. In our study it was found that cancer incidence in South Indian males is mostly due to tobacco smoking while in females it is due to arecanut chewing. In few cases the cause of cancer could be traced to the presence of fractured sharp tooth or overextended dentures (dentures made by quacks).
Even though patients were diagnosed during their middle age (31-41 years), most of them seek treatment only during later years (41-61 years), which negatively affects the prognosis and survival rates.
FACT-H&N scores showed that most of the patients were experiencing poor or very poor quality of life and only few had given satisfactory grade. Most of the people gave poor scores for emotional well being. Pre-operatively most of the patients had satisfactory oral functions like eating talking etc., and none reported poor functional well being.
Correlation between the age and quality of life scores showed that there were significant differences between the age groups. The younger patients had a good quality of life scores when compared to the older ones, while all the age groups were equally affected emotionally due to the poor emotional backup from the society and family. There was no difference in well being scores between males and females.
Limitation
The limitation of our study is that it’s done only in pre-operative period. Further elaborate studies should be done to evaluate the psychological changes associated during and after treatment period, with various treatment modalities such as surgery, radiation or chemotheraphy to understand the effect of these treatments in quality of life in these patients. Further studies can be conducted on patient’s spouses or caretakers whose psychological status is also an important factor during treatment period.
Conclusion
From the above study it is clear that, oral cancer patients of all age groups and of both the sexes are affected emotionally; hence, psychological counselling for the patients and family members should be a part of the comprehensive treatment plan. The cancer centre should have an in house psychiatrist or clinical psychologist to manage emotional instabilities in these patients. Meeting the psychological needs of these patients will help them undergo the treatment with confidence and follow the protocols meticulously, which will definitely increase the treatment outcomes and prognosis.