Introduction
Recurrent Aphthous Stomatitis (RAS) is a condition in which ulcers repeatedly occur in the oral cavity [1]. Aphthous ulcers arise in the oral cavity at least four times a year [2]. It is prevalent in developed countries, occurring in all ages, geographic regions and races [1,3]. About 80% of people have one episode of oral aphthous ulcers before the age of 30 years [1]. Often related to systemic diseases like Behçet’s Disease (BD) and Crohn’s disease, it considerably affects the quality of life of a person [4].
Etiopathogenesis: The etiology of RAS remains unclear [1]. A genetic predisposition has been suggested, as evidenced by the presence of certain types of Human Leucocyte Antigens (HLA) in some patients [5]. Predisposing factors like trauma, deficiency of B-complex vitamins and folate, microbial factors, stress, hormonal changes and immunologic factors may contribute to the formation of ulcers [6,7].
A cell-mediated immune response mechanism has been proposed in the immunopathogenesis of RAS [1]. Trigger factors may initiate the cascade of pro-inflammatory cytokines against the oral mucosa resulting in activation of T-lymphocytes and leukocyte chemotaxis [8]. Type 1 T-helper cells produce cytokines (interferon-alpha (INF-α), interleukin-2, interleukin-12 and tumor necrosis factor-alpha) which are responsible for the immune response seen in RAS. TNF-α is responsible for the appearance of new lesions in RAS [1,9]. Presence of auto-antibodies against the oral mucosal membrane has also been suggested in the pathogenesis of RAS [9].
Clinical Features: RAS presents as painful, shallow, round ulcers which have a pseudomembranous center surrounded by an erythematous margin. A burning sensation is present for about 2 to 48 hours before the appearance of the ulcer [6]. Intense pain is present at the ulcer site and as healing occurs, the pain gradually recedes [1]. Most ulcers occur on the non-keratinizing epithelial surface of the mouth like the buccal and labial mucosa and the tongue. The three forms of RAS are minor, major and herpetiform RAS [1,6].
In Dental and Oral Medicine literature, RAS is used to refer to a dominant condition where the ulceration is not associated with a systemic disease like BD. However, in General Medical literature, the oral ulceration described in BD is indistinguishable from those in RAS. Therefore, it remains elusive whether a similar pathogenesis exists between the ulceration seen in RAS associated with systemic diseases and RAS unassociated with other diseases [10]. It was observed that the oral ulceration occurring in BD resembles those seen in RAS and that BD and RAS share many clinical and immunological characteristics. A study done by Ozyurt K et al., found that the serum interferon gamma, alpha-enolase levels, interleukin-1, interleukin-13, interleukin-18 were higher in patients with BD as well as RAS when compared to healthy controls [10,11]. For the purpose of this review, we have considered studies where recurrent oral ulceration was present in patients, regardless of whether the ulcers were associated with systemic diseases or not.
Diagnosis
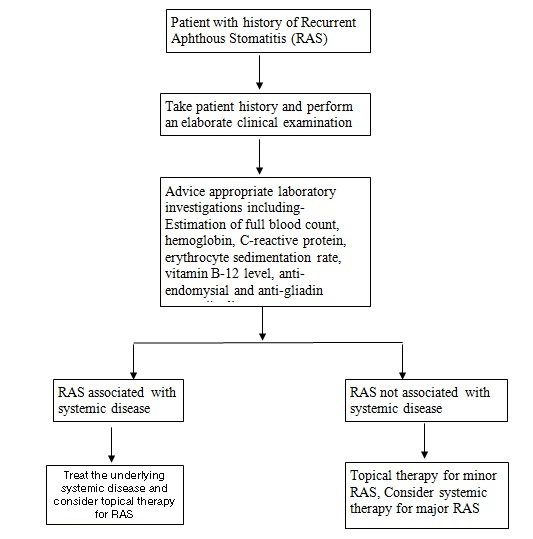
RAS is diagnosed on the grounds of patient history and exami-nation of ulcers. A positive family history, associated medical conditions, medications, occurrence of similar lesions in past, duration and frequency of ulcers may be suggestive of RAS and an inspection of the site, size, number, shape, edge and base of ulcers will help in the clinical diagnosis. There is no definite diagnostic test available for RAS and a biopsy is not warranted in most cases. Estimation of full blood count, hemoglobin, C-reactive protein, erythrocyte sedimentation rate, vitamin B12 level, anti-endomysial and anti-gliadin autoantibodies may provide a clue about the cause of RAS [1,12]. [Table/Fig-1] provides an algorithm for the diagnosis of RAS.
Algorithm for the diagnosis of RAS.
Management
The fundamental goals of treatment are to shorten the duration of ulcer, provide relief from pain, and increase disease-free periods while the secondary goals would be to lessen the frequency and severity of recurrences [12,13]. The same treatment regimen cannot be used in all patients as certain drugs appear to be effective in some, while others might have limited responses [1].
Topical therapy may be sufficient for occasional episodes of minor ulcers while systemic interventions are used in patients who are unresponsive to topical agents or have severe disease [1,6,12]. Various treatment modalities that are available for the treatment of RAS have been enlisted in [Table/Fig-2] [3,14–32].
Treatment modalities commonly used for RAS.
| DRUG | DOSE | BENEFIT | SIDE EFFECTS |
|---|
| TOPICAL TREATMENTS |
| Chlorhexidine [14] | 0.2% mouth rinse; 1% gel | Reduction in frequency, duration and severity of ulcers | Bitter taste, brown staining of tongue and teeth [3] |
| Minocycline 0.2% in aqueous solution [15] | Rinse mouth with 5ml of solution, four times a day | Reduction in severity and duration of pain | No side effects [15] |
| Dexamethasone ointment (5-gram tube) [16] | Apply three times a day after meals on ulcer for 5 days | Reduction in pain and quicker healing | Oral pseudomembranous candidiasis [3] |
| Amlexanox 2mg adhesive pellicles or 5% paste [17,18] | Four times a day for each aphthous ulcer for 5 days | Reduction in pain and size of ulcers | No side effects [18] |
| TOPICAL CAUTERIZATION |
| Silver nitrate pencil (1-2%) [19,20] | Once | Reduction in pain is observed by day 1 | Argyria, mucocutaneous reactions and tattooing of the mucosa [18] |
| LASERS |
| Nd:YAG (Neodymium-doped yttrium aluminum garnet) laser [21] | Once | Reduction in pain immediately and faster healing | None |
| Carbon dioxide laser [22] | Once | Immediate pain relief | No side effects |
| SYSTEMIC ANTI-INFLAMMATORY AND IMMUNOMODULATORY DRUGS |
| Thalidomide [23] | 100mg, daily orally for 15 days | Complete remission | Headache, xerostomia, lethargy, constipation, contraindicated in pregnancy [14] |
| Colchicine [24] | 0.5mg daily, orally for 3 months | Reduction in number of ulcers and pain | Nausea, diarrhea, paresthesia of lower extremities, myopathy, neuropathy, contraindicated in pregnancy [14, 23] |
| Pentoxifylline [25] | 400mg thrice daily orally | Reduction in size of ulcer | Dizziness, nausea [23] |
| Clofazimine [26] | 100mg daily, orally for 30 days followed by 100mg orally every other day | Increase in ulcer-free intervals | Cutaneous adverse effects [27] |
| SYSTEMIC CORTICOSTEROIDS |
| Prednisone [28] | 25mg daily for 15 days followed by tapering of dose over the next 45 days | Rapid healing and reduction in frequency of the ulcers | Depression, lipodystrophy, hyperglycemia, hypothalamic-pituitary-adrenal axis suppression [3] |
| OTHER SYSTEMIC DRUGS |
| Montelukast [28] | 10mg/day for 1 month and then every other day for 1 month, orally | Resolution of pain and number of ulcers | Headache, cough, influenza, dyspepsia, abdominal pain |
| Dapsone [29] | 100mg daily, orally | Reduction in number duration and in frequency of the ulcers | Anemia, jaundice, haemolysis [23] |
| Zinc sulfate [30] | 150mg, daily, orally for 12 weeks | Reduction in size and number of ulcers | No side effects |
| Doxycycline [31] | 20mg, twice a day, orally | Reduction in days with new ulcers | Headache, dizziness |
| Rebamipide [32] | 100mg, thrice daily, orally for 7-14 days | Reduction in number of ulcers and pain | Nausea, vomiting, constipation, diarrhea. |
Evidence-based treatment: Several studies have been carried out to determine a satisfactory treatment for RAS [14–33]. A reduction in pain associated with oral ulcers was found to be achieved with the help of minocycline mouthwash in a trial by Gorsky M et al., [15] and with the use of silver nitrate pencil by Alidaee MR et al., [20]. Keenan AV et al., [16] noted that the topical application of dexamethasone was able to reduce the size of oral ulcers in addition to pain relief. Fernandes R et al., [18] reported that 5% amlexanox was the only drug which could shorten the healing time and prevent the recurrence of ulcers in RAS. A randomized controlled trial by Tezel A et al., [21] found a better decline in pain level and shorter treatment time with the use of Nd:YAG in patients with recurrent oral ulcers.
Thalidomide was found to be a well-tolerated drug that led to complete remission in most of the patients as studied by Mimura MA et al., [23]. Both colchicine (0.5mg/day) and low-dose-prednisolone (5mg/day) were found to be equally effective in reducing the pain, lesions and recurrence rate associated with RAS in the study conducted by Pakfetrat A et al., [24]. However, side effects like headache, gastric disorders and vertigo were prevalent in the patients taking colchicine. Femiano F et al., [28] found systemic montelukast (10mg/day) to be as effective as prednisone (25mg/day) in the treatment of RAS. As severe side effects were not observed with montelukast, it could be considered for patients requiring treatment for long periods of time. Thornhill MH et al., [25] found that pentoxifylline could be considered in patients who do not respond to other modes of treatment as the degree of improvement noted with pentoxifylline was of a lesser degree. Both dapsone and zinc sulphate were found to have substantial benefits in the control of RAS. However, a faster and more sustained action was observed with only zinc sulfate [30]. The randomized, double-blind, placebo-controlled trial done by Volkov I et al., [33] noted that a daily dose of Vitamin B12 (1000mcg) given sublingually for 6 months brought about a decline in the pain and number of aphthous ulcers in RAS. Evidence from 25 trials was evaluated by a Cochrane review (2012) [27] to determine the effect of systemic therapy in RAS. No single treatment modality was identified to be efficient, and there was inadequate evidence to approve or disregard any particular intervention. Therefore, the best systemic intervention for RAS still remains a matter of debate.
Recent trends in the treatment of RAS: Biologic agents are breaking new ground in the treatment of aphthous ulcers. They block specific pathways associated with the pathophysiology of neoplastic or immune-mediated diseases. These agents have a targeted immunosuppressive or anti-inflammatory action. They also have a pathogenesis-based treatment [34]. Etanercept, adalimumab, infliximab and INF-α were the biologic agents have been found to be used by various investigators for the treatment of RAS.
Etanercept: Etanercept is a recombinant TNF soluble receptor. It is a dimeric fusion protein comprising the extracellular portion of human TNF receptor (p75) coupled to the Fc fragment of human IgG. The binding of TNF to TNF receptors is competitively inhibited by etanercept; thereby preventing TNF-mediated cell responses [35]. It is administered subcutaneously, at a dose of 25mg two times a week [36]. Side effects such as reaction at injection site, allergic reactions, systemic lupus erythematosus, heart failure, risk of lymphoma and tuberculosis reactivation may be seen [34].
A few studies [35,37,38] [Table/Fig-3] have reported the use of etanercept with regard to RAS. All the patients had appreciable improvement in symptoms. Robinson ND et al., administered etanercept in a 50-year-old woman suffering from RAS for 24 years and observed significant improvement within 1 month [35]. The patient’s symptoms recurred after 7 months but with lesser severity, frequency and duration; and the patient did not have to take systemic corticosteroids since the use of etanercept. Ting PT et al., noted that this drug did not appear to raise the mortality or morbidity rates in patients with HIV, therefore etanercept could be considered in the treatment of HIV-associated RAS [39]. Since, etanercept was administered subcutaneously, Hasan A et al., found that this drug could be self-administered if adequate instructions were given to the patient [37]. One investigator recorded an increase in triglyceride level after etanercept therapy [38]. Therefore, a close monitoring of the lipid profile should be done when etanercept is administered and triglyceride-lowering drugs may be indicated if the triglyceride level surpasses 400mg/dl.
Studies depicting effects of etanercept in treatment of RAS.
| STUDY | SUBJECTS | TREATMENT | EFFECTS |
|---|
| Robinson ND et al., (2003) [35] | 50-year-old woman with a 24-year history of RAS. | Etanercept (25 mg twice weekly, subcutaneous). | Significant improvement in RAS within 1 month. |
| Hasan A et al., (2013) [37] | Patients with RAS associated with celiac disease. | Etanercept (25 mg twice weekly, subcutaneous). | Complete remission. |
| Gonzalez-Lopez MA et al., (2013) [38] | A 34-year-old man suffering from RAS since 15-years, unresponsive to treatment. | Etanercept (25mg twice weekly). | Significant clinical improvement seen after 4 weeks of therapy. |
Infliximab: Infliximab is a murine monoclonal antibody acting against TNF-α, an important pathogenic factor of RAS. Infliximab is administered in a dose of 3-5mg/kg intravenously every 2-6 weeks. The adverse effects seen with infliximab include hypersensitivity infections, infusion reaction, serum sickness, hepatitis B reactivation, nausea, dizziness, abdominal pain, urticaria, rash, dry skin, elevated transaminases and risk of lymphoma [34].
Several reports [4,40–44] [Table/Fig-4] have been published on the treatment of recurrent oral ulcers with infliximab. Infliximab was considered because the patients were not responding to conventional treatments. Significant improvement was noted by Travis SP et al., [40], Almoznino G et al., [41], Robertson LP et al., [42], Kaufman I et al., [43], Bañeros-Rojas P et al., [44] and Ryu HJ et al., [4]. In four of these studies [40–44], RAS was associated with BD, while in one study [43], RAS was associated with ulcerative colitis and Crohn’s disease. In the study done by Ryu HJ et al., [4], RAS was not associated with any disease. Infliximab may be an acceptable therapeutic alternative in patients of RAS who are resistant to conventional therapies.
Studies depicting effects of infliximab in treatment of RAS.
| STUDY | SUBJECTS | TREATMENT | EFFECTS |
|---|
| Ryu HJ et al., (2014) [4] | Four patients with recurrent oral ulcers resistant to conventional treatments. | A single dose of infliximab was given to the patients; an additional dose was administered in one patient on demand. | A good response was noted in all patients. The effects of infliximab diminished after a few weeks. However, the ulcers were tolerable and an increase steroids or addition of another medication was not required for about 1 year. |
| Travis S et al., (2001) [40] | Two women with orogenital ulceration associated with Behcet’s disease | For one patient, Infliximab 3mg/kg was given because of an episode of recent sepsis, while in the other 5mg/kg was administered. | Ulcers healed within 10 days. |
| Almoznino G et al., (2007) [41] | 48-year-old woman who had recurrent oral ulcers due to Behcet’s syndrome and was unresponsive to many other medications. | A single dose of Infliximab was given. | Complete remission in the mouth aphthae within 7 days. |
| Robertson LP et al., (2001) [42] | 48-year-old woman who had recurrent oral ulcers due to Behcet’s syndrome and unresponsive to many other medications. | Infliximab 5mg/kg infusion (0, 2 and 6 weeks). | Significant improvement in the oral ulcers was observed after first infusion itself and after the third dose, the patient was completely free from ulcers. |
| Kaufman I et al., (2005) [43] | Patients with Crohn’s disease and Ulcerative colitis. | Infliximab 5 mg/kg infusion. | Aphthous stomatitis completely responded in all patients after a single infusion. |
| Bañeros-Rojas P et al., (2015) [44] | 24-year-old woman with RAS associated with BD. | Infliximab 5mg/kg/day (0-2-6 weeks and every 8 weeks) and methylprednisolone (1 g/24h). | Fast remission. |
Adalimumab: Adalimumab is a human monoclonal antibody that binds to TNF-α resulting in inhibition of the activity of TNF-α. Molecular biology studies have found that adalimumab occupies a substantial area on the antigen-antibody interface of TNF-α, thereby achieving a higher affinity than infliximab or etanercept. It has a half-life of nearly two weeks and may be administered at home as a subcutaneous injection [45]. Adalimumab also has other advantages such as fewer adverse effects resulting in better patient compliance [46]. The treatment regimen varied between researchers. Tanida S et al., [47] administered 160mg adalimumab initially, followed by 80mg after two weeks and 80mg or 40mg every alternate week for 52 weeks; while Perra D et al., [48] administered 40mg of adalimumab every 2 weeks. Since it is a completely humanized drug, the probability of developing neutralizing antibodies is low [49]. Side effects caused by adalimumab include infections (viral, upper and lower respiratory tract), headache, dizziness, injection site reaction, tuberculosis reactivation and risk of lymphomas [34].
A few studies [45,47–49] in which patients have been treated successfully with adalimumab are summarized in [Table/Fig-5]. A favorable response to therapy with adalimumab was observed by Vujevich J et al., [49] and Kaji M et al., [45]. In the study by Tanida S et al., [47], two-thirds of the patients suffering from oral aphthous ulcers were completely symptom-free by the 52nd week, while five of the eight patients with severe aphthous disease in the study by Perra D et al., [48] had been completely healed. Therefore, adalimumab could have significant potential as a novel treatment for severe cases of RAS [49].
Studies depicting effects of adalimumab in treatment of RAS.
| STUDY | SUBJECTS | TREATMENT | EFFECTS |
|---|
| Kaji M et al., (2015) [45] | 13-year-old girl presented with RAS due to BD. | Adalimumab was given subcutaneously (160 mg in week 0, 80 mg in week 2, and 40 mg every other week thereafter). | Resolution of the clinical manifestations and symptoms were observed shortly after the commencement of adalimumab. |
| Tanida S et al., (2015) [47] | Patients with Behcet’s disease. | 160 mg adalimumab initially, followed by 80 mg after two weeks and 80 mg or 40 mg every alternate week for 52 weeks. | Two-thirds of patients with oral ulcers had a complete resolution at week 52. |
| Perra D et al., (2012) [48] | 19 patients with BD of whom 8 had severe aphthous disease. | 40 mg adalimumab was given every 2 weeks, except one patient who was given the drug every 3 weeks. | Complete remission was seen in five of the 8 patients (62.5%) who had severe aphthous disease, while the remaining three cases responded only partially. |
| Vujevich J et al., (2005) [49] | 18-year-old man with a 7-year history of severe major aphthous stomatitis unresponsive to standard therapy. | Adalimumab | Good response |
Recombinant IFN-α: INF-α plays an essential role in the transformation from innate to the adaptive immune response. This transformation is important for the clearance of all foreign antigens and to maintain immunological memory. Treatment with a low dose of INF- α down regulates the infiltration of cells into peripheral lymph nodes and delayed-type hypersensitivity [50].
A few studies [51–56] [Table/Fig-6] have explored the effect of topical [51], oral [52,53] and subcutaneous [54,56] INF-α therapy on oral aphthous lesions. Hamuryudan V et al., [51], Alpsoy E et al., [54] and Hutchinson VA et al., [52] noticed a significant diminution in the number of aphthae without any side-effects. However, there were a few studies which did not find cessation in oral ulcers after INF-α therapy. Karagiannidis I et al., [55] reported an occasional recurrence of oral ulcers while Kötter I et al., [56] noted a response of only 36% in the oral lesions and Kiliç H et al., [53] did not find any beneficial effects on the ulcers after treatment with INF-α. Adverse effects observed with INF-α therapy included influenza-like symptoms, reversible leukopenia and reversible mild alopecia [57].
Studies depicting effects of INF alpha in treatment of RAS.
| STUDY | SUBJECTS | TREATMENT | EFFECTS |
|---|
| Hamuryudan V et al., (1990) [51] | Twenty patients with oral aphthous lesions associated with Behcet’s syndrome (twelve-week open trial). | Topical recombinant IFN-α 2c was applied on the aphthous lesions for four weeks. | Significant decline in the number of aphthae in the post-treatment phase. |
| Hutchinson VA et al., (1990) [52] | Double-blind, placebo-controlled study. | Recombinant human IFN-α 2a was administered orally once a day at a low concentration (1,200 IU/day). | All IFN-α 2a treated patients had complete remission of their aphthae within a 2-week period. The placebo control patients had no change in their condition. |
| Kiliç H et al., (2009) [53] | Eighty-four patients with RAS associated with BD. | Low-dose natural human IFN-α was administered by oral mucosal route. | No beneficial effects. |
| Alpsoy E et al., (2002) [54] | Randomized double-blind placebo-controlled study on 50 patients with BD. | IFN-α -2a, 6 x 10(6) IU was given subcutaneously 3 times per week or placebo for 3 months, and examined clinically at weekly intervals. | IFN-α -2a treatment significantly decreased the pain and duration of oral ulcers. |
| Karagiannidis I et al., (2015) [55] | 37-year-old woman suffering from oral ulcers associated with Adamantiades-Behçet disease. | Longterm interferon-α-2a was given. | Reduction of the clinical manifestations but there was occasional occurrence of oral ulcers. |
| Kötter I et al., (2004) [56] | 50 patients with BD | Recombinant human IFN-α 2a subcutaneous dose of 6 x 10(6) units subcutaneously daily followed by dose reduction. | Only 36% of oral aphthous ulcers responded. |
Very few studies have aimed to find an effective treatment for RAS as a distinct clinical entity. Long-term, multi-centric studies may be required to find an appropriate therapy for this disease. Additionally, since RAS can significantly affect a person’s quality of life, efforts need to be made to bring forth a drug that can prevent recurrences as well.
If RAS is associated with allergies, nutritional deficiency or systemic diseases, these factors should be treated first along with the symptomatic treatment of oral ulcers. The following protocol is being put forth for the treatment of RAS. Topical cauterization using silver nitrate pencil (1%-2%) and use of carbon dioxide laser and Nd:YAG laser is recommended for immediate pain relief. Application of amlexanox 5% paste or topical glucocorticoids 3-4 times a day on each ulcer for 5 days constitute the first line of treatment for RAS as they will help reduce the pain and size of ulcers and promote healing. In addition, amlexanox (5%) will also help to prevent the recurrences of ulcers. Other topical agents that may be used are chlorhexidine and minocycline mouth rinses. If the ulcers are severe or constantly recur, systemic treatment may be required. Systemic prednisolone at a dose of 25mg/day for 15 days followed by tapering of the dose over the next 45 days will promote healing and reduce the frequency of ulcers. Other systemic agents include pentoxifylline, colchicine, dapsone and thalidomide which might be given if not contraindicated.
Conclusion
Elimination of the predisposing factors is of prime importance in the management of RAS. Biologic agents are novel drugs that have been used for the treatment of RAS. These drugs possess the advantage of being able to block specific pathways in the pathophysiology of RAS. However, the high cost and adverse-effects of biologic agents limit the widespread use of these drugs, and they may be used in patients who have none or limited alternatives.
Nevertheless, a definitive treatment protocol for RAS still remains inconclusive. This might be due to the lack of clinical trials and a difference in response between patients. Treatment should primarily aim to provide symptomatic relief and it may vary from person to person.
[1]. Beguerie JR, Sabas M, Recurrent aphthous stomatitis: An update on etiopathogenia and treatmentJ Dermatol Nurses Assoc 2015 7(1):8-12. [Google Scholar]
[2]. Vaillant L, Samimi M, Aphthous ulcers and oral ulcerationsPresse Med (Paris, France: 1983) 2016 45(2):215-26. [Google Scholar]
[3]. Natah SS, Konttinen YT, Enattah NS, Ashammakhi N, Sharkey KA, Häyrinen-Immonen R, Recurrent aphthous ulcers today: a review of the growing knowledgeInt J Oral Maxillofac Surg 2004 33(3):221-34. [Google Scholar]
[4]. Ryu HJ, Seo MR, Choi HJ, Baek HJ, Infliximab for refractory oral ulcersAm J Otolaryngol 2014 35(5):664-68. [Google Scholar]
[5]. Jurge S, Kuffer R, Scully C, Porter SR, Number VI recurrent aphthous stomatitisOral Dis 2006 12(1):1-21. [Google Scholar]
[6]. Akintoye SO, Greenberg MS, Recurrent aphthous stomatitisDental Clinics North Am 2014 58(2):281-97. [Google Scholar]
[7]. Preeti L, Magesh KT, Rajkumar K, Karthik R, Recurrent aphthous stomatitisJOMFP 2011 15(3):252-56. [Google Scholar]
[8]. lebioda Z, Szponar E, Kowalska A, Etiopathogenesis of recurrent aphthous stomatitis and the role of immunologic aspects: Literature reviewArchivum Immunologiae et Therapiae Experimentalis 2014 62(3):205-15. [Google Scholar]
[9]. Albanidou-Farmaki E, Markopoulos AK, Kalogerakou F, Antoniades DZ, Detection, enumeration and characterization of T helper cells secreting type 1 and type 2 cytokines in patients with recurrent aphthous stomatitisTohoku J Exp Med 2007 212(2):101-05. [Google Scholar]
[10]. Taylor J, Glenny AM, Walsh T, Brocklehurst P, Riley P, Gorodkin R, Interventions for the management of oral ulcers in Behçet’s diseaseCochrane Database Syst Rev 2014 9:CD011018 [Google Scholar]
[11]. Ozyurt K, Çelik A, Sayarlıoglu M, Colgecen E, Incı R, Karakas T, Serum Th1, Th2 and Th17 cytokine profiles and alpha-enolase levels in recurrent aphthous stomatitisJ Oral Pathol Med 2014 43(9):691-95. [Google Scholar]
[12]. Tarakji B, Gazal G, Al-Maweri SA, Azzeghaiby SN, Alaizari N, Guideline for the diagnosis and treatment of recurrent aphthous stomatitis for dental practitionersJournal of International Oral Health : JIOH 2015 7(5):74-80. [Google Scholar]
[13]. Wardhana DE, Recurrent aphthous stomatitis caused by food allergyActa Med Indones 2010 42(4):236-40. [Google Scholar]
[14]. Altenburg A, Abdel-Naser MB, Seeber H, Abdallah M, Zouboulis CC, Practical aspects of management of recurrent aphthous stomatitisJ Eur Acad Dermatol Venereol 2007 21(8):1019-26. [Google Scholar]
[15]. Gorsky M, Epstein JB, Rabenstein S, Elishoov H, Yarom N, Topical minocycline and tetracycline rinses in treatment of recurrent aphthous stomatitis: a randomized cross-over studyDermatol Online J 2007 13(2):1 [Google Scholar]
[16]. Keenan AV, Promising results for dexamethasome ointment for treatment of recurrent aphthaeEvid Based Dent 2012 13(3):75 [Google Scholar]
[17]. Meng W, Dong Y, Liu J, Wang Z, Zhong X, Chen R, A clinical evaluation of amlexanox oral adhesive pellicles in the treatment of recurrent aphthous stomatitis and comparison with amlexanox oral tablets: a randomized, placebo controlled, blinded, multicenter clinical trialTrials 2009 10(1):30 [Google Scholar]
[18]. Fernandes R, Tuckey T, Lam P, Allidina S, Sharifi S, Nia D, The best treatment for aphthous ulcers: an evidence based study of the literatureAvailable at: https://www.dentistry.utoronto.ca/system/files/aphthousulcers.pdf. Accessed June 14, 2016 [Google Scholar]
[19]. Altenburg A, El-Haj N, Micheli C, Puttkammer M, Abdel-Naser MB, Zouboulis CC, The treatment of chronic recurrent oral aphthous ulcersDeutsches Ärzteblatt International 2014 111(40):665-673.2014;36:5 [Google Scholar]
[20]. Alidaee MR, Taheri A, Mansoori P, Ghodsi SZ, Silver nitrate cautery in aphthous stomatitis: a randomized controlled trialBr J Dermatol 2005 153(3):521-25. [Google Scholar]
[21]. Tezel A, Kara C, Balkaya V, Orbak R, An evaluation of different treatments for recurrent aphthous stomatitis and patient perceptions: Nd: YAG laser versus medicationPhotomed Laser Surg 2009 27(1):101-06. [Google Scholar]
[22]. Prasad S, Pai A, Assessment of immediate pain relief with laser treatment in recurrent aphthous stomatitisOral Surg Oral Med Oral Pathol Oral Radiol 2013 116(2):189-193. [Google Scholar]
[23]. Mimura MA, Hirota SK, Sugaya NN, Sanches Jr JA, Migliari DA, Systemic treatment in severe cases of recurrent aphthous stomatitis: an open trialClinics (Sao Paulo, Brazil) 2009 64(3):193-98. [Google Scholar]
[24]. Pakfetrat A, Mansourian A, Momen-Heravi F, Delavarian Z, Momen-Beitollahi J, Khalilzadeh O, Comparison of colchicine versus prednisolone in recurrent aphthous stomatitis: A double-blind randomized clinical trialClin Invest Med 2010 33(3):189-95. [Google Scholar]
[25]. Thornhill MH, Baccaglini L, Theaker E, Pemberton MN, A randomized, double-blind, placebo-controlled trial of pentoxifylline for the treatment of recurrent aphthous stomatitisArch Dermatol 2007 143(4):463-70. [Google Scholar]
[26]. de Abreu MA, Hirata CH, Pimentel DR, Weckx LL, Treatment of recurrent aphthous stomatitis with clofazimineOral Surg Oral Med Oral Pathol Oral Radiol Endod 2009 108(5):714-21. [Google Scholar]
[27]. Brocklehurst P, Tickle M, Glenny AM, Lewis MA, Pemberton MN, Taylor J, Systemic interventions for recurrent aphthous stomatitis (mouth ulcers)Cochrane Database Syst Rev 2012 9:CD005411 [Google Scholar]
[28]. Femiano F, Buonaiuto C, Gombos F, Lanza A, Cirillo N, Pilot study on recurrent aphthous stomatitis (RAS): a randomized placebo-controlled trial for the comparative therapeutic effects of systemic prednisone and systemic montelukast in subjects unresponsive to topical therapyOral Surg Oral Med Oral Pathol Oral Radiol Endod 2010 109(3):402-07. [Google Scholar]
[29]. Sharquie KE, Najim RA, Abu-Raghif AR, Dapsone in Behçet’s disease: a double-blind, placebo-controlled, cross-over studyJ Dermatol 2002 29(5):267-79. [Google Scholar]
[30]. Sharquie KE, Najim RA, Al-Hayani RK, Al-Nuaimy AA, Maroof DM, The therapeutic and prophylactic role of oral zinc sulfate in management of recurrent aphthous stomatitis (RAS) in comparison with dapsoneSaudi Med J 2008 29(5):734-38. [Google Scholar]
[31]. Preshaw PM, Grainger P, Bradshaw MH, Mohammad AR, Powala CV, Nolan A, Subantimicrobial dose doxycycline in the treatment of recurrent oral aphthous ulceration: a pilot studyJ Oral Pathol Med 2007 36(4):236-40. [Google Scholar]
[32]. Kudur MH, Hulmani M, Rebamipide: A novel agent in the treatment of recurrent aphthous ulcer and Behcet’s syndromeIndian Journal of Dermatology 2013 58(5):352 [Google Scholar]
[33]. Volkov I, Rudoy I, Freud T, Sardal G, Naimer S, Peleg R, Effectiveness of vitamin B12 in treating recurrent aphthous stomatitis: a randomized, double-blind, placebo-controlled trialJ Am Board Fam Med 2009 22(1):9-16. [Google Scholar]
[34]. Georgakopoulou EA, Andreadis D, Arvanitidis E, Loumou P, Biologic agents and oral diseases—an update on clinical applicationsActa Dermatovenerol Croat 2013 21(1):24-34. [Google Scholar]
[35]. Robinson ND, Guitart J, Recalcitrant, recurrent aphthous stomatitis treated with etanerceptArch Dermatol 2003 139:1259-62. [Google Scholar]
[36]. Altenburg A, Zouboulis CC, Current concepts in the treatment of recurrent aphthous stomatitisSkin Therapy Lett 2008 13(7):1-4. [Google Scholar]
[37]. Hasan A, Patel H, Saleh H, Youngberg G, Litchfield J, Krishnaswamy G, Remission of severe aphthous stomatitis of celiac disease with etanerceptClin Mol Allergy 2013 11:6 [Google Scholar]
[38]. Gonzalez-Lopez MA, Blanco R, Garcia-Ibarbia C, Gonzalez-Vela CM, Gonzalez-Gay MA, Etanercept-induced hypertriglyceridemia during the treatment of recurrent aphthous stomatitisIndian J Dermatol Venereol Leprol 2013 79(3):432-33. [Google Scholar]
[39]. Ting PT, Koo J, Use of etanercept in human immunodeficiency virus (HIV) and acquired immunodeficiency syndrome (AIDS) patientsInt J Dermatol 2006 45(6):689-92. [Google Scholar]
[40]. Travis SP, Czajkowski M, McGovern DP, Watson RG, Bell AL, Treatment of intestinal Behçet’s syndrome with chimeric tumour necrosis factor α antibodyGut 2001 49(5):725-28. [Google Scholar]
[41]. Almoznino G, Ben-Chetrit E, Infliximab for the treatment of resistant oral ulcers in Behcet’s disease: a case report and review of the literatureClin Exp Rheumatol 2007 25(4 Suppl 45):S99-102. [Google Scholar]
[42]. Robertson LP, Hickling P, Treatment of recalcitrant orogenital ulceration of Behçet’s syndrome with infliximabRheumatology (Oxford) 2001 40(4):473-74. [Google Scholar]
[43]. Kaufman I, Caspi D, Yeshurun D, Dotan I, Yaron M, Elkayam O, The effect of infliximab on extraintestinal manifestations of Crohn’s diseaseRheumatol Int 2005 25(6):406-10. [Google Scholar]
[44]. Bañeros-Rojas P, Berrozpe-Villabona C, Peraza-Nieves JE, Díaz-Valle D, Early treatment with infliximab in bilateral occlusive vasculitis as a presenting manifestation of Behçet’diseaseArch Soc Esp Oftalmol 2015 90(6):285-88. [Google Scholar]
[45]. Kaji M, Kishi T, Miyamae T, Nagata S, Yamanaka H, Fujikawa S, Efficacy of adalimumab in a girl with refractory intestinal Behcet’s diseaseCase Reports in Rheumatology 2015 2015:716138 [Google Scholar]
[46]. Ueda A, Takeno M, Ishigatsubo Y, Adalimumab in the management of Behçet’s diseaseTherapeutics and Clinical Risk Management 2015 11:611 [Google Scholar]
[47]. Tanida S, Inoue N, Kobayashi K, Naganuma M, Hirai F, Iizuka B, Adalimumab for the treatment of Japanese patients with intestinal Behçet’s diseaseClin Gastroenterol Hepatol 2015 13(5):940-8.e3 [Google Scholar]
[48]. Perra D, Alba MA, Callejas JL, Mesquida M, Ríos-Fernández R, Adán A, Adalimumab for the treatment of Behçet’s disease: experience in 19 patientsRheumatology (Oxford) 2012 51(10):1825-31. [Google Scholar]
[49]. Vujevich J, Zirwas M, Treatment of severe, recalcitrant, major aphthous stomatitis with adalimumabCutis 2005 76(2):129-32. [Google Scholar]
[50]. Brassard DL, Grace MJ, Bordens RW, Interferon-α as an immunotherapeutic proteinJ Leukoc Biol 2002 71(4):565-81. [Google Scholar]
[51]. Hamuryudan V, Yurdakul S, Serdaroglu S, Tüzün Y, Rosenkaimer F, Yazici H, Topical alpha interferon in the treatment of oral ulcers in Behcet’s syndrome: a preliminary reportClin Exp Rheumatol 1990 8(1):51-54. [Google Scholar]
[52]. Hutchinson VA, Angenend JL, Mok WL, Cummins JM, Richards AB, Chronic recurrent aphthous stomatitis: oral treatment with low-dose interferon alphaMol Biother 1990 2(3):160-64. [Google Scholar]
[53]. Kılıç H, Zeytin HE, Korkmaz C, Mat C, Gül A, Coşan F, Low-dose natural human interferon-α lozenges in the treatment of Behçet’s syndromeRheumatology (Oxford) 2009 48(11):1388-91. [Google Scholar]
[54]. Alpsoy E, Durusoy C, Yilmaz E, Ozgurel Y, Ermis O, Yazar S, Interferon alfa-2a in the treatment of Behcet disease: a randomized placebo-controlled and double-blind studyArch Dermatol 2002 138(4):467-71. [Google Scholar]
[55]. Karagiannidis I, Zouboulis CC, Systemic Adamantiades-Behcet’s disease: adverse effects of an otherwise successful therapy with interferon-α-2aDtsch Med Wochenschr 2015 140(2):112-13. [Google Scholar]
[56]. Kötter I, Vonthein R, Zierhut M, Eckstein AK, Ness T, Günaydin I, Differential efficacy of human recombinant interferon-alpha2a on ocular and extraocular manifestations of Behçet disease: results of an open 4-center trialSemin Arthritis Rheum 2004 33(5):311-19. [Google Scholar]
[57]. Zouboulis CC, Orfanos CE, Treatment of Adamantiades-Behçet disease with systemic interferon alfaArch Dermatol 1998 134(8):1010-16. [Google Scholar]