Understanding the patient’s problem and making an accurate diagnosis is of utmost importance prior to initiating any endodontic treatment. Reproducing the patient’s chief complaint can be challenging and consideration of multiple diagnostic tools like history, clinical examination, radiological examination and advanced diagnostic tests like pulse oximetry and laser doppler flowmetry are essential before arriving at an appropriate clinical judgement [1,2].
A systematic approach in providing endodontic treatment should include proper diagnosis, definitive dental treatment and adjunctive drug therapy, known as the “3D” strategy. Clinicians are encouraged to judiciously prescribe analgesics pre-operatively while considering the drug tactic of the “3D” strategy for the management of the endodontic pain [3].
There are occasions when the practitioner is unable to accurately reproduce the patient’s chief complaint as he/she is already under symptomatic relief after consuming over the counter analgesics at the time of their dental examination. This may prove to be a dilemma for clinicians especially when the response to percussion and palpation tests is inconclusive. In cases, with no positive radiographic findings, it is common for most clinicians to defer the treatment and send the patient home with instructions to return to the dental office once the symptoms have returned. Based on these clinical findings, one may hypothesize that analgesics like ibuprofen and diclofenac when taken pre-operatively, can mask, diminish or eliminate the patient’s symptoms. The impact of these drugs on conventional endodontic testing methods is variable and has not been fully understood [4].
The most prevalent symptom or the primary reason for the patient’s visit to a dental office is acute dental pain. A dental emergency arising from pain due to acute irreversible pulpitis or acute apical periodontitis is one of the most annoying experiences for majority of dental patients.
The most important step in endodontic pain management is the accurate diagnosis of the underlying disease condition through proper history taking and effective use of clinical diagnostic tools. This information should include recording of the chief complaint of the patient detailed medical and dental histories, a thorough clinical examination and relevant diagnostic tests.
In India, Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) such as, Cyclooxygenase (COX)-2 selective inhibitors and opioids are readily available over the counter for the management of acute pain. According to a study conducted by Stoller, Eleanor Palo, Gregg H. Gilbert, 84% of the patients suffering from acute odontalgia reported to have tried some form of self-care strategy before visiting a dental professional [5]. Of the different strategies undertaken, 64% of the patients attempted to relieve their dental pain, with over-the-counter analgesics, which was the most popular method opted by them [6].
The diagnosis of any disease or condition is incomplete, if its cause has not been determined. As observed in routine dental practice, the self administration of analgesics like ibuprofen and diclofenac by patients in pain further clouds the decision making capacity of the clinician by masking the symptoms [4], thus jeopardizing the treatment plan and affecting the treatment outcome.
Hence, the purpose of this double blinded, randomized clinical trial was to evaluate the possible "masking" effect of ibuprofen and diclofenac sodium on endodontic diagnosis using a bite force sensor device – a novel approach.
Materials and Methods
A total of 90 adult patients with symptomatic apical periodontitis within the age range of 18-40 years, who reported to the Department of Conservative Dentistry and Endodontics, College Of Dental Sciences and Hospital, Indore, Madhya Pradesh, India, were assessed for eligibility to participate in the prospective randomized double-blinded clinical trial. The study design was parallel and the data were collected for a period of six months (March 2015 to August 2015).
Inclusion Criteria: Patients with minimum age of 18 years, satisfactory health conditions, a clinical diagnosis of chronic irreversible pulpitis with symptomatic apical periodontitis in only one tooth in the affected quadrant, history of exaggerated lingering response to heat and cold stimulus, moderate or severe pain in a maxillary or mandibular first or second molar [7], no intake of any medications for 12 hours prior to diagnosis.
Exclusion Criteria: Absence of contralateral tooth, sensitivity to percussion in the contralateral tooth, tooth with mobility, persistent use of medication such as steroids and antidepressants (which could alter the pain report), grossly decayed tooth which are not in occlusion, use of NSAIDs in the previous 12 hours and NSAIDs allergy.
Sample size calculation revealed that a minimum of 10 (N) patients per group would be required to detect a significant difference (d) of 100 Newtons in the mean bite force tolerance score of the three groups, at an alpha of 0.05 with power (Z1-β) of 80% and the variance of 81(σ) [sample size formula: N=2(Z1-α/2+Z1-β)2 σ2/d2]. A p-value < 0.05 was considered to indicate statistical significance. Hence, 30 patients were allocated to each group (based on analgesics administrated i.e., ibuprofen, diclofenac sodium and a placebo) and the justification for selecting a large sample size was to avoid any false negative reading and to be able to detect even a minor difference in pain tolerance and to make the results clinically relevant to the people of interest. The sample size selection was in accordance to study conducted by Read et al., who had included 42 patients with pulpitis in their study. Accordingly 90 patients were included in the present study, [4]. Ethical clearance was obtained from the institutional (College of Dental Sciences and Hospital, Rau, Indore, Madhya Pradesh, India) ethical committee (trial registration no. 5013/2016) which was in accordance with the Declaration of Helsinki. The patients were thoroughly informed of the complete procedure and written informed consent was obtained.
All the selected patients had a history of prolonged moderate or severe pain in the affected teeth especially on biting [3]. Both the affected as well as the contralateral teeth (unaffected teeth) of patients were then percussed using a mirror handle to confirm the mechanical allodynia in the involved tooth. Pre-operative radiographs of the involved teeth were recorded to confirm the diagnosis and also to exclude the possibility of proximal caries in the adjacent teeth which are not detectable clinically.
An innovative self designed bite force sensor device was used to measure the mechanical allodynia. This device has two components i.e., a mechanical sensor and a display monitor [Table/Fig-1]. The metallic sensor has two prongs which have a distance of 7mm between them equivalent to the freeway space seen in normal occlusion to avoid any false reading. Average occlusal force recorded in molar region in natural dentition ranges between 300 and 600 newtons [8], therefore the sensor is deviced in such a way as to display readings up to 700 newtons. In this study, the contralateral tooth was used to record the average base line bite force values in individual patients following which the affected tooth was tested and the difference was noted. It was noticed that the patient was unable to bite on the affected side using the same force as in the contralateral tooth. These prongs were wrapped in cotton gauze and were placed on the patients offending tooth. The digital readings obtained by this bite force sensor are then displayed on the digital monitor. While using this device, the patient was instructed to sit erect without any back support to prevent any influence of patient’s posture on the obtained results [Table/Fig-2]. It has a distinct advantage over the conventional bite force transducer device that has been used in previous studies which was fabricated by modifying a tooth slooth. However, this device lacked technical accuracy, recording of the measurements was cumbersome for the operator due to a small digital display and moreover this device required a sustained pressure to produce an accurate measurement [4]. In contrast, the advantage of the bite force sensor device used in this clinical trial is that, if the patient accidentally releases the biting pressure in less than 10 seconds of applying full biting force, then the maximum reading obtained will be maintained at a constant value, and this reading will only increase if the patient applies more pressure than that of the previous reading.
Bite force sensor device containing a metallic sensor and a display monitor.

Recording the bite force tolerance value clinically.

After recording the baseline readings, a trained dental hygienist divided the tablets of each NSAID into three bottles: Ibuprofen 400mg, Diclofenac sodium 50mg and Placebo. The bottles were masked with an opaque label and were randomly assigned as Group A, B and C respectively.
The patients were then randomly divided by the dental hygienist into three groups of 27 patients each and one tablet was given to each one of them [Table/Fig-3].
CONSORT 2010 Flow Diagram.
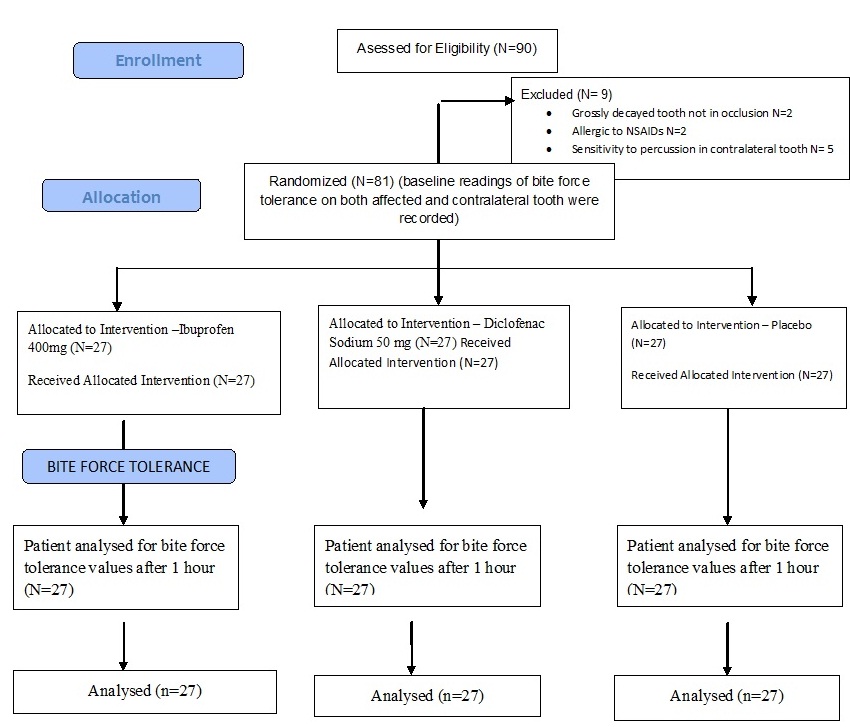
Randomization was achieved using a linear congruential generator by a trained dental hygienist who was unaware of the clinical procedures and only the alphabetical values (i.e., A, B and C) were noted on the data sheets by the dental hygienist to blind the clinical trial. After one hour of oral administration of the tablets, the bite force tolerance values for both contralateral (unaffected) and affected tooth were again recorded following the same procedure as mentioned before.
The data was then uncovered and tabulated by the statistician to summarize the mean average of pre- (before administration of the drug) and post- (1 hour after administration of the drug) bite force tolerance values.
Statistical Analysis
One way ANOVA test was applied to determine the mean pre- and post- bite force tolerance values for all the three groups. Post hoc tukey test was applied to compare the bite force tolerance values between any two groups. Paired t-test was applied to compare mean pre- and post- bite force tolerance values for both affected and contralateral tooth.
Results
The mean pre-bite force values were compared between the three groups on the affected [Table/Fig-4a] as well as the contralateral tooth [Table/Fig-5a] using one-way ANOVA. No statistically significant difference was observed between the values of the affected as well as contralateral tooth using post hoc tukey test, showing that the mean bite force values of the affected [Table/Fig-4b] as well as the contralateral tooth [Table/Fig-5b] was comparable between the three groups.
Table showing pre-bite force tolerance values for all the three groups with respect to affected tooth.
| a) ANOVA Table |
|---|
| Affected tooth bite force tolerance values | Ibuprofen (n=27) | Diclofenac sodium (n=27) | Placebo (n=27) | F value | p-value |
|---|
| Pre-value | 233.48 ±73.79 | 202.00 ±69.08 | 194.44 ± 53.42 | 2.656 | 0.077, NS |
| b) Post-hoc tukey Table |
| Pairs | p value | Significance |
| Ibuprofen – Diclofenac sodium | 0.193 | Not significant |
| Ibuprofen – Placebo | 0.082 | Not significant |
| Diclofenac sodium – Placebo | 0.907 | Not significant |
One-way ANOVA test applied, p-value < 0.05 was taken as statistically significant
Table showing pre-bite force tolerance values for all the three groups with respect to contralateral tooth.
| a) ANOVA Table |
|---|
| Contralateral tooth bite force tolerance values | Ibuprofen (n=27) | Diclofenac sodium (n=27) | Placebo (n=27) | F value | p-value |
|---|
| Pre-value | 497.48 ± 82.10 | 496.63 ± 99.19 | 464.04 ± 61.36 | 1.447 | 0.241, NS |
| b) Post-hoc tukey Table |
| Pairs | p value | Significance |
| Ibuprofen – Diclofenac sodium | 0.999 | Not significant |
| Ibuprofen – Placebo | 0.300 | Not significant |
| Diclofenac sodium – Placebo | 0.319 | Not significant |
One-way ANOVA test applied, p-value < 0.05 was taken as statistically significant
Significant difference in the mean post-bite force values was observed on the affected side [Table/Fig-6a] (p<0.05). The post-hoc tukey test for affected tooth [Table/Fig-6b] revealed that there was a statistically significant difference between the ibuprofen-placebo groups and diclofenac sodium- placebo groups with a higher bite force in ibuprofen group and diclofenac sodium group in comparison to placebo group. However, there was no statistically significant difference in the mean bite force tolerance values between the ibuprofen sodium group (p>0.05) in the affected tooth.
Table showing post-bite force tolerance values for all the three groups with respect to affected tooth.
| a) ANOVA Table |
|---|
| Affected tooth bite force tolerance values | Ibuprofen (n=27) | Diclofenac sodium (n=27) | Placebo (n=27) | F value | p-value |
|---|
| Post value | 364.96 ± 76.57 | 332.19 ± 64.42 | 196.11 ± 55.96 | 49.404 | <0.001* |
| b) Post-hoc tukey Table |
| Pairs | p value | Significance |
| Ibuprofen – Diclofenac sodium | 0.170 | Not significant |
| Ibuprofen – Placebo | <0.001* | Significant |
| Diclofenac sodium – Placebo | <0.001* | Significant |
One-way ANOVA test applied, p-value < 0.05 was taken as statistically significant
The mean post bite force values were compared between the three groups on the contralateral tooth [Table/Fig-7a] using one-way ANOVA. No statistically significant difference was observed between the values of the contralateral tooth using post hoc tukey test, showing that the mean bite force values of the contralateral tooth [Table/Fig-7b] was comparable between the three groups.
Table showing post-bite force tolerance values for all the three groups with respect to contralateral tooth.
| a) ANOVA Table |
|---|
| Contralateral tooth bite force tolerance values | Ibuprofen (n=27) | Diclofenac sodium (n=27) | Placebo (n=27) | F value | p-value |
|---|
| Post-value | 498.89 ± 92.47 | 498.19 ± 101.13 | 466.11 ± 62.48 | 1.252 | 0.292 |
| b) Post-hoc tukey Table |
| Pairs | p value | Significance |
| Ibuprofen – Diclofenac sodium | 1.000 | Not significant |
| Ibuprofen – Placebo | 0.354 | Not significant |
| Diclofenac sodium – Placebo | 0.369 | Not significant |
One-way ANOVA test applied, p-value < 0.05 was taken as statistically significant
Paired t-test was applied to compare the mean bite force values before and after analgesia of the affected tooth [Table/Fig-8], and it revealed that there was a statistically significant difference in mean bite force values after administering analgesia (p<0.05), with a higher mean bite force tolerance after administration of analgesia. However, no statistically significant difference was seen in placebo group (p>0.05).
Table showing comparison of mean bite force before and after analgesia of the affected side among the three groups.
| Group | Before analgesia(Mean±SD) | After analgesia(Mean±SD) | ‘t’ value, df | p-value |
|---|
| Ibuprofen | 233.48 ±73.79 | 364.96 ±76.57 | -17.594, df=26 | <0.001* |
| Diclofenac sodium | 202.00 ± 69.08 | 332.18 ±64.41 | -12.876, df=26 | <0.001* |
| Placebo | 194.44 ± 53.42 | 196.11 ±55.96 | -1.589, df=26 | 0.124, NS |
Paired ‘t’ test applied, p-value < 0.05 was taken as statistically significant
Paired t-test was applied to compare the mean bite force values before and after analgesia of the contralateral tooth [Table/Fig-9], and it revealed that there was no statistically significant difference in mean bite force values after administering analgesia (p>0.05), showing that the mean bite force values of the contralateral tooth before and after analgesia was comparable between the three groups.
Table showing comparison of mean bite force before and after analgesia of the affected side among the three groups.
| Group | Before analgesia(Mean±SD) | After analgesia(Mean±SD) | ‘t’ value, df | p-value |
|---|
| Ibuprofen | 497.48 ± 82.10 | 498.89 ± 92.47 | -0.252, df=26 | 0.803, NS |
| Diclofenac sodium | 496.63 ± 99.19 | 498.19 ± 101.13 | -0.544, df=26 | 0.591, NS |
| Placebo | 464.04 ± 61.36 | 466.11 ± 62.48 | -1.166, df=26 | 0.254, NS |
Paired ‘t’ test applied, p-value < 0.05 was taken as statistically significant
Discussion
As observed in routine clinical dentistry, self care strategies adopted by patients before visiting a dental office could affect the conventional approach of the clinician in arriving at a definitive diagnosis, as the symptoms may be camouflaged by the analgesics consumed. One of the preliminary reason or the urgent need to consume an analgesic is an acute dental pain experienced by the patient especially on biting due to mechanical allodynia frequently associated with apical periodontitis [9].
Patients presenting with irreversible pulpitis or symptomatic apical periodontitis frequently experience mechanical allodynia associated with the affected tooth and its incidence was found to be 57.2%. The progression of the inflammation from the pulp into the apical periodontal ligament fibres may be attributed as the primary reason for aggravation of pain on biting [9].
According to a study conducted by, Torabinejad and Walton, the effect of analgesics on endodontic diagnosis was analyzed using electric pulp tester, it was observed that the results obtained using this device were not consistent and reliable. This can be attributed to the fact that the electric pulp tester only indicates the neural transmission of vital nerve fibers and does not measure the health or integrity of the pulp [2].
The search for a reliable device to actually identify and understand the masking effects of analgesics on endodontic diagnosis has eluded the researchers till date. This exploration led to the designing of an innovative bite force sensor device in the Department of Endodontics (College of Dental Sciences and Hospital, Indore, Madhya Pradesh, India) which was based on the principle of recording mechanical pain threshold values (pain perception due to widened periodontal ligament space during biting) and using it as a parameter to compare the masking effect of analgesics.
This newly designed bite force sensor apparatus was seen to display more accurate and precise results using a more simplified technique when compared to the previously fabricated bite force transducer [4]. Also this device was fabricated to overcome the errors which may arise due to lack of maintenance of sustained pressure on the sensor by the patient during the required period of time (10 secs). In addition, it measures the readings up to a range of 700N which is equivalent to that observed in normal occlusion.
Administration of both the analgesics (ibuprofen and diclofenac sodium) significantly improves the bite force tolerance (p<0.05), thus confirming the masking effect of these analgesics on endodontic diagnosis which is in accordance with study conducted by Read et al., [4].
The drugs (ibuprofen and diclofenac) used for the study have been selected keeping in mind that these analgesics are the more commonly self administered drugs readily available over the counter in India [10]. They have the ability to significantly suppress local production of Prostaglandins (PG’s). The reduction in peripheral inflammatory mediators may be responsible for the analgesic effect which may jeopardise the endodontic diagnosis.
Diclofenac sodium which is a benzoic acid derivative, inhibits the thromboxane-prostanoid receptor, affects arachidonic acid release and uptake, inhibits lipoxygenase enzymes, and activates the nitric oxide–cGMP anti-nociceptive pathway thereby reducing the pain sensation [11]. On the other hand, ibuprofen is a non-selective inhibitor of cyclooxygenase, which is an enzyme that also uses the arachidonic acid pathway for the synthesis of PG’s [12].
Both these NSAIDS have a fast onset of action and reach their peak plasma concentrations within 45 minutes, causing a potent analgesic action thus, efficaciously relieving pain [13]. Hence, they were compared for their masking effect after one hour of oral administration.
There was no statistically significant difference in the analgesic efficacy of ibuprofen and diclofenac sodium on comparing the post-bite force tolerance values between the two groups, this is in accordance to previously conducted study by Komali G, who compared their analgesic efficacy (i.e., onset of action, time to reach its peak effect, duration of action) and concluded that both diclofenac as well as ibuprofen showed similar results in masking the symptoms of pain with respect to affected tooth [14].
Future perspective: Over the counter analgesics are readily available in India which is randomly used and abused by dental patients to achieve immediate relief in cases of symptomatic apical periodontitis. This often proves to be a major obstacle for the clinician in arriving at a conclusive diagnosis in such cases. This novel bite force sensor device can be a major breakthrough in overriding this hurdle and hence may be included in future as a part of routine armamentarium used for modern endodontic diagnosis. On further advancements, this bite force sensor device can be made more compact and easy to use, and it should be helpful to differentiate between the acute and chronic phases of pulpal inflammation.
Limitation
This bite force sensor device has certain limitations. It only provides the status of periodontally involved tooth and does not clearly differentiate between the acute and chronic phases of pulpal inflammation. Also, this device can be used only as an adjunctive tool and should be verified with the help of other diagnostic tests before arriving at a final diagnosis.
Conclusion
Within the limitations of the present study, it may be concluded that this self designed bite force sensor may serve effectively in arriving at a definitive diagnosis in teeth with chronic irreversible pulpitis with symptomatic apical periodontitis, where the alloydynia has been camouflaged by the use of over the counter analgesics like ibuprofen & diclofenac sodium. Although this device has exciting research potential, further clinical trials need to be conducted to establish this device as a routine diagnostic tool in modern endodontic practice.
One-way ANOVA test applied, p-value < 0.05 was taken as statistically significant
One-way ANOVA test applied, p-value < 0.05 was taken as statistically significant
One-way ANOVA test applied, p-value < 0.05 was taken as statistically significant
One-way ANOVA test applied, p-value < 0.05 was taken as statistically significant
Paired ‘t’ test applied, p-value < 0.05 was taken as statistically significant
Paired ‘t’ test applied, p-value < 0.05 was taken as statistically significant