Continuous Ambulatory Peritoneal Dialysis Catheter Tunnel Breakdown and its Repair
Shantajit Nameirakpam1, Salinita Naorem2, Chetan Maibam3, Sharatkumar Singh Naorem4
1 Senior Resident, Department of Urology, Regional Institute of Medical Sciences, Imphal, Imphal West, Manipur, India.
2 Junior Resident, Department of Microbiology, JNIMS, Imphal, Imphal West, Manipur, India.
3 Assistant Professor, Department of Surgery, Regional Institute of Medical Sciences, Imphal, Imphal West, Manipur, India.
4 Professor, Department of Nephrology Unit, Regional Institute of Medical Sciences, Imphal, Imphal West, Manipur, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Shantajit Nameirakpam, Senior Resident, Department of Urology, Regional Institute of Medical Sciences, Imphal, Imphal West, Manipur, India.
E-mail: shantajit@gmail.com
Chronic kidney disease, Complication, Subcutaneous tissue breakdown
Dear Editor,
Continuous Ambulatory Peritoneal Dialysis Catheter (CAPD) tunnel breakdown is a very rare complication and has not been reported previously. Some of the rare complications like intraperitoneal fracture of the catheter [1], channel perforation and aneurysm [2] of the CAPD catheter have been reported. We hereby report two cases of CAPD tunnel breakdown and its repair under local anaesthesia.
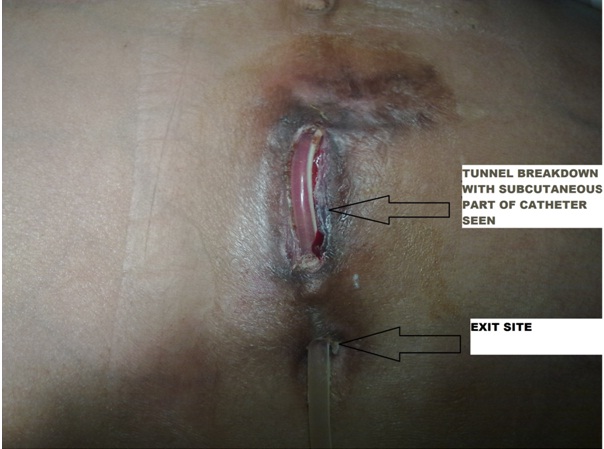
Case-1: A 56-year-old female who had CAPD catheter implantation two months back with chronic kidney disease associated with diabetes mellitus type 2 and hypertension presented with tunnel skin and subcutaneous tissue breakdown [Table/Fig-1]. She was having persistent pus discharge from the catheter exit site before the tunnel breakdown.
Catheter tunnel breakdown.
Case-2: A 60-year-old male who had CAPD catheter implantation four months back with chronic kidney disease associated with hypertension presented with the same features as in Case 1.
Management: Both the CAPD catheters were inserted by right paramedian incision at the level of the umbilicus. The repair was taken up under local anaesthesia. The skin and the subcutaneous tissue were completely freshened [Table/Fig-2] and the catheter was buried under the freshened skin and subcutaneous tissues [Table/Fig-3]. Subcutaneous tissues were repaired with polyglactin 2-0 suture and skin with 2-0 silk sutures. Sutures were removed after 10 days and wound was healthy.

Repair burying catheter in subcutaneous tunnel.

CAPD catheter tunnel breakdown is very rare and it is associated with infection of the tunnel. The tunnel repair is easy and straight forward. Due to rarity of such cases, many case reports have not been published.
[1]. Chang Y C, Lee K H, Chen T H, Tsai P J, Chen P Y, Guo M C, A case of intraperitoneal fracture of a double-cuff Tenckhoff catheterPerit Dial Int 2014 34(1):132-34. [Google Scholar]
[2]. Singh SK, Singh DV, Jha V, Sakhuja V, Partial reimplantation of Tenckhoff catheter for channel perforation and aneurysm: A case seriesIndian J Urol 2013 29(2):133-35. [Google Scholar]